Responses

Other responses
Jump to comment:
- Published on: 13 December 2019
- Published on: 29 November 2019
- Published on: 12 November 2019
- Published on: 13 December 2019In reply to the authors' response to "Concerns regarding the inference that EDS is not rare"
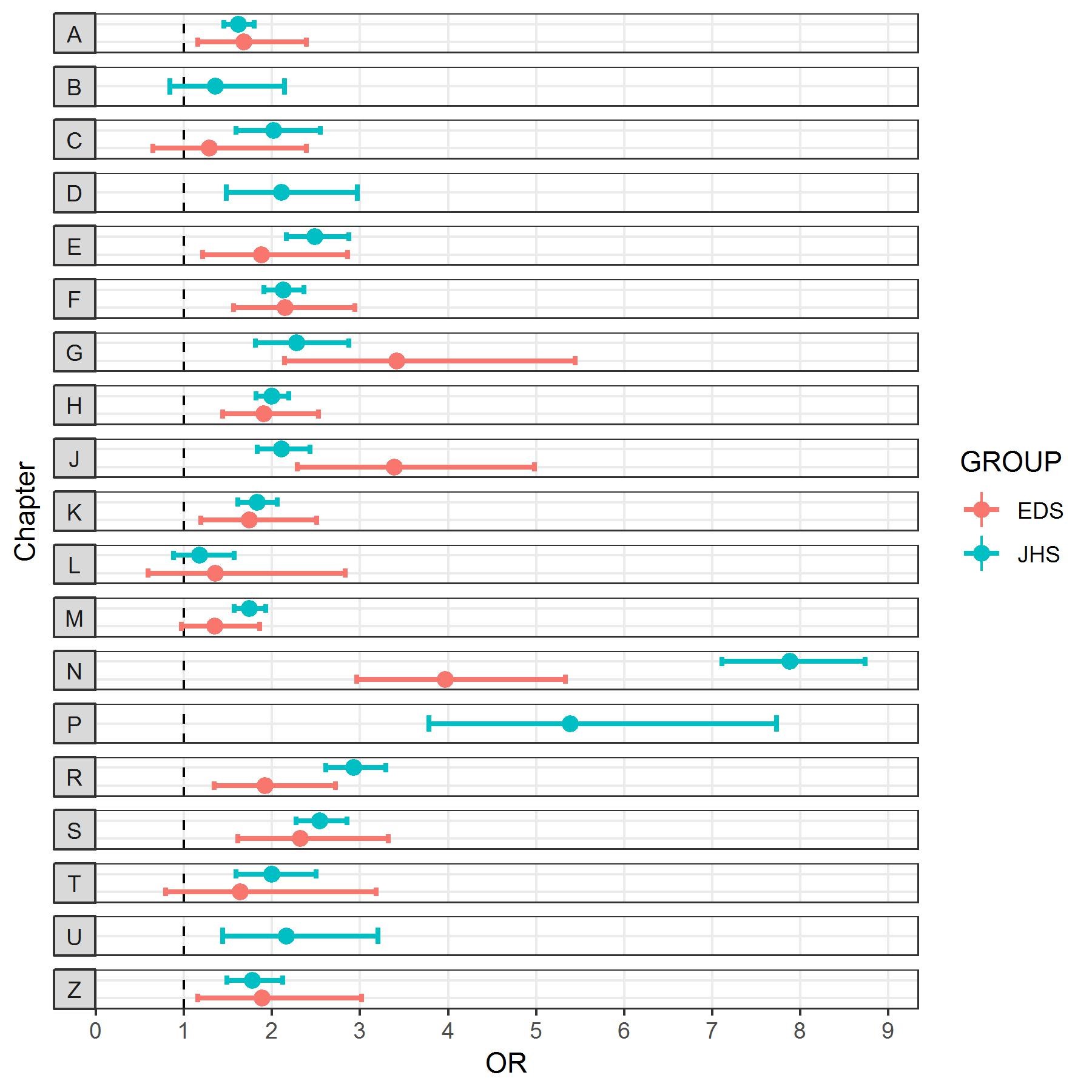
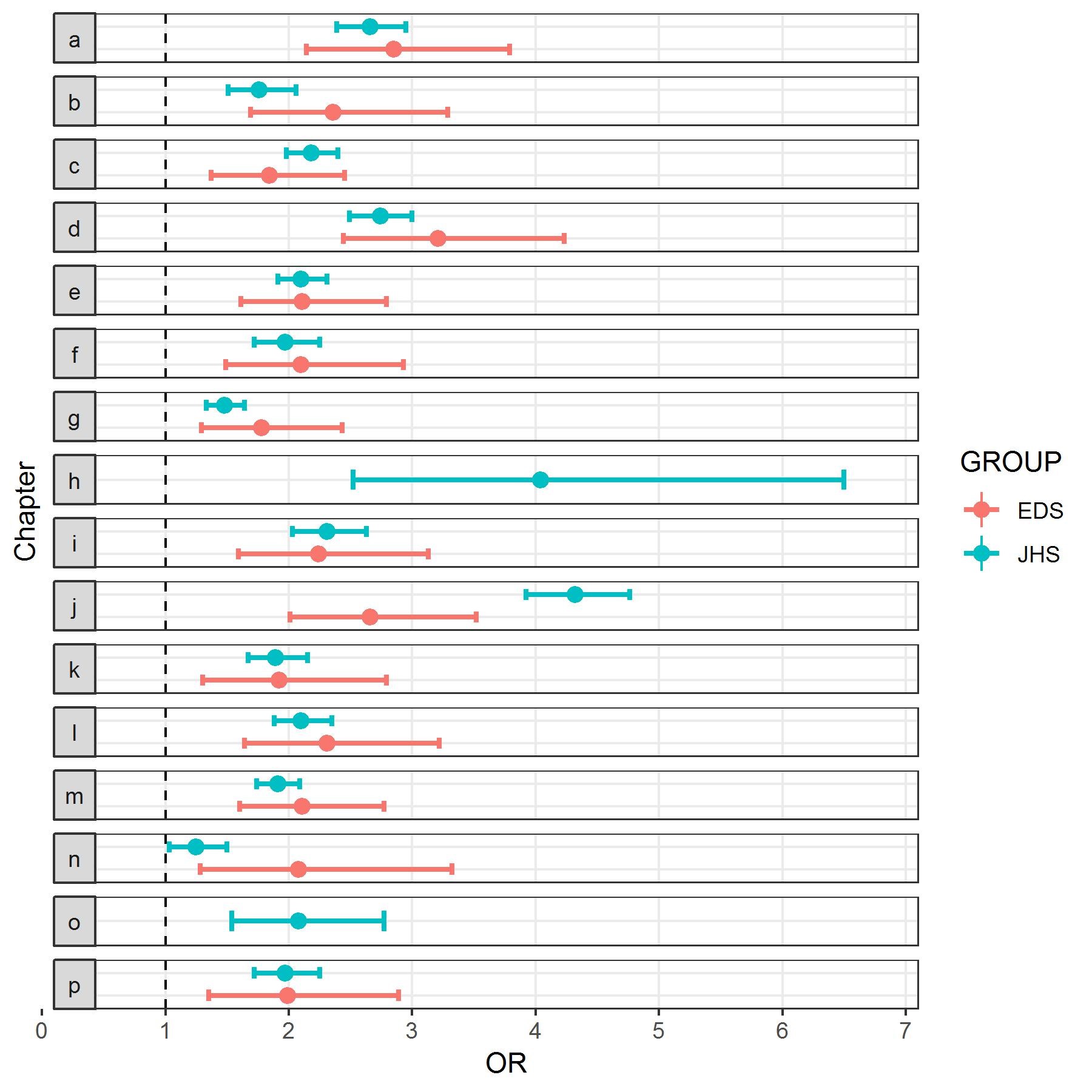
We thank Demmler and colleagues for their reply to our concerns (dated 29th November 2019). In particular we appreciate the analysis required to demonstrate that the Joint Hypermobility Syndrome (JHS) and Ehlers-Danlos syndromes (EDS) cohorts in their study shared similar characteristics across the 35 Read chapter categories. This is a valuable observation of itself.
Demmler and colleagues say in their reply that we ‘asserted that diagnosed JHS is known to be common’. We assume they have misconstrued our opening comments about combining common with rare conditions. We used the words ‘common’ and ‘diagnosed JHS’ to describe their findings, and based on the prevalence of ‘diagnosed JHS’ in the population they studied. We recognise that this study is the first to directly report a healthcare record-based population prevalence for JHS and a healthcare record-based population prevalence for EDS.
We read that the authors agree with our comments that it is not possible to know what proportion of people who met the Brighton criteria for JHS also meet the 2017 hEDS criteria, and, that the authors agree that further studies are required to determine how common hypermobility spectrum disorder (HSD), hypermobile EDS (hEDS), and other forms of EDS are.
We appreciate that the authors did not “seek to remove the protected ‘rare’ status from all subtypes of EDS”, and that they “regret if their work has been misquoted on social media”. Demmler et al. also reply that...
Show MoreConflict of Interest:
None declared. - Published on: 29 November 2019Reply to “Concerns regarding the inference that EDS is not rare"
We would like to thank Hakim et al for the opportunity to continue the debate around the prevalence and definitions of conditions associated with joint hypermobility. Coming to anything like a true population prevalence for these conditions is still a long way off due to both the huge under-diagnosis (1) and ongoing evolution of the clinically-based criteria (2-4) and terminology for patients who do not have one of the known genetic mutations for classical, vascular or the other so-called rare subtypes of Ehlers-Danlos Syndrome (EDS).
Hakim et al assert in their letter that diagnosed Joint Hypermobility Syndrome (JHS) is known to be ‘common’. We have searched the literature for reported whole population prevalence rates for JHS and have been unable to find any. Therefore our paper is the first to report a diagnosed prevalence for this condition, although this figure can also be derived for the population of Sweden, as we pointed out in our work. (5)
We completely agree with the letter’s authors that at this point in time it is not possible to know what proportion of people who met the Brighton Criteria for JHS also meet the 2017 hEDS criteria. We hope further research may reveal this data in the future. What we can say, however, is that for the decade or so prior to 2017, experts in the field considered JHS and EDS-HT to be clinically indistinguishable (1, 6-10), indeed many clinicians used the term JHS/EDS-HT in correspondence in recognition of this. Indeed,...
Show MoreConflict of Interest:
None declared. - Published on: 12 November 2019Concerns regarding the inference that EDS is not rare
Dear Sir or Madam
Re. Diagnosed prevalence of Ehlers-Danlos syndrome and hypermobility spectrum disorder in Wales, UK: a national electronic cohort study and case-control comparison.
Demmler J C, Atkinson M D, Reinhold E, Choy E, Lyons R A, Brophy S T
BMJ Open 2019;9:e031365We write concerning the paper by Demmler et al., published in BMJ Open. We wish to raise the following concerns:
1. With regard to combining the Joint Hypermobility Syndrome (JHS) and Ehlers-Danlos syndromes (EDS) populations for analysis.
If one combines data from a cohort that is found to be ‘common’ (in this case ‘diagnosed JHS’) with one that is found to be ‘rare’ (in this case ‘diagnosed EDS’), the new combined cohort (i.e. diagnosed JHS/EDS) will be common. To then consider the rare cohort common is a fallacy.
Also, although individuals in a population with a previous diagnosis of JHS (i.e. prior to the 2017 international classification (1,2)) might have Hypermobile EDS (hEDS) by the current classification, it is not known how JHS segregates into Hypermobility Spectrum Disorder (HSD) and hEDS. A JHS population would need to be reassessed to confirm this, or modelling assumptions of the data would need to be applied.
Show More
In addition, it is not known what proportion of the EDS cohort have hEDS versus the rare Mendelian types of EDS. As such, there is no way of knowing whether or by what proportion the two cohorts represent the same or similar or dif...Conflict of Interest:
None declared.
{kind=link}
{kind=link}
{kind=link}
{kind=link}