Article Text

Abstract
Introduction Difficult airway management during tracheal intubation can lead to severe hypoxic sequelae. Routine intubation practice is to use a strict supine position, whereas a 25° head-up or reverse Trendelenburg position increases efficacy of preoxygenation, seems more comfortable for the anaesthetist and may also provide better intubation conditions in direct laryngoscopy. The 25° head-up position could be used for the whole population rather than only for obese patients, but there is no prospective randomised controlled trial with a robust design and large number of patients comparing strict supine against 25° intubation in operating room. The objective of the InSize25 study is to test the effect of these two patient positions on intubation conditions during laryngoscopy in scheduled surgery on non-obese patients.
Methods and analysis InSize25 is an investigator-initiated, multicentre, open-label, two-arm, randomised controlled trial. The InSize25 study will randomise 1000 adult patients scheduled for surgery under general anaesthesia requiring intubation with neuromuscular-blocking drugs, candidates for direct laryngoscopy. The primary outcome variable is the view obtained during the first laryngoscopy without any external manipulation assessed using percentage of glottic opening. Important secondary outcomes are: Cormack-Lehane classification, number of attempts at laryngoscopy and at tracheal intubation, use of ancillary equipment (eg, bougies, alternative laryngoscope blades, videolaryngoscope) and manoeuvres (eg, laryngeal manipulation), comfort score for the anaesthetist, episodes of postinduction hypotension or desaturation and mechanical complications of intubation.
Ethics and dissemination The trial received appropriate approval from the ‘CPP Sud-Est II’ ethical review board. Informed consent is required. If the 25° head-up position proves superior for tracheal intubation without more complications, it may become the routine-standard intubation position rather than only for use with obese patients. The final results will be published in a peer-reviewed journal.
Trial registration number Clinicaltrials.gov identifier (NCT03339141).
- anaesthetics
- intubation
- laryngoscopy
- glottis
- view
- 25° head-up position
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
First prospective randomised controlled study with a robust design and large number of patients which compares the 25° head-up position against supine position for routine tracheal intubation for scheduled surgery in non-obese patient in operating room.
Primary endpoint measure is percentage of glottic opening score, which is more relevant, more accurate, as it has less interindividual and intraindividual variability than Cormack-Lehane grades.
The study also uses a comfort score for the anaesthetist, to capture the subjective experience of the intubation position.
The main limitation of the InSize25 trial is its unblinded design with a self-reported primary outcome. However, the trial remains pragmatic, with direct laryngoscopy chosen as standard care to ensure better feasibility among multiple centres and with anaesthetist-led stratification of the randomisation to limit the bias.
Introduction
Background and rationale
Since the advent of tracheal intubation in anaesthesia, anaesthetists have feared airway complications as they can occur even under elective conditions and require immediate management to avoid severe hypoxic sequelae. Fortunately, as shown in several reviews, the frequency of these complications is decreasing fast. This decrease was first highlighted in an epidemiology review published in Anesthesia by Auroy et al in 20091 and confirmed by Cook et al in 2011 in a British Journal of Anaesthesia 2 paper reporting a low incidence of airway management-related cerebral anoxia and death. However, there is still room for improvement.
Tracheal intubation, especially in the operating room, has always been traditionally performed in a strict supine position. It has been found in the general population and especially in obese patients that preoxygenation in the 25° head-up or reverse Trendelenburg position leads to better efficacy of preoxygenation and longer apnoea time before oxygen desaturation.3–6 This position appears to offer a good compromise between optimisation of respiratory function (by elevating the head and thus improving functional residual capacity) and maintenance of haemodynamic stability. It may partially limit gastro-oesophageal reflux. Moreover, this position seems to be more comfortable for the intubating anaesthetist, putting less stress on his or her back as it requires less cervical flexion and helps develop greater force of traction for the same muscular effort.7 8 The 25° head-up position would also provide better intubation conditions in direct laryngoscopy. A Korean randomised crossover study published in 2007 by Lee et al found better intubation conditions in 40 patients in the 25° head-up position compared with the supine position.8 An external anaesthetist, blinded to the patient’s position, determined the intubation score. In 2016, Reddy et al published a ‘before-versus-after’ study on 781 patients and found no difference in glottic views, but the use of external laryngeal manoeuvres such as backwards upwards rightward pressure was significantly less frequent in the 25° head-up group.9 None of the studies comparing these two positions, whether on oxygenation or intubation conditions, has found any difference in terms of haemodynamic or mechanical complications,3 5 6 8 and when using a rescue device like videolaryngoscopy, the head-up position is just as functional as the supine position.10
As intervention tables are become increasingly manageable, and as direct laryngoscopy remains the most common intubation technique,11 we wondered whether it is time to stop and challenge the ‘standard’ intubation position, that is, strict supine, which is widely used in the absence of risk factors. The 25° head-up position could be used for the whole population, rather than only for obese patients (as recommended by the profession’s lead organisation12), leading to a better combination of oxygenation, patient and anaesthetist comfort, optimal laryngeal exposure conditions and a suitable position for performing a passive leg raising test after induction. To the best of our knowledge, there is no prospective randomised controlled trial with a robust design and large number of patients which compares strict supine intubation against 25° intubation. The objective of the InSize25 study is to test the effect of the patient’s position (strict supine or 25° head-up or reverse Trendelenburg) on intubation conditions during laryngoscopy in scheduled surgery on non-obese patients.
Objectives
Primary objective
The primary objective of the study is to determine the effect of patient position (strict supine vs 25° head-up position) on laryngoscopic intubation conditions in scheduled surgery.
Secondary objectives
Secondary objectives of InSize25 are: to test the impact of the strict supine position on the anaesthetist’s comfort during the procedure and the medical devices required to support tracheal intubation; to determine the patient’s tolerance of the position during the procedure; to analyse the relationship between intervention-table height set by each anaesthetist and the anaesthetist’s size; to compare mechanical complications of the direct laryngoscopy procedure.
Trial design
The InSize25 trial is an investigator-initiated, open-label, multicentre, two-arm, randomised controlled trial.
CONSORT diagram
Figure 1 shows the Consolidated Standards of Reporting Trials (CONSORT) diagram of the InSize25 study.

Consolidated Standards of Reporting Trials diagram of the Insize25 trial (comparison of intubating conditions in 25° head-up position vs strict supine position) illustrating the randomisation and flow of patients in the study.
Methods: participants, interventions and outcome
This manuscript was written in accordance with the Standard Protocol Items: Recommendations for Interventional Trials guidelines.13
Study setting
The InSize25 trial involves a total of seven centres in France (Clermont-Ferrand, two university hospitals and one private clinic), Paris (Saint-Louis University Hospital), Moulins, Villefranche-sur-Saone and Alpes-Leman Hospitals.
Eligibility criteria
Inclusion criteria
All adult patients with social security coverage, scheduled for surgery under general anaesthesia, requiring intubation with neuromuscular-blocking drugs, are candidates for direct laryngoscopy. All the anaesthetists participating in the study will select all the patients requiring direct laryngoscopy under neuromuscular-blocking drugs according to standard practice who meet the inclusion criteria.
Exclusion criteria
Patients meeting one or more of the following criteria are not included:
Emergency surgery.
Patients requiring rapid sequence induction of anaesthesia.
Patients who were recognised as having difficult airways where an alternative method of intubation (eg, fibre optic) was the method of choice.
Patients who were scheduled for outpatient surgery (due to the period of reflection prior to participation; ethical considerations).
Patients with epilepsy.
Severe cardiovascular/pulmonary disease.
Patients with mask phobia.
Patients with a body mass index (BMI) >30 kg/m².
Patient refusal.
Patients less than 18 years old.
Pregnant women.
Patients who were deemed unfit to give consent.
Patients requiring rapid sequence induction of anaesthesia will be excluded to enhance homogeneity of induction type and because some anaesthetists will be reluctant to intubate patient on a rapid sequence induction with a 25° interventional position or in the strict supine position according to the anaesthetist.
Interventions
Patients eligible for inclusion will be randomly assigned to the 25° interventional group (head-up when the operating table can accommodate it, or reverse Trendelenburg if not) or to the reference group (strict supine) (figure 2). During the three phases of tracheal intubation, preoxygenation, induction to initiation of laryngoscopy and initiation of laryngoscopy, patient will be placed in the position allocated until successful intubation. Then the position will be changed as surgery needed.

Different positions possible between the two groups of the InSize25 trial.
In the 25° interventional group, two positions will be allowed: preferably 25° head-up position (lower half parallel to floor, upper half at 25° angle to floor) and if intervention table will not allow it, the alternative reverse Trendelenburg position (upper and lower half at 25° to floor). The right angulation of the operating table in the interventional group 25° will be checked with a smartphone application such as ‘niveau’, ‘niveau iHandy’ measuring angulation between upper half table and lower half of the table or the floor if reverse Trendelenburg. Four different smartphone applications were tested with four different smartphones and found only a maximum of 0,1° difference between each measurement. In the reference group, patients will be positioned in supine position: both upper and lower half of table are parallel to floor.
In both groups, the positioning of the head and neck will be up to anaesthetist incharge. The use of pillow or sheets to help adjust the patient’s head in sniffing position will be recorded but no instructions will be given to specify for neck and head position to be closer to daily practice.
Choice of anaesthetic type, agents and monitoring will be left to the anaesthetist’s discretion (following the standard care guidelines and routine protocols of each participating centre), but use of a neuromuscular-blocking drug, use of a size 3 or 4 Macintosh blade, and operating-table position are required protocol.
Only senior anaesthetists will intubate patients. Their anaesthetist’s experience: number of senior practice and type of activities (operating room only or mixed with critical care units or emergency units) will be recorded.
Patient demographics (age, sex, height, weight, BMI, criteria for difficult intubation, surgical details and relevant comorbidities), preoxygenation management (used positive end expiratory pressure or non-invasive ventilation and fraction of exhaled oxygen (FeO2) at the time of induction), drugs used for induction and maintenance of general anaesthesia (sevoflurane, desflurane or propofol), smartphone-measured operating-table angulation, monitoring on neuromuscular-blocking drug action, height of the anaesthetist and height of the patient on the table will be collected.
After two unsuccessful attempts at direct laryngoscopy, the anaesthetist is left to decide on appropriate airway management following the standard care guidelines and routine protocols of each participating centre.
Outcomes
Primary outcome measures
The primary outcome variable is the view obtained during the first laryngoscopy without any external manipulation assessed using percentage of glottic opening (POGO) score14 as calculated by the anaesthetist performing the laryngoscopy. A POGO score of 100% corresponds to a complete visualisation of the glottic opening, from the anterior curvature of the vocal cords to the inter-arytenoid node between the posterior cartilages.
Secondary outcome measures
The secondary outcomes are: Cormack-Lehane classification (Cormack and Lehane grade I is equivalent to a POGO score of 100%, Cormack and Lehane grade III is equivalent to a POGO score of 0%), number of attempts at laryngoscopy and at tracheal intubation, use of an ancillary equipment (eg, bougies, alternative laryngoscope blades, videolaryngoscope) and manoeuvres (eg, laryngeal manipulation) applied at the anaesthetist’s discretion. A numerical-scaled comfort score for the anaesthetist (from 0 very uncomfortable to 10 optimal, really comfortable position) will be recorded. Episodes of post-induction desaturation (pulse oximetry value SpO2 <90%) or hypotension (mean arterial pressure <65 mm Hg or 20% decrease from base value of systolic arterial pressure up to 20 min after anaesthetic induction) and mechanical complications of intubation (laryngeal pain, cough, hoarseness, trauma) up to 2 hours after withdrawal of the breathing tube will be recorded. Management of induction complications such as haemodynamic instability or hypoxaemia is left to the anaesthetist. The data non-related to glottis view will be collected by anaesthesia team participating to the process (anaesthesia resident or nurse).
Patient and public involvement
Patients and public were not involved in the development of the research question and outcome measures because it was judged not applicable. As the two positions are well-known and usual routine positions, it is the regular healthcare and vigilance provisions that apply for this type of study.
Study participants will be able to find the results in the scientific literature but they will not be directly contacted.
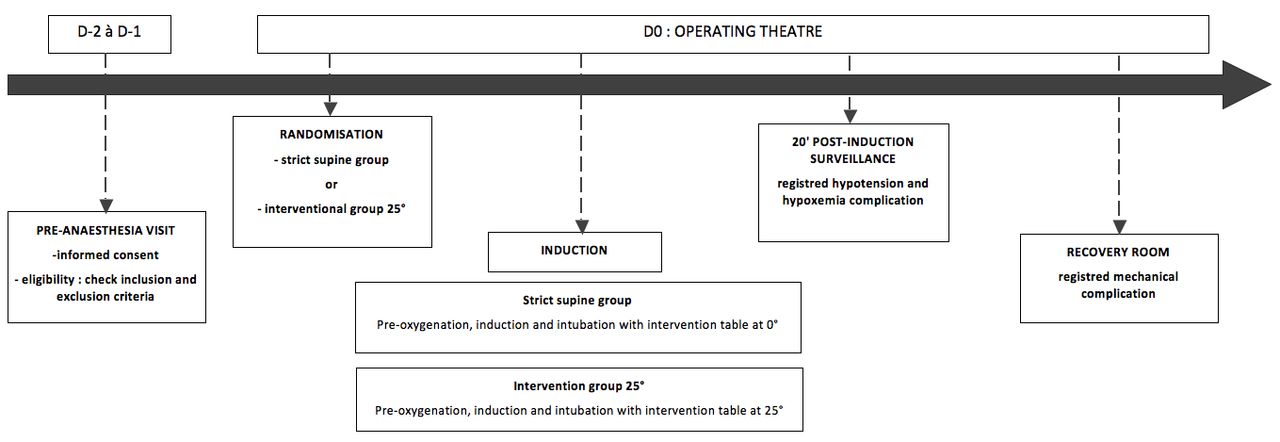
Participant timeline
Figure 3 charts participant timeline through the intervention.
{kind=link}
{kind=link}
{kind=link}
Participant timeline of the InSize25 trial.
Recruitment
Participants are expected to be included during an 18-month inclusion period that began in November 2017. This time-window period was estimated based on the number of orotracheal intubations managed per day by each anaesthetist performing scheduled surgery under general anaesthesia (from 1 to 12 per day) depending on their activity.
2016–2017: Protocol design, approvals from the ethics committee (CPP Sud-Est II); development of trial-related tools (case report form, randomisation system).
2017–2020: Inclusion of patients.
2021: Cleaning and closure of the database. Data analyses, manuscript write-ups and submission for publication.
A prolongation of the inclusion period will be requested if needed based on observed inclusion rate.
Methods: assignment of interventions
Allocation and sequence generation
A permuted-block randomisation (ie, random block sizes) will be conducted using a computer-generated (STATA, V.13) random (1:1) allocation to either supine (strict supine) or 25° (head-up when the operating table can accommodate it, or reverse Trendelenburg if not), ensuring completely random assignment of patients to each randomised group. The randomisation will be stratified according to anaesthetist. Each anaesthetist could include up to 40 patients. All anaesthetists working in all seven study centres were invited to enrol and include patients.
Blinding
For the attending anaesthetist, this trial is open-label and unblinded trial due to the nature of the intervention (changing patient’s position). Although indirect laryngoscopy by an external anaesthetist (blind to the patient’s position) using a videolaryngoscope connected to a smartphone to determine the intubation score could have been proposed as an option to ensure anaesthetist blinding, this type of system setup was not included in the trial design in order to ensure better feasibility among multiple centres. Furthermore, the laryngeal exposure score can differ between direct laryngoscopy and videolaryngoscopy, and the videolaryngoscopy can create a situation in which the view is good but intubation is difficult or impossible.15 Here we wanted to be close to real-world clinical conditions, and the videolaryngoscope is mainly applied as a rescue device (probably too expensive for routine use).
Methods: data collection, management and analysis
Data collection and management
Study data will be prospectively collected and managed by trained research investigators from each participating centre, using Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Clermont-Ferrand University Hospital.16 REDCap is a secure, web-based application designed to support data capture for research studies, providing (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages and (4) procedures for importing data from external sources.
The following data will be collected and registered on inclusion: baseline demographics and characteristics (ie, age, sex, height, weight, BMI, criteria for difficult intubation, surgical details and relevant comorbidities), preoxygenation management, drugs used at induction (type and dose) and for maintenance of the general anaesthesia (sevoflurane, desflurane or propofol), smartphone-measured operating-table angulation, monitoring on neuromuscular-blocking drug action, height of the anaesthetist, height of the patient on the operating table, the intubation conditions, the anaesthetist’s comfort and any complications (hypoxaemia, hypotension, mechanical complication of direct laryngoscopy).
Statistical methods
Sample size estimation
The sample size was determined as recommended by Cohen17 who defined effect-size (ES) bounds as: small (ES: 0.2), medium (ES: 0.5) and large (ES: 0.8, ‘grossly perceptible and therefore large’). We thus need 338 patients per group in order to highlight an ES of 0.25 for a two-sided type I error at 5% and a statistical power of 90%, which corresponds to a minimal difference in primary endpoint of 5%, for a SD ranged between 10% and 20%.
Thinking ahead to potential possible subgroup analyses and to maintain adequate statistical power for the secondary endpoints, it was agreed to recruit 500 patients per group. Interim analyses will be proposed sequentially every 100 inclusions, applying a correction of the type I error (Kim-DeMets, East software). Only the steering committee has access to interim results and make the final decision to terminate the trial if futility cause is found or lack of fundings. None anaesthetist participating in the study has access to the interim analyses.
Statistical analysis
Statistical analyses will be performed with STATA V.13 software. The tests will be two-sided with type I error set at 5%. Continuous data will be expressed as mean±SD according to the statistical distribution. The assumption of normality will be assessed with the Shapiro-Wilk test. For the primary outcome measure, the comparison between the randomised groups will be performed using a Student’s t-test or the Mann-Whitney U test if the assumptions of t-test do not hold. Normality will be verified by the Shapiro-Wilk test and the homoscedasticity by Fisher-Snedecor F test. The results will be expressed as ES and 95% CIs. Multivariate analyses will then be conducted using a linear mixed model. In addition to random effects of centre and anaesthetist, the covariables will be fixed according to univariate results and clinical relevance: height of the anaesthetist, height of the patient at the tragus of the ear at the time of intubation (which could be lower in 25° interventional group because table should be lower to facilitate the intubation) and ratio of these two parameters. Normality of the residuals will be studied using the Shapiro-Wilk test. If appropriate, a logarithmic transformation will be proposed to achieve the normality of the dependent endpoint. The results will be expressed as regression coefficients and 95% CIs.
Interaction with the intubation position parameter (strict supine position vs 25° head-up/Trendelenburg position) will be studied before considering possible subgroup analyses: subgroup 25° head-up versus reverse Trendelenburg position, subgroups considering the height of the anaesthetist.
The secondary endpoints will be compared between randomised groups using a Student’s t-test or Mann-Whitney U test for quantitative parameters (anaesthetist’s comfort during the procedure) and by a χ2 or Fisher’s exact test for categorical data (medical devices required to support tracheal intubation, Cormack-Lehane grade of laryngeal exposure, episodes of desaturation and episodes of arterial hypotension, mechanical complications: laryngeal pain, cough, hoarseness, trauma of the upper airways). For these dichotomous parameters, the results will be expressed as absolute differences and 95% CIs. The multivariate analyses will be conducted using a generalised linear mixed model with a logit link function. The results will be expressed as ORs and 95% CIs.
Repeated data will be analysed by mixed models considering time, group and time × group interaction as fixed effects along with the within-subject and between-subject variability (in addition to centre and anaesthetist effects).
A sensitivity analysis will be used to evaluate the statistical nature of missing data (eg, intubation failure) and to measure the impact on results. The most appropriate imputation approach will be proposed, that is, maximum bias or estimation as proposed by Verbeke and Molenberghs for repeated data.
Methods: monitoring
Data monitoring
Before the start of patient recruitment, all physicians and other healthcare workers working in the operating theatre and recovery room will attend formal training sessions on the study protocol and data collection. Illustrations of the Cormack-Lehane views and POGO score will be included on the data collection form as ready-reference cues.
The anaesthetists will be incharge of daily patient screening and inclusion, ensuring compliance with the protocol and collecting study data. Patients who are eligible but not included will be recorded and the reasons why they are not included will be anonymised and entered into a screening log in each centre.
Data monitoring and quality control will be conducted at least annually in all participating centres by official representatives from the study sponsor, that is, the Department of Clinical Research and Innovation at Clermont-Ferrand University Hospital.
Harms
Not applicable.
As the two positions are well-known and usual routine positions, it is the regular healthcare and vigilance provisions that can be applied for this type of study.
Auditing
Not applicable. Likewise.
Ethics and dissemination
Consent or assent
Patients will be included after giving written informed consent at least the day before the surgery in order to accommodate a reflection period as per the 2013 Declaration of Helsinki.
Confidentiality
Data will be handled in a confidential and anonymous manner, according to French law. All original records will be archived at trial sites for a 15-year retention period. The clean database file will be anonymised and kept for 15 years.
Dissemination policy
Findings will be published in peer-reviewed journals and presented at local, national and international meetings and conferences to publicise and explain the research to clinicians, commissioners and service users. All investigators will have access to the final dataset. Participant-level datasets will be made accessible on a controlled-access basis. Data are deidentified participant data, using REDCap electronic data capture tools. Data are available on reasonable request to the authors of this study.
Discussion
Tracheal intubation using direct laryngoscopy is the cornerstone of general anaesthesia induction. In 2017, the French Society for Anaesthesia and Postoperative Intensive Care published updated guidelines for management of difficult intubation18 and recommended videolaryngoscopy for scheduled surgery in patients with at least two criteria for difficult intubation, but not for all patients. The strict supine position has been used for years is still the standard position for intubation, even if many studies have found better preoxygenation and longer apnoea time by raising the upper body by 25° in obese and non-obese patients.3–6 This position, also known as ‘ramped’ position (elevating the head and upper body until the external auditory canal is aligned with the sternal manubrium), is now recommended for anaesthetic management and intubation of the obese patient,12 but not for the non-obese patient.19
To the best of our knowledge, InSize25 is the first prospective randomised controlled trial with a robust design and large number of non-obese patients which compares strict supine intubation and 25° intubation in operating room, which is the first strength of this study. Semler et al compared in a multicenter, randomised trial the ramped position versus sniffing position during endotracheal intubation of critically ill adults published in Chest in 2017,20 but the conditions of intubation in intensive care are not similar because of the patients who are often unconscious and in respiratory distress and because it is different to intubate on an intensive care’s bed or on the operating table. And in this robust study, the position of the head was really different between the two groups of patients which has a great impact on the intubation conditions. The 25° position was chosen in an attempt to find a good compromise between ventilation optimisation, haemodynamics, mechanics and ease of intubation. Lee et al 8 used this table angulation in their crossover randomised prospective study comparing laryngeal exposure conditions with the POGO score on 40 patients, as did Reddy et al 9 in their before-and-after studies of 781 patients. Here we decided to give anaesthetists the possibility of placing the patient in a 25° head-up position or a 25° reverse Trendelenburg position because some operating tables do not yet accommodate placing patients in a half-sitting position with bent at the waist. However, the head-up position should be preferred by the anaesthetist whenever technically permissible. It is more comfortable for the patient and would allow a leg lift test immediately after induction if necessary, which helps to manage the patient’s haemodynamic state.21 22
The second strength of this study is that it uses the POGO score as primary assessment criterion, which is more relevant, more accurate and has less inter- and intra-individual variability than Cormack-Lehane grades.14 23 Indeed, Cormack-Lehane grade II can correspond to a view of almost the entire glottis or to only a tiny part of it, and so cannot serve predict easy or difficult intubation.24 Laryngoscopy attempts, use of external laryngeal manipulation and use of ancillary equipment are also reported in order to concretely describe the ease of intubation assessed, for example, by the Fremantle score in O’Loughlin et al.15 The laryngoscopy attempts was not chosen as the primary outcome because we doubted that it would make a significant difference with this outcome as most of intubation requires only one laryngoscopy. As for the duration of intubation, it is not always relevant, difficult to precisely measure and could hasten the anaesthetist’s gesture.
Third, as this position is not yet routine for intubation of patients in the operating room, we thought it informative to study height of the operating table in relation to height of the anaesthetist and the comfort score of the anaesthetist performing the intubation.25 Data produced in this pragmatic study will help incorporate this position as standard care, encouraging inexperienced anaesthetists to lay back for the intubation.
Finally, randomisation stratified by anaesthetist limits the bias induced by the subjectivity of the POGO score and Cormack-Lehane grades and also the bias linked to inter-anaesthetist variability in laryngeal exposure and intubation conditions depending on the traction applied during laryngoscopy and the technique used. This inter-operator variability is likely significant26 but also difficult to evaluate ethically, as the procedure is painful and possibly traumatic, which makes it unreasonable to carry out several laryngoscopies in the same patient to compare glottis views and glottis exposure. This study opted for block randomisation to ensure that each anaesthetist includes as many patients in one group as the other. Then, another strength of the study is that each operator is allowed only to intubate 40 patients in the trial. This will ensure a larger number of operators and make the results more generalisable.
This study may have some limitations. First, the InSize25 trial does not protocolise every single aspect of anaesthesia management. Type, dose and route of administration of the induction drugs, preoxygenation management, bag-ventilation during the apnoea induced by anaesthesia before intubation are all left at the discretion of the anaesthetist incharge. As all these aspects can affect the onset of post-induction hypotension or desaturation, the interpretation of results on their frequency could be biased. The anaesthetist-led stratification of the randomisation will limit this bias and, we hope, avoid reluctance from some anaesthetists to place the patient in this 25° position at induction out of fear of hypotension episodes. In any case, the data will be collected and thus inform further understanding. We believe that a restricted protocol would have hampered the inclusion of patients and the feasibility of this pragmatic study.
Second, the unblinded design of the InSize25 trial is a limitation. As stated earlier, it would have been possible to work with indirect laryngoscopy using smartphone-connected videolaryngoscope or endoscope to avoid a self-reported primary outcome, but this approach would have required two anaesthetists: one conducting the laryngoscopy and another one, blinded to allocation group, classifying the POGO score. In 2007, Lee et al 8 compared the POGO score during direct laryngoscopy with a rigid endoscope on 40 patients in supine position and then in 25° backup position. Each laryngeal view was captured and compared by a position-blinded anaesthetist. Comparing the two positions, mean (SD) POGO scores increased significantly from 42.2% in supine position to 66.8% in the 25° backup position (p<0.0001). However, this strategy involved two laryngoscopies per patient with a possible increment of direct laryngoscopy-related complications, which could pose ethical problems. Here, then, the choice of the better view captured to establish the POGO score is left to the anaesthetist incharge of the direct laryngoscopy who is unblinded to the allocation group. Regarding the use of videolaryngoscopy, the laryngeal exposure score can differ between direct laryngoscopy and videolaryngoscopy: in direct laryngoscopy, the view achieved by the line of sight correlates directly to the ease of intubating the trachea, as videolaryngoscopy can create a situation in which the view is good but intubation is difficult or impossible.15 This type of system was not included in the InSize25 trial design in order to ensure better feasibility among multiple centres. Here, this pragmatic study aimed to be close to real-world clinical conditions, and the videolaryngoscope is usually a rescue device.
In conclusion, the InSize25 trial is an investigator-initiated, pragmatic, multicentre, randomised controlled trial powered to compare direct laryngoscopic intubation in scheduled surgery between the strict supine position and the 25° head-up or reverse Trendelenburg position. The InSize25 trial will also assess all aspects of the intubation management as well as any complications and the anaesthetist’s comfort during the procedure.
Acknowledgments
The authors wish to thank the patients and the physicians of this study.
References
Footnotes
Twitter @Fatima BINAKDANE
Contributors MS takes responsibility for the content of the manuscript. MS, BP and J-EB were involved in the conception, hypotheses delineation and design of the study, acquisition and analysis of the data, in writing the article and in its revision prior to submission. A-SF and FB were involved in the design of the study, acquisition and analysis of the data, in writing the article and in its revision prior to submission.
Funding This study received support from University Hospital—–Clermont-Ferrand.
Disclaimer The funders have no influence on the study design, conduct and analysis or in the preparation of this article.
Competing interests The study is an investigator-initiated trial. The study is sponsored by Clermont-Ferrand University Hospital, Clermont-Ferrand, France. There is no industry support or involvement in the trial. The principal investigators have no financial or other competing interests.
Patient consent for publication Obtained.
Ethics approval The Insize25 study is conducted in accordance with the Declaration of Helsinki and was registered at http://www.clinicaltrial.gov on 13 November 2017 under trial identification number NCT03339141. The trial received appropriate approval from the ‘CPP Sud-Est II’ ethical review board in October 2017 (ID-RCB: 2016-A02078-43). Any change to eligibility criteria, outcomes and analyses will be notified to the investigators and ethics committee to secure prior approval.
Provenance and peer review Not commissioned; externally peer reviewed.