Article Text

Abstract
Objectives Recent data relating to the association between spicy food intake frequency and abdominal obesity are limited, especially in low-income areas. Therefore, the study explored the relationship between spicy food intake frequency and abdominal obesity, and assessed the role of energy intake as a mediator of these associations in a rural Chinese adult population.
Design Cross-sectional study.
Setting Rural Chinese adult population.
Participants Subjects from Henan Rural Cohort Study (n=28 773).
Primary outcome measures The effects of spicy food intake frequency on abdominal obesity were analysed by restricted cubic spline and logistic regression, and the mediation effect was analysed using the bootstrap method.
Results The adjusted percentages of abdominal obesity were 47.32%, 51.93%, 50.66% and 50.29% in the spicy food intake subgroups of never, 1–2 day/week, 3–5 day/week and 6–7 day/week, respectively. An inverse U-shaped association was found between spicy food intake frequency and abdominal obesity (p<0.01). Compared with subjects who never consumed spicy food, the adjusted ORs (95% CIs) in the 1–2 day/week, 3–5 day/week and 6–7 day/week subgroups were 1.186 (1.093, 1.287), 1.127 (1.038, 1.224) and 1.104 (1.044, 1.169), respectively. Furthermore, the increased odd of abdominal obesity related to more frequent spicy food intake was mediated by higher fat energy intake; the direct and indirect effects were 1.107 (1.053, 1.164) and 1.007 (1.003, 1.012), respectively.
Conclusions The data indicated that spicy food intake increased the risk of abdominal obesity, and fat energy intake may be a mediator of this association in rural Chinese populations. Clarifying the mechanisms will facilitate the development of novel preventive and therapeutic approaches for abdominal obesity.
Trial registration number ChiCTR-OOC-15006699
- Spicy food intake frequency
- abdominal obesity
- fat energy intake
- mediator analyses
- rural population
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to estimate the relationship between spicy food intake frequency and abdominal obesity mediated by energy intake.
A large, population-based sample was investigated.
The study included available information on a broad range of covariates.
However, the survey did not clarify a relevant causal association between spicy food intake frequency and abdominal obesity.
Introduction
As a disorder of energy metabolism, obesity is defined as abnormal or excessive fat accumulation that may impair health, and the excessive accumulation of visceral fat is an independent risk factor of cardiovascular diseases.1 Although great efforts have been made to control the weight of the population in China, the prevalence of obesity continues to increase, especially in the rural areas.2 According to the data obtained in the China Health and Nutrition Survey (CHNS) in 2011, the prevalence of abdominal obesity was 44.0% in rural China.3 A recent study also showed that the age-standardised prevalence of abdominal obesity was 43.71% in rural Chinese adults.4 Ongoing and reliable programmes are needed to manage obesity and reduce the associated complications. It is commonly acknowledged that many modifiable risk factors contribute to obesity besides genetic factors. Physical activity and lifestyle factors, particularly dietary behaviour, are considered to be closely related to obesity, especially in low/middle-income countries.1
Spices, which improve the flavour and taste of food, have long been widely consumed in Chinese cuisine.5 Several studies have indicated that the consumption of spicy food affects obesity-related human health outcomes, such as hypertension, irritable bowel syndrome, lipid disorders, cancers and even mortality.6–10 As the most practical and simplest index, waist circumference is used to measure the magnitude of fat accumulation in the abdomen. An observational study conducted in five urban and five rural areas of China provided evidence that the frequency of spicy food consumption was positively associated with waist circumference,11 which indicated that spicy food intake plays a role in the regulation of abdominal obesity. According to the sixth national population census, the rural districts account for 63.90% of the population of China, and the education level, economic development, behaviour factors, food choices and dietary patterns in rural areas differed from those found in urban areas of China.12 However, the associations between spicy food intake frequency and abdominal obesity in rural populations remain to be fully elucidated. Furthermore, population studies have shown that spicy food consumption inhibits obesity by regulating energy metabolism,13 and Choi and Chan14 found that the energy intake in chili pepper non-users was significantly lower than that in chili pepper users in the New York City area. However, the associations among spicy food intake frequency, energy intake and abdominal obesity have not been reported.
Therefore, the study investigated the effects of spicy food intake frequency on abdominal obesity in a rural Chinese population, and assessed the role of energy intake as a mediator of these associations.
Methods
Study participants
The participants in the current study were from the Henan Rural Cohort Study.15Briefly, the study was carried out between July 2015 and September 2017 in the following locations in Henan Province in China: Xuchang City, Yuzhou County; Zhumadian City, Suiping County; Kaifeng City, Tongxu County; Xinxiang City, Xinxiang County and Sanmenxia City, Yima County. A total of 29 867 people aged between 18 and 79 years and with complete information for spicy food intake and waist circumference measurements were recruited into the current study. To better estimate the relationship between the frequency of spicy food intake and abdominal obesity, 365 subjects with serious diseases (heart failure, kidney failure and malignant tumour), 650 participants with hepatitis or tuberculosis or other infectious diseases, 51 women who were pregnant or lactating, and 28 subjects under weight control management during the previous 6 months were excluded. Finally, 28 773 participants were included in the current analysis.
Patient and public involvement
Neither patients nor the public were involved in developing this project.
Assessment of spicy food intake frequency
The Food Frequency Questionnaire (FFQ) regarding dietary intake was delivered by well-trained staff through face-to-face interviews. Participants were also asked ‘During the past month, how often did you have spicy foods in one week?’ and a frequency between 0 and 7 days per week was selected by the participants. Based on the observation of the existing epidemiological studies,16 the participants were divided into four groups according to spicy food intake frequency: never (reference), 1–2 day/week, 3–5 day/week and 6–7 day/week. The participants were asked to confirm that the food types contained spices. The test–retest reliability and the internal consistency of the questionnaire were accredited through a pilot study with 76 subjects. The intraclass correlation coefficient (ICC) was 0.978, which indicated that the current variable provides a reasonable estimation of spicy food intake frequency.
Assessment of covariates
Detailed information on sociodemographic and lifestyle factors was collected using a questionnaire. The following variables were included in the current study: age, gender, education, tobacco use (current smoker was defined as smoking at least one cigarette per day for six consecutive months), alcohol use (current drinker was defined as alcohol drinking of at least 12 times per year) and marital status. Individual dietary intake data were collected by asking each household member to report the category of all food consumed, quantity, meal type and dining place) using a dietary recall method. The quantity of food consumed, including staple food, livestock, poultry, fish, eggs, dairy, fruits, vegetables, beans, nuts, pickles, cereal and animal oil over the previous year was recorded. For each individual, the mean total daily energy intake and the proportions of protein, fat and carbohydrate were derived from dietary data according to the Chinese Food Composition Table (2009). The 3-day 24 hours record was conducted in a small sample to validate the FFQ and the results demonstrated that the questionnaire provided a representative tool to conduct a dietary evaluation of a rural population.17 Physical activity was divided into low, middle and high according to the international physical activity questionnaire.18 Blood pressure recorded on the right arm supported at heart level in the sitting position was measured using electronic sphygmomanometers (Omron HEM-7071A, Japan). All recordings were obtained in triplicate and the mean value was used for analysis. Body weight with light clothing was measured to the nearest 0.1 kg using a weight measurement device (VBODY HBF-371, OMRON, Japan). Height was measured to the nearest 0.1 cm without shoes using a standard right-angle device and a fixed measurement tape. The body mass index (BMI) was estimated as body weight (kg) divided by the height squared (m2).
Assessment of outcomes
Waist circumference was measured to the nearest 0.1 cm at a point midway between the lowest rib and the iliac crest in a horizontal plane using a non-elastic tape. All measurements were obtained in duplicate by trained research staff according to a standard protocol from the Working Group on Obesity in China and the mean values were used for statistical analyses. Abdominal obesity was defined as a waist circumference ≥90 cm for men and ≥80 cm for women according to the guidelines of the International Diabetes Federation for Chinese populations.19
Statistical analysis
Continuous variables were described as means±SD and categorical variables were presented as proportions. Analysis of variance and X2 tests were used to evaluate the differences in the general characteristics of the four spicy food intake frequency subgroups. The crude, age-adjusted and sex-adjusted percentages of abdominal obesity in the different groups were estimated. Restricted cubic spline analysis was used to explore the dose–response relationship between continuous spicy food intake frequency and abdominal obesity. Logistic regression analysis was used to estimate the association of categorical spicy food intake frequency and abdominal obesity based on the ORs and 95% CIs.
To examine the extent of the association between spicy food intake frequency and abdominal obesity mediated by energy intake, we estimated the magnitude of change in the regression coefficient with and without adjustment for different types of energy intake. The following models were evaluated in the analyses: model 1, the crude model; model 2, adjusted for age, gender, education, marital status, tobacco use, alcohol use and physical activity; model 3, adjusted for model 2 plus total energy intake; model 4, adjusted for model 2 plus protein energy intake; model 5, adjusted for model 2 plus fat energy intake and model 6, adjusted for model 2 plus carbohydrate energy intake. The mediation analyses were conducted using the bootstrap method. A conceptual model to illustrate the proposed association between spicy food intake frequency (predictor variable), energy intake (mediator) and abdominal obesity (dependent variable) was conducted. Stratified subgroup analyses were performed, according to the demographic characteristics and the types of spicy food, to investigate changes in the effects of spicy food intake frequency on the risk of abdominal obesity. The statistical analyses of the current data were performed using SPSS V.23.0 software package and p<0.05 (two tailed) was considered to indicate statistical significance.
Results
Demographic characteristics
Table 1 summarises the general characteristics of the participants. The mean age of 28 773 subjects was 55.39±12.36 years, and the mean values of waist circumference were 85.44±10.55 cm for males and 82.54±10.22 cm for females. There were significant differences in the characteristics of age, gender, education level, tobacco and alcohol use, marital status, BMI, waist circumference, systemic blood pressure (SBP), diastolic blood pressure (DBP), protein energy, fat energy and carbohydrate energy between the spicy food intake frequency subgroups (p<0.05).
Characteristics of the participants according to the spicy food intake frequency
Distribution of abdominal obesity in subgroups
The percentages of abdominal obesity by the categories of spicy food intake frequency are shown in figure 1. Among the participants, 49.15% had abdominal obesity, of which 5997 (48.79%), 1674 (51.48%), 1575 (48.60%) and 4968 (49.73%) were categorised in the never, 1–2 day/week, 3–5 day/week and 6–7 day/week, subgroups of spicy food intake frequency, respectively. The corresponding age-adjusted and sex-adjusted percentages of abdominal obesity were 47.32%, 51.93%, 50.66% and 50.29%, respectively.

The percentage of abdominal obesity by different categories.
Association between spicy food intake frequency and abdominal obesity
The ORs of the spicy food intake frequency subgroups for abdominal obesity first increased and then declined after reaching the peak. All non-linear association tests revealed this inverted U-shaped dose–response relationship (p<0.01, figure 2).

ORs (solid lines) and 95% CIs (dashed lines) of spicy food for abdominal obesity from restricted cubic splines. (A) Crude model, (B) adjusted for age, gender, education, marital status, tobacco use, alcohol use and physical activity, (C) adjusted for B plus total energy intake, (D) adjusted for B plus protein energy intake, (E) adjusted for B plus fat energy intake, (F) adjusted for B plus carbohydrate energy intake.
Table 2 summarises the ORs of spicy food intake frequency for abdominal obesity. Taking the participants who never consumed spicy food as the reference group, the crude ORs (95% CIs) for the 1–2 day/week, 3–5 day/week and 6–7 day/week subgroups were 1.113 (1.031, 1.203), 0.992 (0.918, 1.072) and 1.038 (0.985, 1.095), respectively. For each 1-day increment in the frequency of spicy food intake, the OR (95% CI) was 1.009 (0.992, 1.027) (Ptrend=0.308). After adjustment for potential confounders, the ORs (95% CIs) of 1–2 day/week, 3–5 day/week and 6–7 day/week subgroups were 1.183 (1.090, 1.283), 1.129 (1.040, 1.226) and 1.118 (1.057, 1.183), respectively. The adjusted OR (95% CI) was 1.036 (1.017, 1.055) for each 1-day increment in the frequency of spicy food intake. In further analyses of changes in the ORs (95% CIs) with and without adjustment for energy intake, spicy food intake frequency remained positively associated with abdominal obesity in models 3–6. After adjusting for fat energy intake, the ORs (95% CIs) were 1.186 (1.093, 1.287), 1.127 (1.038, 1.224) and 1.104 (1.044, 1.169), respectively. The adjusted OR (95% CI) was 1.051 (1.032, 1.070) for each 1-day increment in the frequency of spicy food intake.
The ORs (95% CIs) of spicy food intake frequency for abdominal obesity
Mediating role of energy intake
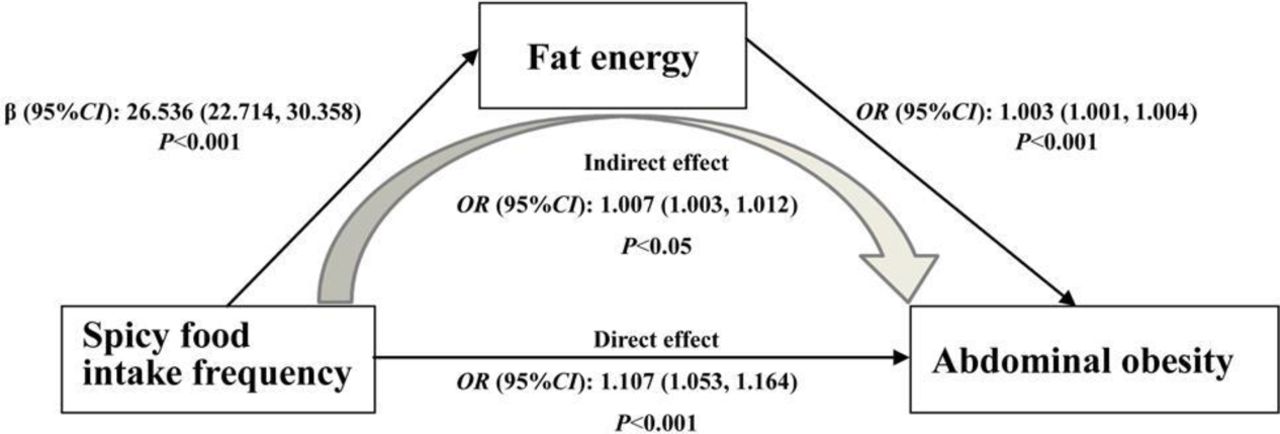
The role of energy intake in mediating the association between spicy food intake frequency and the risk of abdominal obesity was analysed, and the related results are presented in online supplementary table 1. The ORs (95% CIs) for direct and indirect effects mediated by fat energy intake on the associations between spicy food intake frequency and abdominal obesity were 1.107 (1.053, 1.164) and 1.007 (1.003, 1.012), respectively. The adjusted OR (95% CI) of spicy food intake frequency for fat energy intake was 26.536 (22.714, 30.358), and the adjusted OR (95% CI) of fat energy intake for abdominal obesity was. Our analyses indicated that fat energy intake partially mediated the relationship between spicy food intake frequency and abdominal obesity (figure 3). There were no significant effects mediated by protein energy intake, carbohydrate energy intake and total energy intake.
Supplemental material
{kind=link}
{kind=link}
{kind=link}
The mediation analyses between spicy food intake frequency and abdominal obesity by fat energy intake.
Subgroup analyses between spicy food intake frequency and abdominal obesity
The ORs (95% CIs) of spicy food intake frequency subgroups for abdominal obesity are presented in table 3. There were no statistically significant trend associations in subgroup participants aged ≤30 years, >61 years, male, illiterate and elementary-level educated, widowed/single/divorced/separated, ex-smoker, smoker, ex-drinker, drinker and low physical activity (ptrend >0.05).
The subgroup ORs (95% CIs) of spicy food intake frequency for abdominal obesity
Discussion
The present epidemiology survey provides new evidence for the current burden of abdominal obesity in rural Chinese populations. Overall, the prevalence of abdominal obesity was higher in a rural population of Chinese adults than that in previous national studies in China.3 In total, 57.28% of participants consumed spicy food, demonstrating the popularity of spicy food in the Chinese diet.20 Compared with participants who never had spicy food, the participants in the spicy food intake frequency subgroups (1–2 day/week, 3–5 day/week and 6–7 day/week) were positively associated with an increased risk of abdominal obesity. Moreover, an inverted U-shaped relationship between spicy food intake frequency and abdominal obesity was observed in the current study. The study also showed that fat energy intake partially mediated the association between spicy food intake frequency and abdominal obesity.
A previous intervention study showed a beneficial effect of spicy food consumption on weight management in a small sample size from Western countries,21 although data regarding the effect of spicy food on obesity in Asian populations are scarce. A prospective study of CHNS data showed that the cumulative average chili intake was inversely associated with the risk of overweight/obesity, which was independent of overall dietary pattern, energy intake and lifestyle factors.22 In contrast, clinical trials have also shown no significant differences in the indicators of obesity between the placebo and capsaicin groups.23 Additionally, a previous study combining cross-sectional and meta-analysis showed that spicy food intake frequency was positively associated with general obesity in rural Chinese populations.16 Both the BMI and waist circumference are considered as practical and effective indexes in evaluating obesity.24 BMI is closely related to body fat,25 and reflects the degree of obesity without the influence of differences in height. However, BMI does not accurately reflect the distribution of fat mass in the body, whereas waist circumference is regarded as the most practical and simplest indicator for evaluating abdominal fat accumulation.26 In this study, we found that the mean waist circumference was in the desirable range for males, but elevated for females. This phenomenon might be explained by asymmetrical age structure and hormone differences.15 27 28 Perimenopausal and postmenopausal women are known to experience relatively unfavourable metabolic changes compared with those in men of similar age, making women more likely to show a tendency for abdominal weight gain during the menopausal transition.27 28 Studies exploring the associations between spicy food intake frequency and abdominal obesity are still limited. Snitker et al 29 and Haramizu et al 30 conducted investigations using capsinoids, which are non-pungent capsaicin analogues.13 Snitker et al 29 reported that abdominal adiposity decreased to a greater extent in the capsinoid group than in the placebo group, although the mean change in waist girth was not significant. Fat oxidation increased in the capsinoid group, a pattern analogous to that observed in the animal study conducted by Haramizu et al.30 Furthermore, it should be noted that the effects of capsinoids delivered to humans in capsules and mice being fed capsiate solution prior to an endurance test cannot necessarily be extrapolated to those in free-living humans consuming capsaicin-containing spicy food as part of their regular diet. Thus, further studies are required to fully elucidate the effects of spicy food components on abdominal adiposity. The China Kadoorie Biobank study showed that waist circumference increased with the frequency of spicy food intake,11 which is consistent with the current results. In addition, the non-linear association tests demonstrated an inverted U-shaped dose–response relationship between spicy food intake frequency and abdominal obesity in all participants. It can be speculated that this effect is related to the observation that participants who consume spicy foods more regularly tend to become less sensitive to the oral tactile effects and rate spicy stimuli as having lower burn intensity.31 32 However, these preliminary findings require further verification in other populations and multicentre study.
Accumulating evidence from animal studies and clinical trials suggested that spicy food consumption may reduce energy intake and enhanced fat oxidation.33 34 However, the prospective study using CHNS data showed that high amounts spicy food intake was positively associated with energy intake. The mean energy intake of participants who consumed more than 50 g/day of chili was greater (>200 kcal/day) compared with that of the non-spicy food intake group.22 In addition, capsaicin is a basic component of spicy food and responsible for approximately 70% of the burn. Janssens et al 35 found that satiety and fullness increased when capsaicin was added into the human diet. Moreover, several human studies have indicated that capsaicin plays an important role in energy balance by changing the intake of fat, carbohydrate and protein.36 37 Although metabolic studies have indicated a lipolytic effect of spices, these studies have shown that fat energy intake mediates the association between spicy food intake frequency and abdominal obesity. It can be speculated that the mechanism underlying the cholesterol-lowering activity involves the capacity of spicy food to stimulate faecal excretion of bile acids and increased resistance of serum lipoproteins to oxidation.38 However, the effect of spicy food on weight management in terms of the mechanisms underlying energy intake balance and changes in appetite and lipid metabolism remain to be clarified.39 In addition, Kawada et al 40 found that capsaicin supplementation lowered serum triacylglycerol concentration and stimulated lipid mobilisation from adipose tissue but did not affect lipogenesis in obese rats. Non-ivamide, which is a less pungent structural analogue of capsaicin, was found to prevent weight gain without affecting blood total cholesterol, low-density lipoprotein cholesterol or triglycerides in a 12-week intervention trial.41
Considering the defects of this cross-sectional study, further investigations are warranted to explore the pathophysiological mechanisms underlying the effect of spicy food consumption on abdominal obesity and lipid metabolism. In our subgroup analyses, there was no association between spicy food intake frequency and abdominal obesity in participants aged over 61 years, possibly as a result of the severe effects of the Chinese famine occurred in 1959–1961 on the prevalence of obesity in adults in Henan Province. We previously reported that marital status, tobacco use, alcohol use and physical activity were associated with abdominal obesity, particularly in women, which could explain the associations of the subgroups to some extent.4 The variety of chili types and the lifestyles of both sexes partly account for the relationships between each additional day of spicy food intake and abdominal obesity in the subgroup analyses. Additionally, the current study showed that the participants with higher spicy food intake tended to have lower SBP and DBP, which is consistent with the findings of He et al. 42 In terms of the associations of both obesity and hypertension with chronic disease, a possible association between spicy food intake and hypertension warrant further investigations. To some extent, the current epidemiological study indicated that the spicy food might affect abdominal obesity by increasing energy intake. These effects might vary depending on the type of fats consumed (eg, saturated, trans, monounsaturated, polyunsaturated); thus, further studies focusing on the different types of fats consumed should be conducted to examine the contribution of fat energy intake to the effects of spicy food intake on abdominal obesity.
This is the first study to estimate the relationship between spicy food intake frequency and abdominal obesity mediated by energy intake. However, several limitations should be noticed. First, as a cross-sectional study, we were unable to reveal a causal association between spicy food intake frequency and abdominal obesity and studies with long-term follow-up are needed to validate the associations. Second, assessing dietary behaviours in population-based studies through FFQ might have reporting and recall bias, and the variety of chili types might affect the associations. However, a validation study with a small number of participants who completed the 3-day 24 hours recall demonstrated that the current FFQ is a representative tool to conduct a dietary evaluation of a rural population. Third, some residents, such as college students and migrant workers, were not included in the current study. These groups are more likely to be young and healthy, which might lead to an overestimate of the proportion of abdominal obesity in the rural population. Finally, the participants in the current study were from one province in the central region of China, which may not be representative of the total Chinese rural population. However, the rural population of Henan Province accounts for 9% of total rural Chinese population. Therefore, the results of this study provide some insights into the association between spicy food consumption and abdominal obesity.
In conclusion, the present study indicates that the frequency of spicy food intake is positively associated with abdominal obesity in the rural Chinese population, and implicate fat energy intake as a potential mediator linking the increased prevalence of abdominal obesity in this population. Therefore, multicentre, prospective and intervention studies are needed to further explore the possible causal associations and elucidate potential mechanisms.
Acknowledgments
The authors would like to thank the participants, coordinators and administrators for their support during this study. The authors would like to express their gratitude to Tanko Abdulai for his critical reading of the manuscript.
References
Footnotes
Contributors CW conceived and designed the study. KY, YL, YX, LW, XD, ZM and WL coordinated data collection. KY, YL, XL and RT conducted the analyses. YL and KY wrote the manuscript. All authors have approved the final manuscript.
Funding This research was supported by the National Key Research and Development Programme Precision Medicine Initiative of China (grant no: 2016YFC0900803), National Natural Science Foundation of China (grant no: 81573243, 81602925, U1304821), Science and Technology Foundation for Innovation Talent of Henan Province (grant no: 164100510021, 154200510010), Henan Natural Science Foundation (grant no: 182300410293), High-level Personnel Special Support Project of Zhengzhou University (grant no: ZDGD13001).
Disclaimer The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was conducted according to the Declaration of Helsinki guidelines, and all procedures were approved by the Zhengzhou University Life Science Ethics Committee (Code: (2015) MEC (S128)).
Provenance and peer review Not commissioned; externally peer reviewed.