Article Text

Abstract
Objectives To assess whether changes in patterns of combined oral contraceptive (COC) prescriptions to starters between 2008 and 2016 were in line with changes in national recommendations for use.
Design Historical prospective cohort study.
Setting The national Norwegian Prescription Database.
Participants Women aged 10–49 years who started COCs between 1 January 2008 and 30 June 2016, in total 285 009 women.
Primary outcome The proportion of levonorgestrel-containing COC prescriptions to starters.
Intervention The Norwegian Medical Agency recommended levonorgestrel-containing COCs to starters from 2010 onwards.
Results The proportion of levonorgestrel-containing COCs prescribed to starters increased from 41% in 2008 to 80% in 2016 with the greatest increase from 2011 to 2012. This prescription pattern comprised all age groups but was observed to a lower extent among older women. Public health nurses and midwifes had the highest compliance with recommendations and prescribed levonorgestrel-containing COCs to 96% of starters aged <20 years in 2016, compared with 75% and 86% among general practitioners and doctors with no specialty.
Conclusion All professions have increased the proportion of levonorgestrel-containing COC prescriptions to starters. Public health nurses and midwives had the highest compliance with the new recommendations. Future studies will examine whether this shift in prescription pattern has prevented venous thromboembolism in women of reproductive age in Norway.
- contraceptives
- hormonal contraception
- combined oral contraceptives
- venous thromboembolism
- gestagens
- physician prescription pattern
- women's health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- contraceptives
- hormonal contraception
- combined oral contraceptives
- venous thromboembolism
- gestagens
- physician prescription pattern
- women's health
Strengths and limitations of this study
The main strength of this study was the use of national register data comprising all combined oral contraceptive prescriptions in Norway.
Large dataset with reliable information about prescriptions (endpoint) and prescribers (exposure).
Minimal, if any, recall bias or misclassification bias as the endpoint and exposure are registered as prescribed by prescribers rather than as reported by users.
A 4-year, register-based ‘wash-out’ window before study start minimalised misclassification bias of ‘starters’.
Online prescriptions from abroad are not included in the register data. We consider this limitation to be minimal, as hormonal contraceptives are easily available and affordable.
Introduction
Venous thromboembolism (VTE) is a serious, though rare, complication of combined oral contraceptives (COCs).1 The first COCs were launched in the early 1960s.2 Since then, the oestrogen dose they contain has significantly decreased, as prothrobotic properties were thought to be associated more with the oestrogen component than the gestagen (synthetic progestins) component. This replacement proved highly effective in reducing the risk of thrombosis,3 while a further decrease from 30 to 20 µg ethinyl estradiol has had a limited impact on VTE risk.4–6
From 1995, the gestagen component of COCs has received more attention, as three independent studies of that time reported significantly different VTE risks by type of gestagen.7–9 Numerous studies on COCs containing gestoden and desogestrel, and later drospirenone, have reported a VTE risk that was twice that observed in COCs containing levonorgestrel.4–6 10–14 The VTE risk associated with COCs containing the newest gestagens, dienogest and nomegestrol, is not yet known.15
The prothrombotic effect of COCs is mainly related to the dose of oestrogen they contain, but gestagen seems to reverse this effect.16 It has been theorised that various gestagens have different abilities to reverse the prothrombotic effect of oestrogen and that levonorgestrel is more effective at reversing this effect than the newer gestagens.16 One theory for this mechanism is the effect of gestagens on the quantity of sex hormone-binding globulin, which reflects the level of ‘oestrogenisity’ in the blood, as levonorgestrel reduces this quantity to a greater extent than newer gestagens.17–19
Given the lack of solid pharmacovigilance data, medical agencies around the world have hesitated to change their recommendations of COC use. In 2009, the Norwegian Medicines Agency (NOMA) found that the evidence was strong enough to recommend COCs with levonorgestrel to starters.20 In 2010, NOMA initiated a campaign in collaboration with the Norwegian Directorate of Health and the companies that sold COCs in Norway. It comprised letters to various prescribers (physicians, public health nurses and midwifes). Facebook and Twitter groups were established with known bloggers, and new packaging for COCs included a warning on VTE symptoms and risks. The aim of this study was to assess whether changes in patterns of COC prescriptions to starters between 2008 and 2016 were in line with changes in national recommendations for use.
Material and methods
We used a historical prospective cohort design to analyse data from the Norwegian Prescription Database (NorPD). NorPD was established on 1 January 2004. All pharmacies take part in the compulsory, electronic reporting to this registry, which contains information on prescriptions, prescribed drugs delivered by pharmacies to users, users and prescribers.21 NorPD includes detailed information about the prescribed drug, date of delivery and location of the pharmacy; user information on month and year of birth, gender and home municipality; and prescriber information on year of birth, gender, profession and subspecialisation. When prescriptions are recorded in NorPD, the personal identification number of the user and the prescriber is replaced with a pseudonym.
A total of 939 469 women had at least one prescription for hormonal contraceptives registered in NorPD between 1 January 2004 and 30 June 2016. We excluded women who did not have any prescriptions for COCs in this period (n=282 104) and women who used COCs before 2008 (n=370 517). Finally, we excluded women with prescriptions from pharmacists/veterinarians (n=65), women aged ≥50 years (n=519), women with prescriptions with missing user age (n=313) and women with prescriptions missing prescriber ID (n=942). After these exclusions, 285 009 women were eligible for inclusion in the analysis.
COCs are categorised as pills that contain one of the following gestagens: levonorgestrel, norethisterone, desogestrel, drospirenone or dienogest/nomegestrol. Period and age at first COC prescription were categorised into five groups (2008, 2009–2010, 2011–2012, 2013–2014 and 2015-2016/10–14, 15–19, 20–24, 25–29, 30–34 and 35–49 years). Residence was used to determine the health region (Southern/Eastern, Western, Central and Northern) of users. Information on prescribers’ age (≤29, 30–39, 40–49, 50–59 and ≥60 years), gender (male or female) and profession was also included. Profession was categorised as doctor with no specialty, general practitioner, gynaecologist, doctor with other specialty and public health nurse/midwife. Doctors with no specialty included doctors in specialisation, postgraduate students from medical school doing their internship and medical students who had a valid licence issued from the fifth year of medical school. Doctors with more than one specialty were assigned to the most recent specialty. Public health nurses and midwives had the right to prescribe COCs to women aged 16–19 years only.
All analyses were done in Statistical Package for Social Sciences V.22.0 with χ2 test for trend for categorical variables at a significance level p<0.05. We defined starters as women who used COCs for the first time ever. When estimating the annual proportion of starters, we applied data from NorPD for starters as the numerator and data for the entire female population aged 15–49 years from Statistics Norway as the denominator. In these estimates, adjustments were made for starters in previous years.
Patient and public involvement
As the study was register-based, the research question and outcome measures were not informed by any specific patient priorities, experiences or preferences. This study used only data from NorPD and thus did not include a recruitment process for patients; therefore, patients were not involved in the design or the conduct of the study.
Results
Over the study period (complete years 2008–2015) the prevalence of COC use (20.1%–20.3%) and the proportion of starters of COCs (3.2%–3.3%) among women of reproductive age (15–49 years) were remarkably stable. The proportion of starters among all women filling a COC prescription decreased significantly from 17.0% to 12.7% between 2008 and 2015. This proportion was fairly constant among women aged 15–19 years (34.1%–35.0%), while a decrease was observed in the proportion of starters among all women filling a prescription of COCs in older age groups across the study period (decreasing from 7.0%–13.0% to 4.5%–7.1%) .
Most starters were aged below 20 years, and there was a relative increase in the proportion of starters among the youngest women (table 1, upper panel). The proportion of prescriptions of COC to starters in the different health regions was very stable over the study period (table 1, central panel). While general practitioners were the main prescribers of COCs at the beginning of the study period, doctors with no specialty had the highest proportion of prescriptions of COC to starters in the last part of the study period (table 1, lower panel). Public health nurses and midwives prescribed approximately 25% of COCs to starters. COC prescriptions to starters by gynaecologists were low and decreased slightly over time. Doctors with other specialties had the lowest proportion of prescriptions of COC to starters (table 1, lower panel).
Characteristics of starters and prescribers of combined oral contraceptives, 2008–2016 (%)
The age of prescribers gradually increased during the study period for all professions, except for doctors with no specialty. Among the main prescribers of COCs to starters, there were minimal differences in gender, except for public health nurses and midwives, who were almost 100% women.
Levonorgestrel was the most common gestagen in the COCs prescribed throughout the study period. The proportion of prescriptions with levonorgestrel-containing COCs to starters increased from 41% in 2008 to 80% in 2016 (table 2, upper panel, and figure 1) (χ2-trend, p<0.001), with the greatest increase occurring from 2011 to 2012. In 2012, the proportion of prescriptions with levonorgestrel-containing COCs to starters became greater than the proportions of prescriptions with desogestrel-containing and drospirenone-containing COCs combined. After 2012, the proportion of prescriptions with levonorgestrel-containing COCs increased gradually, but the increase was smaller in the last years of the study period (figure 1). Prescriptions of dienogest-containing and nomegestrol-containing COCs to starters represented less than 1% of investigated prescriptions during the study period, and the proportion of prescriptions of norethisterone-containing COCs decreased (table 2, upper panel, and figure 1).

Proportion of COC prescriptions to starters by type of gestagen, 2008–2016. COC, combined oral contraceptive.
Proportion of different types of combined oral contraceptives prescribed to starters, 2008–2016 (%)
The proportion of starters who were prescribed COCs with the lowest dose of oestrogen did not change during the study period (table 2, lower panel). The prescription rate of levonorgestrel-containing COCs increased in similar terms for pills with both 20 and 30 µg oestrogen, while the prescription rate of COCs containing other gestagens, independent of oestrogen dose, decreased.
The proportion of prescriptions of levonorgestrel-containing COCs increased among starters in all age groups (figure 2) (χ2-trend, p<0.001; age-stratified analyses). The differences between the various age groups were small before 2012, but after that, a larger increase was observed among the youngest starters (<20 and 20–24 years). The proportion of prescriptions of levonorgestrel-containing COCs decreased with increasing age of starters. In 2016, the proportion of prescriptions of levonorgestrel-containing COCs ranged from 65% among starters aged ≥35 years to 85% among starters aged <20 years (figure 2).
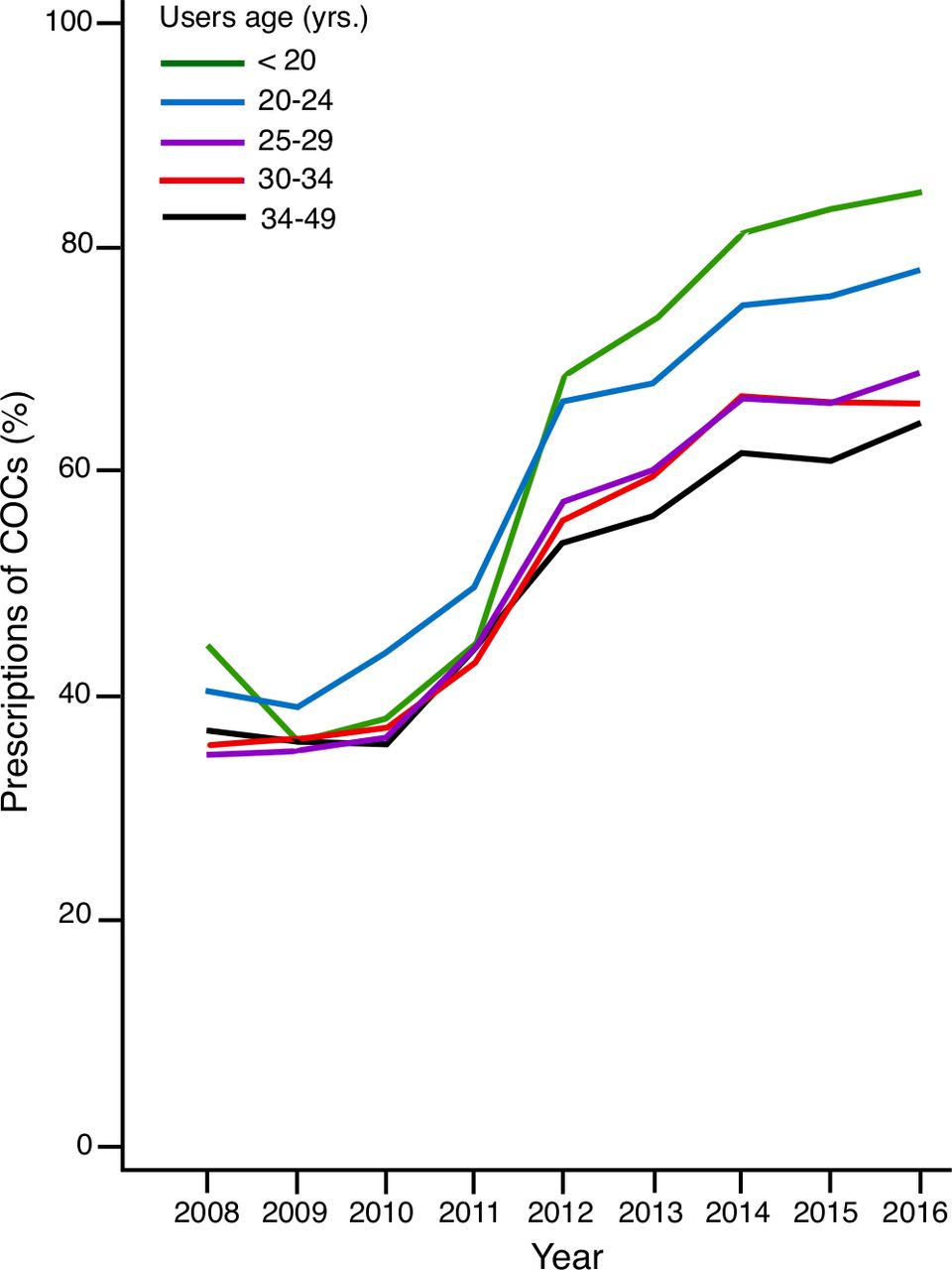
Proportion of COC prescriptions containing levonorgestrel to starters by age, 2008–2016. COC, combined oral contraceptive.
There were small differences in the prescription rate of levonorgestrel-containing COCs across the various professions before 2012, but thereafter, greater differences in compliance with the national recommendations were observed. Public health nurses and midwives, who were only able to prescribe to women aged between 16 and 19 years, had had the highest prescription rate of levonorgestrel-containing COCs to starters: 96% in 2016 (figure 3). In contrast, the other main prescribers, general practitioners and doctors with no specialty, increased their prescription rate of levonorgestrel-containing COCs to 75% and 86% among starters aged <20 years. Gynaecologists followed the same prescription pattern to starters as general practitioners. Doctors with other specialties had the lowest prescription rate of levonorgestrel-containing COCs to starters aged <20 years throughout the study period, and the rate increased to 59% in 2016 (figure 3).

Proportion of COC prescriptions containing levonorgestrel to starters <20 years by profession, 2008–2016. COC, combined oral contraceptive.
All professions showed decreasing prescription rates of levonorgestrel-containing COCs with increasing age of starters. The increase in the prescription rate of levonorgestrel-containing COCs was less marked among starters aged >20 years (figure 4) than among starters aged <20 years (figure 3) for all professions. The greatest difference in the prescription rate of levonorgestrel-containing COCs between starters aged <20 and >20 years was seen among gynaecologists, who had the lowest prescription rate of levonorgestrel-containing COCs, together with doctors with other specialties, throughout the study period (figures 3 and 4). The majority of prescriptions from gynaecologists were to starters aged 25–49 years, while general practitioners and doctors with no and other specialties had a more even distribution of prescriptions to starters in the age groups 20–24 and 25–49 years.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of COC prescriptions containing levonorgestrel to starters ≥20 years by profession, 2008–2016. COC, combined oral contraceptive.
Discussion
The proportion of prescription of levonorgestrel-containing COCs to starters has, independent of oestrogen dose, increased from 41% in 2008 to 80% in 2016, with the greatest increase observed from 2011 to 2012. This may be related to the updated recommendations published by NOMA in 2010, which stated that levonorgestrel-containing COCs should be the first choice for starters because of the lower VTE risk. The fact that four out of five starters obtained the recommended COCs in the first half of 2016 shows high compliance with these recommendations.
The greatest increase in the prescription rate of recommended COCs was seen among the youngest starters (<20 years and 20–24 years); the proportion of prescriptions of levonorgestrel-containing COCs decreased with the increasing age of starters. Some women included in the study, mainly in the oldest age groups, may have used COCs before 2004 and may be ‘restarters’. The restarters in this study would have had a break of at least 4 years, and thus levonorgestrel-containing COCs should be the first choice based on the VTE risk. Nevertheless, restarters have experiences that may affect the type of COC they want, and this may explain the differences in prescription patterns among women across age groups.
Public health nurses and midwives, who only had the right to prescribe COCs to women between 16 and 19 years of age, had the highest prescription rate of levonorgestrel-containing COCs to starters: 96% in 2016. This suggests that midwives and public health nurses may be more aware of and have better compliance in general with best practice recommendations than other prescribers. The other main prescribers, doctors with no specialty and general practitioners, prescribed the recommended COCs to 86% and 75% of starters aged <20 years in 2016. General practitioners especially may increase their prescription rate of levonorgestrel-containing COCs to further increase the total proportion of starters obtaining COCs with the lowest risk of VTE. Although gynaecologists and doctors with other specialties had the lowest proportion of prescriptions of levonorgestrel-containing COCs to starters, they contributed a small number of prescriptions overall, and their prescription volume was less important for overall use.
All professions prescribed recommended COCs less often to older starters. The greatest difference in prescriptions between starters below and above 20 years of age was seen among gynaecologists, but they probably provide more prescriptions to restarters compared with the other professions, since gynaecologists have a higher volume of prescriptions to older women.
The strength of this study is the large dataset, with reliable information about prescriptions and prescribers, and that all pharmacies take part in the compulsory, electronic reporting of prescriptions to NorPD. Moreover, only a few women were excluded from the analysis. Other strengths include the elimination of recall bias on the type of COC used, as this was a register-based study, and the near elimination of misclassification of starters by having a 4-year window of exposure before study start. A possible limitation of the study is that filled prescriptions do not necessarily mean that the medication was actually taken. As 91.5% of the study participants had one refill and 83.9% had two refills of a hormonal method within timely intervals of first initiation of COCs, we find it reasonable to state that the sales database NorPD reflects real use. Indeed, Triebwasser et al reported that pharmacy claims are more reliable than self-reported contraceptive use, which is often overestimated.22
The medical product agencies in Sweden and Denmark also updated their recommendations based on the increasing scientific evidence regarding a differential risk of VTE with COC with different gestagens, but Finland and Iceland still have no national guidelines.23 Compared with Norway, where levonorgestrel-containing COCs constituted a larger proportion than before, the share of the recommended products increased to a larger extent in Denmark, from 13% of overall sales of COCs in 2010 to 50% in 2013. Danish studies that showed an association between gestagens and VTE4 5 received more attention in Denmark than in the other Nordic countries, and this may explain the larger increase in this country. In Iceland, the total proportion of prescriptions of levonorgestrel-containing COCs increased; in Finland, it remained below 1%, contrasting with a slight decrease in Sweden.23 Compared with the other Nordic countries, the changes in the prescription pattern of COCs in Norway and Denmark following updated recommendations may be considered a success. Moreover, the increased proportion of prescriptions of levonorgestrel-containing COCs in Norway has probably led to a decreased incidence of VTE among young women, and this will be addressed in future studies.
Conclusion
The total proportion of starters who obtained levonorgestrel-containing COCs increased from 41% in 2008 to 80% in 2016, with the greatest increase from 2011 to 2012. All professions increased their proportion of prescriptions of recommended COCs, mainly among the youngest starters, with the highest compliance with recommendations observed among public health nurses and midwives. Norwegian health personnel do comply relatively well with the new recommendations, but general practitioners may prescribe a larger proportion of levonorgestrel-containing COCs to starters to further increase the population of users with the lowest risk of VTE.
Article summary
A large-scale national pharmacovigilance campaign had a major impact on the pattern of COC prescriptions in Norway.
References
Footnotes
Contributors JE did the literature review and wrote the first draft. FES did all the formal applications, organised the data and did the analysis. JE had full access to the data. JE and FES revised the manuscript and approved the final version for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The NorPD board reviewed the study protocol and gave permission for the use of data (PDB 1459, saksnr. 16/12041). According to Norwegian legislation, studies using anonymous data from nationwide registers are exempt from institutional regulatory board approval and written informed consent from patients.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.