Article Text

Abstract
Objective Evaluate effectiveness, harms and burdens of faecal blood testing, sigmoidoscopy and colonoscopy screening for colorectal cancer over 15 years.
Design We performed an update of a Cochrane systematic review, and performed network meta-analysis comparing randomised trials evaluating colorectal cancer screening with guaiac faecal occult blood test (gFOBT) (annual, biennial), faecal immunochemical test (FIT) (annual, biennial), sigmoidoscopy (once-only) or colonoscopy (once-only) in a healthy population, aged 50–79 years. We conducted subgroup analysis on sex. Follow-up >5 years was required for analysis of colorectal cancer incidence and mortality.
Results 12 randomised trials proved eligible. Compared with no-screening, we found high certainty evidence for sigmoidoscopy screening slightly reducing colorectal cancer incidence (relative risk (RR) 0.76; 95% confidence interval (CI 0.70 to 0.83) and mortality (RR 0.74; 95% CI 0.69 to 0.80), while gFOBT screening had little or no difference on colorectal cancer incidence, but slightly reduced colorectal cancer mortality (annual: RR 0.69; 95% CI 0.56 to 0.86, biennial: RR 0.88; 95% CI 0.82 to 0.93). No screening test reduced mortality nor incidence by more than six per 1000 screened over 15 years. Sigmoidoscopy had a greater effect in men, for both colorectal cancer incidence (women: RR 0.86; 95% CI 0.81 to 0.92, men: RR 0.75, 95% CI 0.71 to 0.79), and mortality (women: RR 0.85; 95% CI 0.71 to 0.96, men: RR 0.67; 95% CI 0.61 to 0.75) (moderate certainty).
Conclusions In a 15-year perspective, sigmoidoscopy reduces colorectal cancer incidence, while sigmoidoscopy, annual and biennial gFOBT all reduce colorectal cancer mortality. Sigmoidoscopy may reduce colorectal cancer incidence and mortality more in men than in women.
PROSPERO registration number CRD42018093401.
- PUBLIC HEALTH
- Gastroenterology
- GENERAL MEDICINE (see Internal Medicine)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first review on colorectal cancer screening including estimates from three of the major sigmoidoscopy screening trials after as long as 14.8 years of follow-up.
This is the first meta-analysis to assess the subgroup effect of sigmoidoscopy screening by sex from all four major sigmoidoscopy trials.
This review was conducted based on a a priori protocol, and designed by input from professionals and patient partners in a BMJ Rapid Recommendations guideline panel.
This review provides absolute risks in addition to relative estimates in a 15-year perspective after initial screening episode.
We only look at effects of screening in randomised controlled trials.
Introduction
Colorectal cancer is a major global health burden. It is the third most common cancer worldwide, and the second most cause of cancer-related deaths.1 Colorectal cancers may arise from precancerous lesions known as adenomas.2 Both adenomas and colorectal cancers can be visualised during sigmoidoscopy and colonoscopy. Even before symptoms occur, colorectal cancers might cause occult bleeding, which can be discovered by faecal blood tests known as guaiac faecal occult blood test (gFOBT) and the more recently developed faecal immunochemical test (FIT). gFOBT, FIT, sigmoidoscopy and colonoscopy are all used as screening methods for colorectal cancer.
Cancer screening are based on two different principles: early detection and prevention.3 Early detection of cancer enables treatment of cancer before it reaches an incurable state, and may thus reduce cancer mortality. Preventive cancer screening, on the other hand, is to detect and remove precursor lesions to cancers, such as colorectal adenomas. Thus, preventive screening may cause a reduction in both cancer incidence and subsequently mortality.3
Prior systematic reviews and meta-analyses evaluating the effectiveness of colorectal cancer screening showed that sigmoidoscopy screening reduces colorectal cancer incidence, while both sigmoidoscopy and gFOBT reduce colorectal cancer mortality.4–7 Recently, updates of three major trials on once-only sigmoidoscopy screening have been published: the UK Flexible Sigmoidoscopy Screening (UKFSST),8 the Norwegian Colorectal Cancer Prevention (NORCCAP)9 and the Prostate, Lung, Colorectal and Ovarian cancer (PLCO)10 trials. These updates provide estimates on reduced colorectal cancer incidence and mortality after a median follow-up of approximately 15 years or longer. In addition, these updates suggest a subgroup effect of screening on sex, with men experiencing greater reduction in both incidence and mortality than women.8–11
This is the first systematic review and meta-analysis including these updated results, and thus provides estimates for the risk of colorectal cancer incidence and mortality as long as 15 years after screening initiation. This review informed a clinical practice guideline, developed in parallel as a part of the BMJ Rapid Recommendations project, a collaborative effort from the MAGIC research and innovation programme (www.magicproject.org) and The BMJ. The aim of the project is to respond to new potentially practice changing evidence and provide a trustworthy practice guideline in a timely manner.12 Box 1 shows the articles linked to this BMJ Rapid Recommendation cluster.
Linked articles in this BMJ Rapid Recommendation cluster
Helsingen et al. Colorectal cancer screening with faecal immunochemical test, sigmoidoscopy or colonoscopy: a clinical practice guideline.16
Summary of the results from the Rapid Recommendation process.
Jodal et al. Colorectal cancer screening with faecal testing, sigmoidoscopy or colonoscopy: a systematic review and network meta-analysis.
Systematic review and network meta-analysis of all available trials that assessed colorectal cancer screening.
Buskermolen et al. Colorectal cancer screening with faecal immunochemical test, sigmoidoscopy or colonoscopy: a microsimulation modelling study.56
Modelled estimates of benefits and harms of screening after 15 years for different levels of baseline risk of colorectal cancer.
MAGICApp (http://magicproject.org/190220dist).
Expanded version of results with multilayered recommendations, evidence summaries and decision aids for use on all devices.
Methods
Protocol and registration
The protocol for this systematic review was registered with PROSPERO (CRD42018093401).13
BMJ Rapid Recommendations and patient involvement
According to the BMJ Rapid Recommendations process,12 a guideline panel provided critical oversight to the review. The panel identified populations, screening methods, subgroups and patient-important outcomes of interest a priori, based on most common screening practice today.14 15 The panel requested evidence in a 15-year perspective, as the recent publications that prompted the recommendations evaluated once-only sigmoidoscopy screening after approximately 15 years of follow-up. The panel included patient partners (individuals with experience of colorectal cancer screening), general practitioners, general internists, gastroenterologists, content experts in colorectal cancer screening, methodologists and a nurse practitioner. The patient partners were full members of the guideline panel, and contributed to the selection and prioritisation of outcomes together with the rest of the panel, under guidance of a patient liason. The panel members helped interpret the evidence in this review and make clinical practice recommendations.16
Search strategy
We updated a previously published Cochrane systematic review search.4 The search previously ended in November 2012, while we updated the search until 17 December 2018. A trained medical librarian searched MEDLINE, EMBASE and the Cochrane Central Register of Controlled Trials for published randomised controlled trials, with no language restrictions (online supplementary appendix 1). We reviewed reference lists from eligible new trials and related reviews for additional citations.
Supplemental material
Study selection
We imported all citations into Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia). Two reviewers (HCJ and LMH) independently screened titles, abstracts and full texts according to the eligibility criteria. Since this is an update of a previously published systematic review,4 we also screened the full texts of all the studies that were included and excluded at the full-text screening stage by the authors of the original review.
We considered all randomised controlled trials in any language comparing annual or biennial gFOBT or FIT, once-only sigmoidoscopy or once-only colonoscopy, compared with no-screening or to one another, in a healthy population aged 50–79 years, as requested by the panel.16 Outcomes of interest were colorectal cancer incidence and mortality, all-cause mortality, harms (bleeding, perforation, screening-related death and other major and minor complications as reported by trial authors) and burdens (need for further diagnostic workup including colonoscopy, procedure-related pain, psychological impact of a positive test and absence from work to prepare, perform and recover after the screening procedure).
Meta-analyses have shown that it takes at least 5 years from screening until an effect on colorectal cancer mortality or incidence can be observed.17 18 Thus, for analyses of colorectal cancer incidence and mortality, as well as all-cause mortality, we only included trials where follow-up was at least 5 years. Harms and burdens, on the other hand, are experienced during or soon after the screening procedure, and thus no follow-up restrictions were applied to the analyses of these outcomes.
Data extraction and rating of evidence
Two reviewers (HCJ and JCA) independently extracted data using a standardised form. From each eligible trial we collected the following information: study characteristics (study design, description of intervention, study period), description of participants (number, screening adherence, age and sex distribution), length of follow-up and outcomes data (events and numbers of patients included for analyses in each group). Reviewers had a third party available to resolve disagreement, however it was not needed. The authors of studies that did not report all outcomes of interest (eg, sex subgroups) were contacted.
Two reviewers (HCJ and LMH) independently assessed risk of bias using a modified version of the Cochrane tool,19 assessing the domains random sequence generation (selection bias), allocation concealment (selection bias), blinding (performance and detection bias), incomplete outcome data (attribution bias), selective reporting (reporting bias) and other bias. For each domain, the risk of bias was judged as low or high. Reviewers had a third party available to resolve disagreement, however it was not needed. We followed the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach to rate the certainty of evidence of estimates derived from pairwise and network meta-analysis.20 We rated direct, indirect and network meta-analysis (NMA) estimates separately. We used the lower certainty rating of the two pairwise estimates contributing as first-order loop for indirect comparisons.21 22 To rate the NMA estimates, we evaluated the ratings of the direct and indirect evidence and their coherence.21 22 Harms and burdens from screening will only occur in individuals attending screening, and is thus prognostic. Therefore, we evaluated the certainty of the evidence on harms and burdens using GRADE for assessment of evidence about prognosis.23
Data synthesis and analysis
Intention-to-treat numbers were used for all analyses regarding incidence and mortality. In one of the trials,9 the ratio of screened to control participant differed in different age groups (1:3 vs 1:5.4), thus the average age in the screened and the control groups differed. Therefore, these two age groups are analysed as two separate trials in this NMA. We performed standard pairwise comparisons of each screening intervention versus no-screening, using a restricted maximum likelihood approach to estimate relative risks (RR) with 95% CIs. Between-study variances were made equal, and correlations were set to 0.5. We examined statistical heterogeneity among studies using the Cochran Q-test (significant if p<0.10) and the between-study variance tau.2 Furthermore, an NMA applying mixed-treatment models based on a random-effects model in a frequentist framework was performed to compare the different interventions, using the mvmeta program and network graphs package for Stata.24 We report RRs for direct, indirect and network estimates and associated 95% CIs. We used the node-splitting approach for the assessment of loop inconsistency. We used the mean risk of events in the comparison groups to calculate the absolute effects of treatment in a 15-year perspective. We performed a sensitivity analysis including the 30-year follow-up of one of the gFOBT trials,25 and another sensitivity analysis excluding the PLCO trial,10 as this trial included a second sigmoidoscopy screening episode 3 or 5 years after the initial screening. As the length of follow-up varies between the studies, we also performed sensitivity analyses using person-years as the denominator rather than number of participants, and we report HRs for network estimates.
Subgroup differences in incidence and mortality between women and men were analysed using a fixed-effect meta-analysis. To further explore the effect modification for sex, we used a one-stage multilevel meta-regression model including screening intervention, sex and interaction term between sex and intervention as fixed-effect covariates, and study as a random-effect covariate. Furthermore, we fit a meta-analysis using only within-study comparisons, that is, pooling the risk differences (the deft approach).26 We excluded studies that did not report outcomes separately for men and women.
Harms and burdens as selected by the guideline panel were analysed using meta-analyses for binomial data using the metaprop_one Stata package modelling random effects and exact CIs. Analysis of psychiatric harms was not possible due to differences in reporting, and is therefore only descriptive. All numbers on harms and burdens are presented as proportions of patients who underwent screening, that is, per-protocol numbers.
We used Stata V.15.1 for all data analyses (StataCorp, College Station, Texas, USA). We followed the reporting standards set by Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA)27 and the PRISMA-NMA extension statement28 for all aspects of the review (online supplementary appendix 2).
Supplemental material
Results
Description of included studies
Our search yielded 8992 potentially relevant records. Combined with the result from the previously published review,4 a review of reference lists and updates of included trials published after our search was performed, a total of 12 different randomised trials described in 36 articles were included in this review (figure 1, table 1). Five trials included gFOBT screening, two included FIT screening, five included sigmoidoscopy screening and two included colonoscopy screening.
Characteristics of studies included in the systematic review

Preferred Reporting Items for Systematic reviews and Meta-Analyses flow diagram of study selection for systematic review and meta-analysis.27 RCT, randomised controlled trial.
The included trials enrolled a total of 1 325 618 participants, from Denmark, Italy, the Netherlands, Norway, Poland, Spain, Sweden, the UK and the USA, with follow-up ranging from 0 to 19.5 years for colorectal cancer incidence, and 0 to 30 years for colorectal cancer mortality. The age of invited participants ranged from 45 to 80 years, with an equal distribution of men and women. The gFOBT trials have reported results from 1 to 11 screening rounds, while the FIT trials, both still ongoing, have reported results from none to one screening round. One of the gFOBT trials performed annual screening, while five performed biennial screening.
The studies included in this review deviate slightly from the panel’s request for evidence on a healthy population aged 50–79 years, as two of the gFOBT trials included individuals from 45 years of age.29 30 In addition, one of the sigmoidoscopy trials included some participants who were screened twice,10 in contrast to the panel’s request for evidence on once-only sigmoidoscopy screening.
The trials varied in follow-up time after screening intervention, from 0 to 30 years. However, for the trials exceeding >5 years of follow-up, which were thus included in the analyses of incidence and mortality, the follow-up ranged from 10.5 to 30 years. One of the included trials25 had a maximum follow-up time substantially longer than the others (30 years vs 10.5–19.5 years), and we therefore chose to extract data from the 18-year follow-up of this trial.31 Thus, all trials had approximately 15 years of follow-up (range 10.5–19.5 years) for the analyses of incidence and mortality, which was also relevant to the guideline panel’s goal of providing 15 years estimates for different screening interventions.16
All trials had at least one criterion at high risk of bias. For the outcomes of incidence and mortality, only one report was assigned high risk of bias for incomplete data, due to a high withdrawal of consent from the participants.32 None of the trials were assigned high risk of bias for selective reporting of the outcomes incidence and mortality, but several were so for harms and burdens (figure 2, online supplementary appendix 3).
Supplemental material

Risk of bias summary for each clinical trial included in the systematic review.
Effects on incidence and mortality
Eight of the randomised trials had >5 years of follow-up, and were thus included in the analyses of incidence and mortality: four studies on gFOBT screening, and four on sigmoidoscopy screening (figure 3).

Network of included trials with available direct and indirect comparisons. The number next to each line is the number of studies comparing the connecting interventions. gFOBT, guaiac faecal occult blood test.
Sigmoidoscopy screening slightly reduced colorectal cancer incidence (RR 0.76; 95% CI 0.70 to 0.83) (figure 4) and colorectal cancer mortality (RR 0.74; 95% CI 0.69 to 0.80) (figure 5) compared with no-screening. In a 15-year perspective, this corresponds to a reduction of six (eight to four fewer) colorectal cancer cases per 1000 individuals screened, and a reduction of three (three to two fewer) colorectal cancer deaths per 1000 individuals screened. The certainty of evidence was high (table 2).
Relative and absolute NMA effect estimates for incidence and mortality in a 15-year perspective comparing the different screening interventions and no-screening

Effect of different screening interventions on colorectal cancer incidence shown as relative risks (RR) with 95% CIs. gFOBT, guaiac faecal occult blood testing.

Effect of different screening interventions on colorectal cancer mortality shown as relative risks (RR) with 95% CIs. FOBT, faecal occult blood testing.
gFOBT screening made little or no difference on colorectal cancer incidence compared with no-screening, neither annually nor biennially (annual: RR 0.86; 95% CI 0.72 to 1.03, biennial: RR 0.95; 95% CI 0.87 to 1.04) (figure 4). Colorectal cancer mortality was slightly reduced for both annual and biennial gFOBT screening compared with no-screening (annual: RR 0.69; 95% CI 0.56 to 0.86, biennial: RR 0.88; 95% CI 0.82 to 0.93) (figure 5). In a 15-year perspective, this corresponds to a reduction of one (three fewer to one more) colorectal cancer case and one (two to one fewer) colorectal cancer death per 1000 screened individuals when screened biennially, and a reduction of four (seven fewer to one more) colorectal cancer cases and three (four to one fewer) colorectal cancer deaths per 1000 screened individuals when screened annually. The certainty of evidence for comparisons involving biennial gFOBT screening was high (table 2). The certainty of evidence was downgraded for all comparisons involving annual gFOBT screening due to serious imprecision, as this evidence is based on estimates from only one trial and the rate of events is low (table 2). Direct and indirect estimates are available in online supplementary table 1A.
Supplemental material
Sigmoidoscopy screening slightly reduced colorectal cancer incidence (RR 0.80; 95% CI 0.71 to 0.91) (figure 4) and mortality (RR 0.85; 95% CI 0.77 to 0.93) (figure 5) compared with biennial gFOBT. In a 15-year perspective, this corresponds to an absolute reduction of six (eight fewer to three fewer) colorectal cancer cases and a reduction of two (three to one fewer) colorectal cancer deaths per 1000 individuals screened. The certainty of evidence was high (table 2).
Sigmoidoscopy compared with annual gFOBT screening probably had little or no difference on colorectal cancer incidence (RR 0.89; 95% CI 0.73 to 1.09) (figure 4) and mortality (RR 1.07; 95% CI 0.85 to 1.34) (figure 5), corresponding to an absolute reduction of three (seven fewer to two more) colorectal cancer cases, and an increase of one (one fewer to three more) colorectal cancer death per 1000 individuals screened in a 15-year perspective. The certainty of evidence was downgraded due to serious imprecision, as the evidence of the effect of annual gFOBT screening is based on estimates from only one trial and the rate of events is low (table 2).
Annual compared with biennial gFOBT screening probably has little or no difference on colorectal cancer incidence (RR 0.90; 95% CI 0.75 to 1.08) (figure 4), but probably reduced colorectal cancer mortality slightly (RR 0.79; 95% CI 0.64 to 0.98) (figure 5). In a 15-year perspective, this corresponds to an absolute reduction of three (seven fewer to two more) colorectal cancer cases, and three (four fewer to zero) colorectal cancer deaths per 1000 individuals screened. The certainty of evidence was downgraded due to serious imprecision, as the evidence of the effect of annual gFOBT screening is based on estimates from only one trial and the rate of events is low (table 2). Direct and indirect estimates are available in online supplementary table 1B.
All-cause mortality showed little or no difference among any of the screening interventions (online supplementary figure 1). For direct and indirect estimates, see online supplementary table 1A-B. The heterogeneity of the only loop in the network (annual gFOBT—biennial gFOBT—no-screening) could not be estimated due to insufficient observations, and reports of inconsistency are therefore abundant.
Sensitivity analyses including the 30-year follow-up of one of the gFOBT trials25 had no significant impact on the results. Sensitivity analysis excluding the PLCO trial10 on sigmoidoscopy screening (participants screened with sigmoidoscopy twice) had no significant impact of the results. A post hoc sensitivity analysis excluding the UKFSST trial8 on sigmoidoscopy was also performed, as this trial contributed to statistical heterogeneity in colorectal cancer incidence. This had no significant impact of the effect estimates, however moved the point estimates slightly towards the null. Therefore, this statistical heterogeneity was not considered a serious concern. Sensitivity analyses calculating hazard ratios (HR rather than RR, showed only minor differences, none of which affect the interpretation of the results (online supplementary figures 2-4).
Sex differences
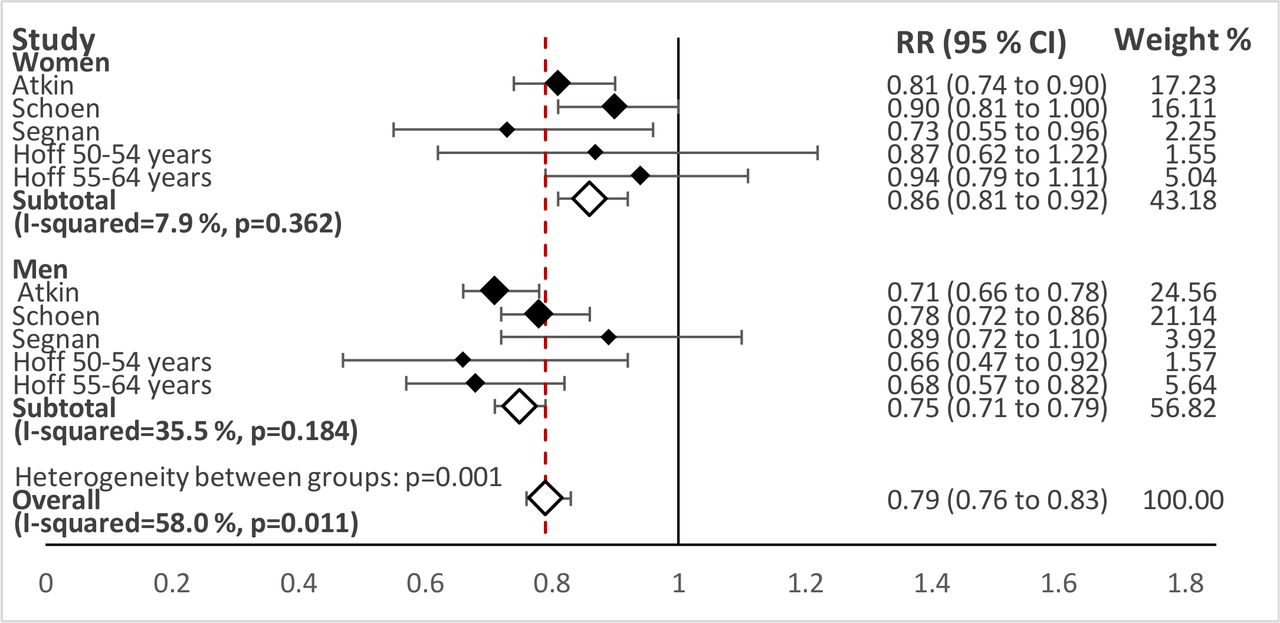
The subgroup analyses suggested a sex difference for sigmoidoscopy screening (table 3). Pairwise fixed-effect meta-analyses showed heterogeneity between the sexes for both colorectal cancer incidence (women: RR 0.86; 95% CI 0.81 to 0.92, men: RR 0.75; 95% CI 0.71 to 0.79, p=0.001) (figure 6) and mortality (women: RR 0.85; 95% CI 0.71 to 0.96, men: RR 0.67; 95% CI 0.61 to 0.75, p=0.006) (figure 7), but not for all-cause mortality (online supplementary figure 5). The one-stage multilevel model for sex and effect of sigmoidoscopy was statistically significant for interaction (incidence: p=0.001, mortality: p=0.015). Using the deft approach, we obtained similar results (colorectal cancer incidence risk difference 11% (95% CI 3% to 20%); colorectal cancer mortality risk difference 17% (95% CI 1% to 34%)). We assessed the credibility of these observed subgroup differences to be moderate (online supplementary table 2),33 supporting a greater relative effect of sigmoidoscopy in men than in women, for reducing colorectal cancer incidence and mortality.
Sex difference for sigmoidoscopy screening vs no-screening: relative and absolute NMA effect estimates for incidence and mortality in a 15-year perspective

Sex differences on colorectal cancer incidence with sigmoidoscopy screening compared with no-screening. RR, relative risk.

Sex differences on colorectal cancer mortality with sigmoidoscopy screening compared with no-screening. RR, relative risk.
Harms and burdens
The gFOBT trials reported harms in different ways: three of the trials34–37 reported harms summarised after several screening rounds where only those who had attended the previous screening episode were re-invited, while the two other trials38 39 reported harms and total number of screening tests where all randomised participants were re-invited even though they chose not to attend the first or previous screening episodes. We therefore pooled the harms and burdens events from gFOBT screening trials data in two groups: 1) reported as a total from two to five screening rounds and 2) reported per performed screening test, assuming that harms and burdens were independent of the screening round. The sigmoidoscopy trials reported harms and burdens from the screening procedure including subsequent workup. Due to the differences in reporting, we were not able to pool estimates across screening interventions. All trials reported the total number of events. None of the trials, regardless of screening intervention, have reported harms and burdens following surveillance procedures.
Perforation and bleeding requiring hospitalisation
Eight out of the total of 11 trials reported on bleeding requiring hospitalisation and nine reported on perforations after screening, either from the screening procedure itself or subsequent workup. The risk of bleeding in the sigmoidoscopy trials was 3 (1–6) per 10 000 (0.03%; 95% CI 0.01% to 0.06%) screening attenders, while for colonoscopy it was 17 (12–23) per 10 000 (0.17%; 95% CI 0.12% to 0.23%) (figure 8). The risk of bleeding in the gFOBT trials were none (zero to one) per 10 000 (0.00%; 95% CI 0.00% to 0.01%) screening attenders in the trials reporting harms per two to five screening rounds, while it in the trial reporting harms per screening test was one (zero to one) per 10 000 screening tests (0.01%; 95% CI 0.00% to 0.01%) (figure 8). The risk of bleeding in the FIT trial was eight (3–14) per 10 000 (0.08%; 95% CI 0.03% to 0.14%) screening tests (figure 8). The risk of colorectal perforation in the sigmoidoscopy trials was three (one to four) per 10 000 (0.03%; 95% CI 0.01% to 0.04%) screening attenders, while for colonoscopy it was one (zero to three) per 10 000 (0.01%; 95% CI 0.00% to 0.03%) (figure 9). The risk of perforation in the gFOBT trials were one (one to two) per 10 000 (0.01%; 95% CI 0.01% to 0.02%) screening attenders in the trials reporting harms per two to five screening rounds, while it in the trial reporting harms per screening test was zero (zero to one) per 10 000 screening tests (0.00%; 95% CI 0.00% to 0.01%) (figure 9). The risk of perforation in the FIT trial was zero (zero to three) per 10 000 (0.00%; 95% CI 0.00% to 0.03%) screening tests (figure 9). The certainty of evidence for all screening interventions was downgraded to moderate due to risk of bias (online supplementary table 3A-B). The certainty of evidence for the gFOBT trials and FIT trial was downgraded further due to indirectness, with differences in the number of screening rounds (online supplementary table 3B and C).

Risk of bleeding requiring hospitalisation after screening and workup procedure shown as percentage of screening attenders with 95% CIs, unless otherwise mentioned. gFOBT, guaiac faecal occult blood test; FIT, faecal immunochemical test.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk of colorectal perforation after screening and workup procedure shown as percentage of screening attenders with 95% CIs, unless otherwise mentioned. gFOBT, guaiac faecal occult blood test; FIT, faecal immunochemical test.
Other physical harms and burdens
The mean risk of needing further workup due to findings at screening varied: 13% (95% CI 5% to 26%) in sigmoidoscopy trials, 7% (95% CI 7% to 8%) per screening test in the FIT trial, 5% (95% CI 5% to 5%) per screening test in gFOBT trials and 6% (95% CI 4% to 9%) per two to five gFOBT screening rounds (table 4 and supplementary table 3A-B). The confidence in the estimate of effect was downgraded to moderate certainty due to indirectness, resulting from differences in the number of screening rounds (gFOBT), and the differences in definitions of a positive screening test (online supplementary table 3A-B).
Harms and burdens
Surveillance of individuals with high-risk adenomas is recommended.40 The trials did not report the findings of high-risk adenomas consistently, however, we referred to reported adenoma characteristics and the European Society of Gastrointestinal Endoscopy guidelines to estimate surveillance need.40 We approximated those that will require surveillance as 1% (95% CI 1% to 2%) of screening attendees per two to five rounds with gFOBT screening, 2% (95% CI 2% to 3%) of screening attendees per FIT performed, 4% (95% CI 3% to 5%) of sigmoidoscopy screening attendees and 10% (95% CI 10% to 11%) of colonoscopy screening attendees (table 4 and supplementary table 3A-B). The certainty of evidence for all screening interventions was downgraded to moderate due to differences in reporting of the findings at screening or subsequent workup. The certainty of evidence from the gFOBT trials was further downgraded to low, due to differences in number of screening rounds. The certainty of evidence from the sigmoidoscopy trials were further downgraded to low, due to failure to report how information was obtained (online supplementary table 3A-B).
Other patient-important harms and burdens
All four sigmoidoscopy screening trials published reports on procedure-related pain,41–44 where 16% (95% CI 10% to 22%) reported moderate-to-severe pain during the procedure (online supplementary figure 6). Only one of the colonoscopy trials45 published a report on pain related to the procedure, where 21% (95% CI 19% to 22%) reported severe-to-moderate pain during the procedure, although no relation to sedation or air/CO2 insufflation was reported (online supplementary figure 6). The certainty of evidence of pain in sigmoidoscopy was downgraded to low certainty, due to probable selection bias in those who answered the questionnaires, as well as inconsistency between the trials (online supplementary table 3A). The certainty of evidence of pain in colonoscopy was high (online supplementary table 3B).
We identified four reports on the psychological impact of a positive screening test, two from sigmoidoscopy,46 47 and one from each gFOBT48 49 and FIT.47 One report on sigmoidoscopy screening46 used the short version of the Spielberger State-Trait Anxiety Inventory (STAI)50 to ask participants if they were worried about bowel cancer before and 3 months after sigmoidoscopy screening, and reported no significant psychological harms associated with positive screening results. One report on gFOBT screening48 measured anxiety using the original STAI, and reported that anxiety scores in a sample of 100 screening test false-positive patients were highest after the notification of a positive test, fell after a negative workup colonoscopy, and subsequently remained low. There were no data on the individuals who had a positive test, but did not attend the workup colonoscopy.
Another report on gFOBT screening49 measured worry at different time points during the screening process by using a questionnaire where the screening attenders reported their worry on a five-point scale ranging from ‘not at all’ to ‘extremely’. Sixty per cent reported to be extremely or very worried after receiving a positive gFOBT screening test result, an increase of 44 percentage points from when first receiving the invitation to screening. Concurrently, 15% reported negative effects on daily life ‘to a great deal’ when receiving the positive test result, compared with 5% when receiving the invitation to screening.
The most recent study, on sigmoidoscopy and FIT screening,47 reported no significant increase in anxiety and depression on the Hospital Anxiety and Depression Scale51 after a positive result in either sigmoidoscopy or FIT, neither before or after the workup colonoscopy, regardless of colonoscopy result.
We also searched for data on absence for work to prepare for, attend and recover after the screening, as decided a priori by the guideline panel, but no data were identified in the included randomised trials.
Discussion
Statement of principal findings
Screening with gFOBT or sigmoidoscopy slightly reduced colorectal cancer mortality in a 15-year perspective, based on high certainty evidence. Neither gFOBT nor sigmoidoscopy screening, however, had any effect on all-cause mortality. The absolute effects will depend on the baseline risk of the screening attenders, thus in the trials the absolute effect was one less colorectal cancer death per 1000 (0.1%) individuals screened with gFOBT biennially, and three fewer colorectal cancer deaths per 1000 (0.3%) individuals screened with gFOBT annually or once-only sigmoidoscopy.
Sigmoidoscopy screening also slightly reduced colorectal cancer incidence, based on high certainty evidence, where the absolute effect observed in the trials was six fewer colorectal cancer cases per 1000 (0.6%) individuals screened in a 15-year perspective. We found no significant difference between annual gFOBT and sigmoidoscopy screening on colorectal cancer incidence, but the certainty of evidence is moderate, as annual gFOBT has been evaluated in only one trial where rate of events is low. Biennial gFOBT had no effect on colorectal cancer incidence.
Compared with annual or biennial gFOBT, or no-screening, sigmoidoscopy is the most effective method for decreasing both colorectal cancer mortality and incidence in a 15-year perspective. However, sigmoidoscopy has a greater relative effect in men than in women: five fewer colorectal cancer cases and three fewer colorectal cancer deaths per 1000 (0.5% and 0.3%) screened individuals in men compared with in women. The reasons behind the greater relative effect in men than in women is unknown. Sigmoidoscopy screening focuses on the detection of adenomas, one of the precursors to colorectal cancer.2 52 53 Men have a higher risk of developing adenomas, and colorectal cancers in women may more frequently develop from a different pathway, such as sessile serrated adenomas.54 With increasing evidence that there is a difference in the relative effect of sigmoidoscopy screening between men and women, this should be studied further.
The certainty of the evidence on harms and burdens reported in the randomised trials was downgraded mainly due to high risk of bias, as none of the trials reported how the data were collected. Bleeding requiring hospitalisation and colorectal perforations after screening or subsequent workup occurred in between one and three per 10 000 (0.01% to 0.03%) individuals screened. Moderate-to-severe pain was reported by approximately one in five (16%–21% dependent on screening method) individuals undergoing endoscopic procedures. Screening attenders receiving a positive screening test experienced immediate anxiety, but no sustained psychological effects are shown. However, information on individuals choosing not to attend the workup procedure is not found.
Strengths and limitations of the study
This review has several strengths: first, the review was conducted based on an a priori protocol, based on the Cochrane and GRADE approaches.19–23 Second, outcomes were informed by input from professionals and patient partners in the BMJ Rapid Recommendations guideline panel. Third, the study is based on a comprehensive systematic search of several databases, and it is unlikely that we have missed any ongoing or previously performed trials. Finally, this review, in addition to showing relative effects of the screening interventions, also quantifies the absolute risks, as compared with the average control population in the studies, in a 15-year perspective. This enables the reader to interpret the effects more easily.
The major limitation of this study is that we only look at harms and burdens of the screening interventions in randomised trials. As none of the randomised trials are designed for collecting data on the harms and burdens and do not report how data on harms and burdens were obtained, observational trials might provide further information on these outcomes. In addition, the absolute effects calculations are based on the mean risk of colorectal cancer incidence and mortality in the control groups of the different trials, which varies between the different trials. This might be due to the different calendar times at which the trials were performed, in addition to differences between the control groups of the different trials. All absolute risk reduction estimates assume that all individuals have mean risk. This is a strong assumption in the individual perspective, but represent the mean absolute effect in our target population of healthy individuals aged 50–79 years.
Findings in relation to other studies
Prior reviews show that sigmoidoscopy screening reduces colorectal cancer incidence, while both sigmoidoscopy and gFOBT reduce colorectal cancer mortality.4–7 This is the first review that includes follow-up from three of the major sigmoidoscopy trials exceeding 14.8 years,8–10 and we show that there is sustained effect of once-only sigmoidoscopy screening even 14.8 years after screening. This is also the first review that performs a network meta-analysis comparing the different screening test against one another with this long follow-up.
In addition, this is the first meta-analysis assessing the subgroup effect of sigmoidoscopy screening by sex with data from all four major sigmoidoscopy trials after 14.8 years of follow-up, demonstrating that there is a greater relative effect of reduction of both colorectal cancer incidence and mortality in men than in women.
Implications for clinicians and policy makers
Our review shows that sigmoidoscopy screening slightly reduces colorectal cancer incidence even 15 years after a once-only screening. Sigmoidoscopy, annual and biennial gFOBT all slightly reduce colorectal cancer mortality in the same time perspective. Sigmoidoscopy is likely to be more effective in men than in women both for colorectal cancer incidence and mortality. None of the screening interventions show effect on all-cause mortality. These results show that the relative effect of once-only sigmoidoscopy screening is maintained as long as 15 years after screening. Most guidelines today recommend rescreening 5–10 years after initial screening. This may now be safely extended to 15 years.
Harms and burdens were reported with large variation. The frequency of testing (annual or biennial for faecal blood tests) is important in the evaluation of possible harms and need of surveillance, as more frequent testing is likely to increase the rate of harms. The need for future surveillance reported in this study must be viewed critically for implications in contemporary practice, in particularly for gFOBT, where studies used sigmoidoscopy and barium contrast enemas, instead of colonoscopy, as the primary workup strategy after a positive screening test.
All trials on colorectal cancer screening mainly have participants of European origin, and there is paucity of data for other ethnicities.
Unfortunately, there are no reports on long-term effects on colorectal cancer incidence and mortality of FIT and colonoscopy. Colonoscopy and FIT both have higher sensitivity than gFOBT and colonoscopy, and are therefore likely to have a larger effect on incidence and mortality.55 However, these benefits must be weighed against increased harms and burdens such as more individuals in need of colonoscopy surveillance.
This review supported the development of an evidence-based clinical practice guideline, as reflected in the accompanying Rapid recommendations guideline.16
Acknowledgments
The authors would like to thank Marte Ødegaard, Senior librarian and Hilde Strømme, adviser, at the Medical library, University of Oslo, for performing the literature search.
References
Footnotes
Contributors HCJ drafted the protocol and the first draft of the review. HCJ, LMH and JCA performed data extraction. HCJ and LMH assessed risk of bias of included studies. HCJ and LE performed the statistical analyses. PV and LE supervised the study. HCJ, LMH, JCA, LL, PV and LE participated in writing the manuscript, interpretation of results and approval of the final version of the review. Corresponding author HCJ is the guarantor.
Funding The present work was funded by a PhD grant from the Norwegian Research Council (grant no 231920/F20). The default licence, a CC BY NC licence, is needed.
Disclaimer The funding sources had no role in the design, conduct or reporting of the study.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure and declare: no support from any organisation for the submitted work. POV is a member of the GRADE working group. JCA routinely see individuals eligible for colorectal cancer screening and is a co-writer on the American College of Gastroenterologists 2008 colorectal cancer screening guidelines. He is a member of the ACG, AGA, ASGE and the US Multi-Society Task Force for Colorectal Cancer Screening.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data available.