Article Text

Abstract
Introduction Metabolically healthy obese phenotype (MHO) refers to obese individuals with an adequate metabolic profile and absence of metabolic syndrome. Many prospective studies have reported the benign condition relating the MHO phenotype and its potential role in reducing risk of cardiovascular disease, total cancer, and all-cause and cause-specific mortality. However, inconsistent results were found and the question remains controversial. We aim to conduct a systematic review and meta-analysis to clarify the associations these associations from relevant prospective studies.
Methods and analysis The Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Protocols 2015 statement was used to prepare this protocol. MEDLINE, Web of Science databases, EMBASE and Cochrane Database will be used for literature search from their inception up to December 2019 with restriction of published studies in English. Published prospective studies reporting adjusted relative risk (RR) estimates for the association between MHO phenotype and cardiovascular disease, total cancer, all-cause or cause-specific mortality will be included. The process of study screening, selection and data extraction will be performed independently by two reviewers, and the risk of bias for the studies included will be assessed using the Newcastle-Ottawa Quality Assessment Scale. HRs or RRs for disease events and mortality with 95% CIs will be considered as primary outcomes, and summary HRs/RRs will be pooled using random-effects models. The Cochrane’s Q and the I2 statistics will be used to assess and quantify heterogeneity, respectively. Subgroup analysis will also be carried out according to study characteristics to investigate potential sources of heterogeneity.
Ethics and dissemination As this meta-analysis is performed based on the published studies, no ethical approval and patient safety considerations are required. The findings of the study will be reported and submitted to a peer-reviewed journals for publication.
PROSPERO registration number CRD42019121766.
- obesity
- metabolic health
- cardiovascular disease
- mortality
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This review is anticipated to be the first comprehensive meta-analysis of prospective studies to address the metabolically healthy obesity (MHO) to the risk of coronary heart disease, stroke, cardiovascular disease, total cancer and all-cause mortality as well as less common causes of death.
This systematic review and meta-analysis will provide a more up-to-date and comprehensive assessment of the MHO and several health outcomes.
This meta-analysis has a comprehensive literature search strategy involving restriction of studies to prospective studies, and will ensure that both the risk of bias and the quality of evidence of the included studies is properly assessed by Cochrane risk of bias assessment tool and Newcastle-Ottawa Quality Scale, respectively.
Only included studies written in English may lead to publication bias.
Introduction
Obesity is now one of the major public health problems and becomes a worldwide epidemic in the past four decades. Its prevalence has risen globally from 3.2% to 10.8% in adult men and from 6.4% to 14.9% in adult women in the same period.1 The excess body weight was estimated to affect nearly 2 billion people, and accounted for approximately 4 million deaths and 120 million disability-adjusted life years.2 3 Obesity is a well-established risk factor for a great number of cardiovascular diseases (CVDs) and metabolic disorders,4–6 and also has been shown as the main cause of CVD, cancer mortality and all-cause mortality.7–10 However, obese people may vary in their body fat distribution and cardiometabolic profiles, thereby their association with morbidity and mortality could be heterogeneous in the obese people.11 12 In this context, recent search focused on a novel subgroup of obese individuals who seem to have an adequate metabolic profile and do not have metabolic syndrome (MetS)while being categorised as obese, referred as metabolically healthy obese (MHO).13 14 Multiple studies showed that MHO phenotype accounted for as much as 10%–50% of the obese adults, depending on the population and the criteria used to ascertain metabolic health.12 15 A very recent meta-analysis of 40 population-based studies reported an overall prevalence of 35% among obese adults.16
The extent to which the MHO phenotype is the benign condition and is associated with a lower risk of adverse health outcomes and all-cause mortality remains controversial. Some studies have confirmed a protective effect and no increased risk of CVD and mortality among MHO individuals, particularly compared with at-risk obese17–19; whereas several other studies have shown a higher risk of CVD, cancer incidence and mortality in this group compared with metabolically healthy normal weight (MHNW) individuals.20–22 For instance, a 10-year follow-up study of 25 626 women aged 45 years and more found no increased CVD risk for MHO individuals,23 a finding replicated in a 15-year follow-up Italian study of obesity and insulin sensitivity.24 In contrast, another study showed that overweight and obese individuals without the MetS had an increased risk of CVD compared with MHNW individuals after a 17-year follow-up, a finding justified by using five different metabolic health definitions.25 It is important to note that inconsistent results depend on study design, population, follow-up time and MHO definition used. Several meta-analysis studies have investigated this ongoing controversy26–28; however, the reliability of summarised evidences was questionable due to methodological constraints. Some roughly merged the incidents of CV events and all-cause mortality together instead of differentiating these two outcomes, some calculated the pooled risk estimate based on unadjusted risk estimates, and some only considered MetS as MHO definitions, resulting in a limited number of analysed studies.26 27
Another two recent meta-analyses reported that, compared with participants with MHNW, those with MHO were at higher risk of cardiovascular events but not all-cause mortality.28 29 The systematic review and meta-analysis by Eckel et al is particularly important because it was the first to carefully consider the full range of possible definitions of metabolic health,28 and this aspect is crucial when addressing the role of this complex condition for the prediction and prevention of cardiometabolic diseases and possibly of certain types of cancer.30 Besides, the meta-analysis conducted by Eckel et al extended literature search to include only prospective studies with strict standard of reference groups considered, and perform a comprehensive subgroup analyses.28 The meta-analysis conducted by Zheng et al ,29 including a large sample size, enabled the determination of a robust and reliable risk estimates of CV events and mortality for MHO individuals by using both raw data and fully adjusted effect sizes from original studies, but these two aforementioned meta-analysis study were not up to date, with their literature search until April 2014 and September 2015, respectively, and since then, according to our general search, there are more than 17 new publications investigating MHO and health outcomes between 2016 and 2019. More importantly, the association with cancer events and various cause-specific mortality is still scarce.
Objectives
The protocol study is designed to establish an explicit methodology for systematically and comprehensively conducting a review evidence and meta-analysis, and the aim is to (1) clarify whether is there an increase in risk of developing CVD, total cancer, and all-cause and cause-specific mortality in adults with MHO, compared with their MHNW peers and (2) to define more accurate estimates of risk.
Methods and analysis
Registration and review design
The procedure for this study will be conducted in accordance with the guidelines provided by the Preferred Reporting Item for Systematic Reviews and Meta-analyses Protocols (PRISMA).31
Search strategy
A literature search will be undertaken using the following electronic databases: MEDLINE (via PubMed), ISI Web of Knowledge databases, EMBASE and the Cochrane Database to identify published studies. The databases will be searched from their inception to December 2019. In addition, the literature search will be later updated and supplemented through the manual review of reference list of obtained articles. The following search terms will be used as keywords or (and) medical subject headings (MeSH) terms in the electronic search: body mass index (BMI), obesity, metabolic, metabolically, healthy, MetS, CVD, risk, mortality, cause of death. Details of search terms and strategy for MEDILINE are provided in table 1, and this strategy will be adapted to suit other databases.
Proposed search terms
Inclusion criteria
All prospective studies of MHO and incidence or mortality from coronary heart disease (CHD), stroke, CVD, total cancer, and all-cause and cause-specific mortality will be considered eligible and included if they meet the following criteria:
The study design is a prospective cohort study;
MHO and other obesity phenotypes (eg, MHNW and metabolically unhealthy obese (MUO)) are defined according to the cross-classification of obesity criteria and metabolic health status. Obesity is defined using BMI, waist circumference (WC) or body fat per cent; metabolic health status is defined using any of the following published MetS criteria: the Adult Treatment Panel-III (ATP-III)-based criterion (including any extended or modified ATP-III criteria), the International Diabetes Federation (IDF) criteria, Joint Interim Statement (JIS) criteria, Harmonised MetS criteria, the Wildman criteria, the Karelis criteria, insulin resistance (IR)—or risk score-based criteria (eg, the Homoeostasis model assessment of IR (HOMA-IR) index of having HOMA-IR in the upper quartile of the HOMA index and the triglyceride-glucose (TyG) index of having TyG >8.82/8.73 for men/women) or other cardiometabolic clusterings.
The main outcomes of interest are CHD (total CHD or major coronary event, non-fatal myocardial infarction (MI), any MI, fatal MI, incident ischaemic heart disease, fatal ischaemic heart disease, acute coronary syndrome), stroke (total stroke, ischaemic, haemorrhagic, intracerebral and subarachnoidal haemorrhage), total CVD (CHD and stroke combined), and total cancer and all-cause mortality; the secondary outcomes will be cause-specific mortality from any cause of death.
Outcomes are measured by multivariate Cox proportional hazards models, and the relative ratio (RR) or HR and the corresponding 95% CI are reported.
Population of adults or participants are aged 18 years and older.
Studies are published in English.
Study selection
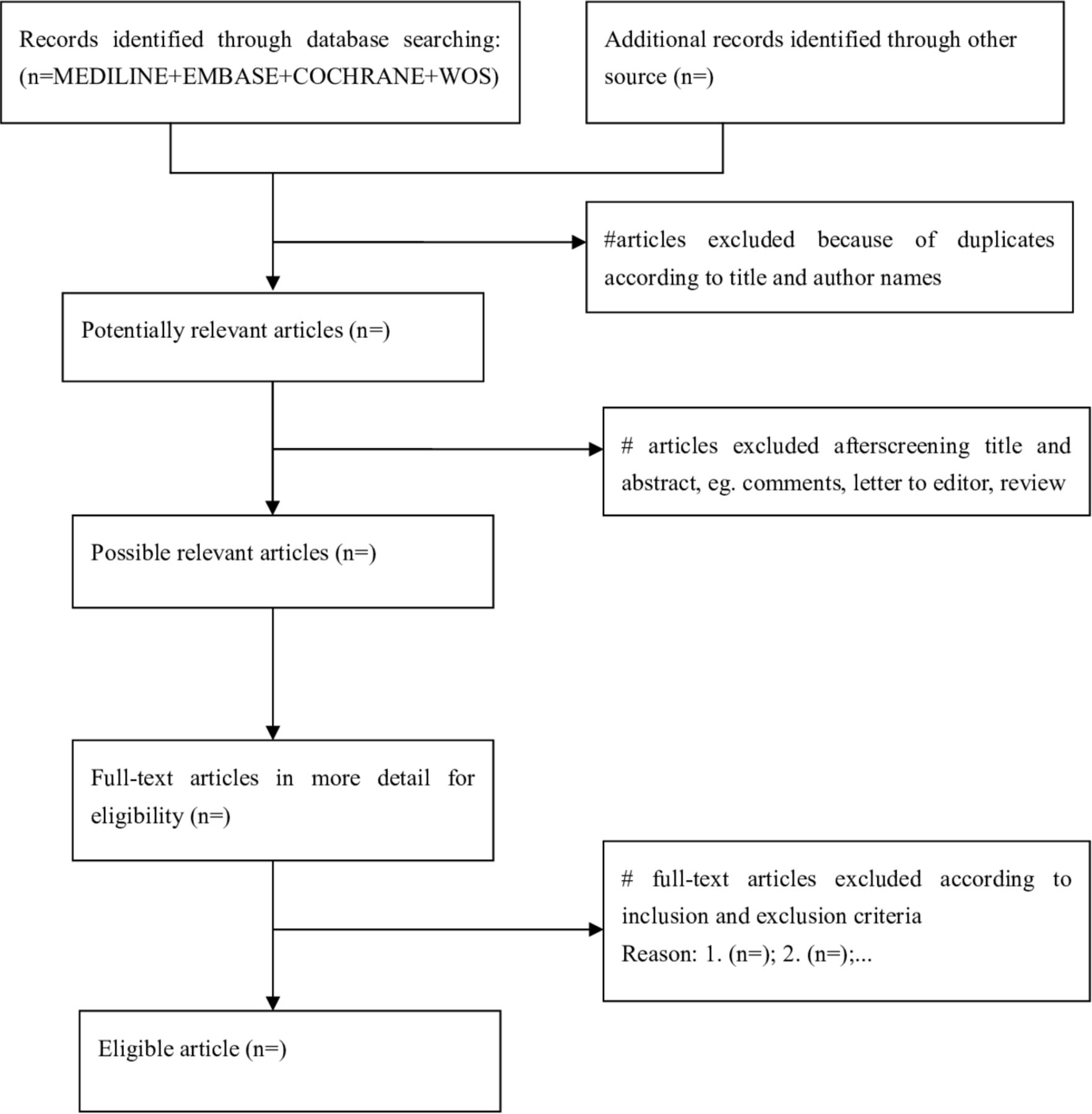
All investigators will be properly trained prior to data screening task. Two review author (KL and HD) will first screen the title and abstract of the searched studies independently and in duplicate to assess the eligibility of the searched studies. Then, all potentially eligible studies will be retrieved and the same review authors will review full-text articles for inclusion, according to prespecified inclusion criteria. When disagreements occur, it will be resolved by group discussion or, if required, a third author (AF) will be consulted to evaluate the full text and the discrepancy. In addition, excluded studies and the rationale for exclusion will be documented. Figure 1 depicts the study selection processes in a PRISMA flow diagram.
{kind=link}
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart of study selection.
Data extraction
We will extract results and study characteristics into tables using a standardised data collection form from eligible studies. Information that needed to be extracted will be as follow: first author’s name, year of publication, country or region, duration of follow-up, study location, sample size and number of events or deaths, gender proportion and age at baseline year, baseline MHO sample size, MHO definition, adjustments or covariates in the models, outcomes, the size of the association (HRs, RRs or ORs with 95% CI). We compared the risk of having various health outcomes, such as mortality and CVD events, and calculate the pooled risk estimates for the MHO, metabolically unhealthy normal weight (MUNW) and MUO phenotypes using MHNW participants as the reference. If one article contained several obesity and metabolic health definitions, we will treat each definition as an independent one. It is noteworthy mentioning that several studies revealed that MUNW individuals, even though with a normal BMI range, was unexpected associated with higher risk of all-cause mortality and/or cardiovascular events.26 In this regard, Stefan et al provided a comprehensive review and data addressing to what extent major risk phenotypes determine metabolic health in lean compared with overweight and obese people and provide support for the existence of a lipodystrophy-like phenotype in the general population.32 Therefore, for the sake of integrity of the study, the risk of MUNW and other obesity phenotypes with health outcomes will also be summarised in the present study.
The data extraction will be independently conducted by KL and HD, and be checked for accuracy by AF. All disagreements will be settled by discussion until a consensus is reached. In case of lacking key information, authors of primary studies will be contacted and consulted for obtaining missing data.
Study quality assessment
Study quality of included studies will be assessed by the Newcastle-Ottawa Quality Scale (NOS) adopted for cohort studies,33 and this scale awards 0–9 score points based on the selection, comparability and outcome assessment. Specifically, the NOS includes the following criteria with associated points: (1) representativeness (*); (2) selection of non-exposed cohort (*); (3) exposure-ascertainment (*); (4) demonstration of outcome not present at start (*); (5) adjustment for age/adjustment for any other factor (**); (6) assessment of outcome (*); (7) long enough follow-up (*) and (8) adequacy of follow-up (*). We will consider studies with 0–3, 4–6 and 7–9 points to represent low, medium and high-quality studies, respectively. The study quality will be independently assessed by two reviewers (KL and HD), and if any discrepancies, we will resolved by group discussion or consultation from with a third reviewer.
Data synthesis and statistical analysis
Once the data extraction has been completed, we will conduct the statistical analysis. All statistical analyses will be done with R V.3.2 software (R Foundation for Statistical Computing, Vienna, Austria)34 and ‘metafor’ package of R.35 In the present meta-analysis, the HR with its 95% CI will be as a common measure of incidence or mortality from CHD, stroke, total CVD and total cancer, and of all-cause mortality for the MHO group compared with the MHNW group (the reference group). For studies that reported several multivariable-adjusted HR, we will use the most fully adjusted for potential confounders in the meta-analysis. Heterogeneity between studies will be evaluated using the Cochrane’s Q and Higgins I2 statistics, respectively.36 For the Q statistic, a p §amp;lt; 0.1 is considered to be significant, and I2 values of 0, 25, 50% and 75% represent no, low, moderate and high heterogeneity, respectively. Either fixed-effects or random-effects models, depending on heterogeneity magnitude, will be applied to calculate the summary risk estimates and 95% CI for outcomes in the MHO group. In the fixed-effect model, the pooled HR is obtained by averaging the lnHR (HR value in log scale) weighted by the inverses of their variances.37 In the random-effect model, the DerSimonian-Laird method is used to further incorporate between-study heterogeneity.38
The sensitivity analyses will also performed when MetS was used for metabolic health criteria. In literature, several studies defined metabolic health by the absence of all metabolic factors, and this stricter definition may lead a different conclusion.28 This findings were consistent with a very recent evidence based on the large European Prospective Investigation into Cancer and Nutrition study (CVD).39 In this case-cohort analysis including 520 000 Europeans after a median follow-up of 12.2 years, Lassale et al found that the MHO phenotype, defined as none of MetS component, was not associated with increased risk of CHD (HR, 1.21, 95% CI 0.76 to 1.92) whereas MHO individuals were at higher risk of CHD with loose definition of MetS (HR 1.28, 95% CI 1.03 to 1.58).39 For the sake of the integrity of the study and comparability with other meta-analysis, we will also perform additional sensitivity analyses with different definitions of metabolic health when MetS criteria were used: excluding the WC criterion from the definition of MetS, modifying the definition of MH to be <2 abnormalities; and defining MH participants as having none of four possible abnormalities (elevated blood pressure, triglyceridaemia, hyperglycaemia, low HDL cholesterol).
Subgroup analyses
In case of substantial heterogeneity, subgroup analyses will be further performed to investigate the potential source of between-study heterogeneity using following variables: gender (men and women), model adjusted for physical activity (PA) (no vs yes), follow-up duration (<5, 5–10 and >10 years), participant’s age at baseline (<50 and ≥ 50 years), criterion used to define metabolic health (ATP-III, JIS or IDF, HOMA vs others), geographical location (Asia, Europe, North America, others), sample size (<5000, 5000–10000, >10 000) and study quality (0–3 stars, 4–6 stars, 7–9 stars).
It is noteworthy mentioning that among various factors, PA and/or cardiorespiratory fitness (CRF) has been recognised as a novel characteristic of the MHO, as well as play an important role in MHO prognosis.40 Specially, based on Aerobics Center Longitudinal Study,40 MHO individuals have a significantly higher CRF level than the individuals with MUO, and these findings have been confirmed by recent meta-analysis of Ortega et al that MHO, compared with MUO, have higher levels of PA, lower levels of sedentary behaviour and higher levels of CRF.41 Recently, Lavie et al provided a state-of-the-art review on the causes of obesity and effective modalities for this prevention, and the importance of fitness and lifestyle consideration to protect MHO from CVDs.40 Therefore, the impact of PA/CRF will be taken into account in the subgroup analysis for the prognosis of future all-cause mortality and other health outcomes in MHO individuals compared with MHNW.
It is also important to recognise that follow-up duration is a critical element in evaluating low-risk populations for the future events. Several studies observed that an increased risk of adverse clinical outcomes occurred only after 8–10 years of follow-up,42 43 which suggests a transient nature of the MHO phenotype. Indeed, based on a large-scale Nurses’ Health Study including 90 257 women, Eckel et al found that after 30-year follow-up, the majority of MHO converted to unhealthy phenotypes, and among those who maintained MHO status during follow-up were still at a higher CVD compared with their MHNW peers (HR 1.57, 95% CI 1.03 to 2.38).44 In this regard, whether or not MHO is a benign obesity phenotype may be impacted on the length of follow-up; thus, the duration of follow-up is another important factor to take into account in the subgroup analysis.
Furthermore, a sensitivity analysis will be conducted by removing one study in each turn, the rest of the studies are analysed to investigate the robustness of the findings.45 Potential publication bias will be assessed with the aid of the Egger’s rank and regression test,46 47 and the visual assessment of funnel plots will also be used if there are sufficient studies (10 or more) in the meta-analysis.48
Patient and public involvement
Patients and/or the public were not directly involved in the design or planning of the study.
Potential protocol amendments
The current protocol as written will not be modified in the course of the study. However, any modification will be concisely described in the final review.
Dissemination
The findings of the study will be reported according to the PRISMA-compliant guidelines and submitted to a peer-reviewed journals for publication and also presented at conferences.
Acknowledgments
The authors would like to thank the experts from Native EE for invaluable assistance in English language editing.
References
Footnotes
Contributors ST designed the study protocol and registered the protocol on the PROSPERO database. YL and AF drafted the manuscript. KL and HD tested the feasibility of the study. AF will perform the data collection and analyses. ST revised and finalised the study protocol. All authors reviewed and approved the final manuscript for submission.
Funding This research was funded by National Natural Science Foundation of China (81803329) and China Postdoctoral Science Foundation (2018M631780).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study will not conduct a primary data collection, but will only include previous published studies. Therefore, no ethical approval will be required.
Provenance and peer review Not commissioned; externally peer reviewed.