Article Text

Abstract
Objectives Modifying lifestyle can prevent the progression of chronic kidney disease (CKD) but the specific elements which lead to favourable behaviour change are not well understood. We aimed to identify and evaluate behaviour change techniques and functions in lifestyle interventions for preventing the progression of CKD.
Design Systematic review.
Data sources MEDLINE, EMBASE, CINAHL and PsycINFO.
Eligibility criteria Trials of lifestyle behaviour change interventions (including diet, physical activity, smoking and/or alcohol) published to September 2018 in adults with CKD stages 1–5.
Data extraction and synthesis Trial characteristics including population, sample size, study setting, intervention, comparator, outcomes and study duration, were extracted. Study quality was independently assessed by two reviewers using the Cochrane risk of bias tool. The Behaviour Change Technique Taxonomy v1 was used to identify behaviour change techniques (eg, goal setting) and the Health Behaviour Change Wheel was used to identify intervention functions (eg, education). Both were independently assessed by three reviewers.
Results In total, 26 studies involving 4263 participants were included. Risk of bias was high or unclear in most studies. Interventions involved diet (11), physical activity (8) or general lifestyle (7). Education was the most frequently used function (21 interventions), followed by enablement (18), training (12), persuasion (4), environmental restructuring (4), modelling (2) and incentivisation (2). The most common behaviour change techniques were behavioural instruction (23 interventions), social support (16), behavioural demonstration (13), feedback on behaviour (12) and behavioural practice/rehearsal (12). Eighteen studies (69%) showed a significant improvement in at least one primary outcome, all of which included education, persuasion, modelling and incentivisation.
Conclusion Lifestyle behaviour change interventions for CKD patients frequently used education, goal setting, feedback, monitoring and social support. The most promising interventions included education and used a variety of intervention functions (persuasion, modelling and incentivisation).
PROSPERO registration number CRD42019106053.
- chronic kidney disease (CKD)
- lifestyle
- diet
- exercise
- behaviour change techniques
- health behaviour change wheel
- Behaviour Change Technique Taxonomy v1
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- chronic kidney disease (CKD)
- lifestyle
- diet
- exercise
- behaviour change techniques
- health behaviour change wheel
- Behaviour Change Technique Taxonomy v1
- systematic review
Strengths and limitations of this study
We used comprehensive, evidence-based frameworks to identify and describe behaviour change techniques and intervention functions in lifestyle behavioural interventions for patients with chronic kidney disease.
Coding of behaviour change techniques and intervention functions was systematically and independently conducted by three researchers, and risk of bias was assessed.
Summary estimates could not be ascertained due to the heterogeneity of interventions and outcome measures.
Introduction
Preventing the progression of chronic kidney disease (CKD) is a high priority for patients and clinicians, to reduce the requirement for dialysis.1–3 Lifestyle interventions which modify behavioural risk factors such as poor diet and low physical activity can prevent progression of CKD and life-threatening complications and improve quality of life and survival.4–6 Addressing behaviour change is particularly relevant in CKD as lifestyle modification can be challenging. Poor adherence to diet, medication and other treatments is common in CKD.7 Barriers to modifying lifestyle include low health literacy, conflicts with cultural norms, complicated nutritional requirements and safety concerns.7–11
Guidelines recommend the explicit use of behaviour change for addressing lifestyle risk factors when designing and reporting interventions for patients with CKD.12 13 However, it is uncertain which aspects of lifestyle behaviour change interventions are the most effective, and reporting of behavioural components is often unclear, making implementation in practice problematic.
The Behaviour Change Technique Taxonomy v1 was developed to provide a comprehensive framework that integrates behaviour change techniques used in interventions.14 The Taxonomy was further synthesised into a framework, the Health Behaviour Change Wheel which describes the intervention functions necessary to change health behaviours.15 The Health Behaviour Change Wheel provides a broad, overarching framework in which to characterise behaviour change interventions while the Taxonomy identifies specific techniques related to individual behaviours. The intervention functions described in the Health Behaviour Change Wheel can be delivered by a variety of behaviour change techniques. For example, the intervention function, ‘education’, outlined in the Wheel, can include the behaviour change techniques ‘instruction on how to perform the behaviour’ and ‘information about antecedents’, detailed in the Taxonomy. Similarly, the intervention function ‘incentivisation’ can incorporate techniques such as ‘feedback on behaviour’ and ‘rewards’.
Behaviour change interventions using the Wheel and the Taxonomy can effectively change lifestyle behaviours. For example, a text-messaging and pedometer programme improved physical activity in people at high risk of type 2 diabetes,16 a digital healthy eating programme increased consumption of fruit and vegetables and sustained this over a 6-month period17 and a digital behaviour change programme achieved significant weight loss results in individuals at risk of type 2 diabetes.18 The Taxonomy and the Wheel are recommended approaches to modify lifestyle risk factors for chronic disease prevention.12 16 18 However, these frameworks have not been used in designing and reporting behaviour change strategies in lifestyle interventions for patients with CKD.
We aimed to identify and evaluate behaviour change techniques and intervention functions used in lifestyle interventions for preventing the progression of CKD. This may inform the development of effective and replicable behaviour change interventions for the prevention of CKD, leading to improvements in patient outcomes.
Methods
We used the Preferred Reporting Items for Systematic Reviews and Meta-analyses Statement19 and checklist to report this systematic review (online supplementary file S1).
Supplemental material
Selection criteria
We included randomised trials of lifestyle behaviour change interventions (including, but not restricted to diet, physical activity, smoking and alcohol consumption) in adult patients (aged over 18 years) with CKD stages 1–5 and not requiring renal replacement therapy. We did not apply restrictions based on outcomes or language. Studies including a combination of pharmacological therapy and lifestyle were included but trials involving only pharmacological therapies were excluded.
Literature search
A comprehensive search was conducted in MEDLINE (1946 to 20 September 2018), EMBASE (1996 to 20 September 2018), CINAHL (1982 to 20 September 2018) and PsycINFO (1806 to 20 September 2018) using Medical Subject Heading (MeSH) terms relating to CKD, and lifestyle behaviour change interventions (online supplementary file S2), and reference lists of relevant articles and reviews. Author NE screened the studies by title and abstract and assessed full-text articles for eligibility. Those that did not meet the inclusion criteria were excluded.
Supplemental material
Data extraction and critical appraisal
The trial characteristics relevant to the population, sample size and study setting as well as intervention (type, mode of delivery, use of theory, intervention functions (as described in the Health Behaviour Change Wheel15 and behaviour change techniques (as described in the Behaviour Change Technique Taxonomy v114)), comparator, outcomes and study duration, were extracted and tabulated. We assessed the risk of bias using the Cochrane tool for randomised studies.20 NE and KM assessed the risk of bias in each study independently and any differences were resolved by discussion.
We contacted the authors of the studies when it was necessary to gather additional information. Supplemental data was available in 12 of the 26 studies. In six studies with no supplemental data, sufficient information was available in the published article. Therefore, we contacted eight authors to request further information and received responses from two authors.
Analysis of intervention functions and behaviour change techniques
The Behaviour Change Technique Taxonomy v1 (the ‘Taxonomy’) and Health Behaviour Change Wheel (the ‘Wheel’) are comprehensive tools for identifying behavioural components in interventions and how frequently they occur.14 15 The two frameworks are complementary and in addition to designing interventions, they have been used as a method for identifying behavioural components in public health interventions and clinical trials.21 The tools have been used in previous systematic reviews to identify behaviour change techniques and functions in health interventions.22–28
Behaviour change techniques
The Behaviour Change Technique Taxonomy consists of 93 behaviour change techniques, such as goal-setting, self-monitoring, social support and re-structuring the physical environment (see online supplementary table S1 for the full taxonomy). The techniques are grouped into 16 domains: goals and planning, feedback and monitoring, social support, shaping knowledge, natural consequences, comparison of behaviour, associations, repetition and substitution, comparison of outcomes, reward and threat, regulation, antecedents, identity, scheduled consequences, self-belief and covert learning.
Supplemental material
Intervention functions
There are nine intervention functions in the Wheel: education, persuasion, incentivisation, coercion, training, enablement, modelling, environmental restructuring and restrictions.15 These are activities designed to change behaviours and include one or more behaviour change techniques. Definitions of each intervention function have been described by Michie et al and were used to inform decisions about what functions were present in each study.15
Authors NE and KM completed online training for interpreting the Wheel and the Taxonomy to ensure consistency and reliability of coding.29 N.E, KM and VS independently read intervention descriptions line-by-line to locate text matching a definition of an intervention function15 and the description of behaviour change techniques from the BCTTv1 coding frame (online supplementary table S1). Each of the 93 behaviour change techniques were indicated as either present or absent in a standardised data extraction form. A behaviour change technique had to be explicitly described to be coded and included in the analysis. The authors compared the codes and discussed discrepancies to reach consensus.
Patient and public involvement
No patient involved.
Results
Literature search and study characteristics
The literature search yielded 10 043 citations from which 26 studies (n=4263 participants) were eligible and included in the review (figure 1). Study characteristics are shown in table 1. The studies were conducted in 15 countries.
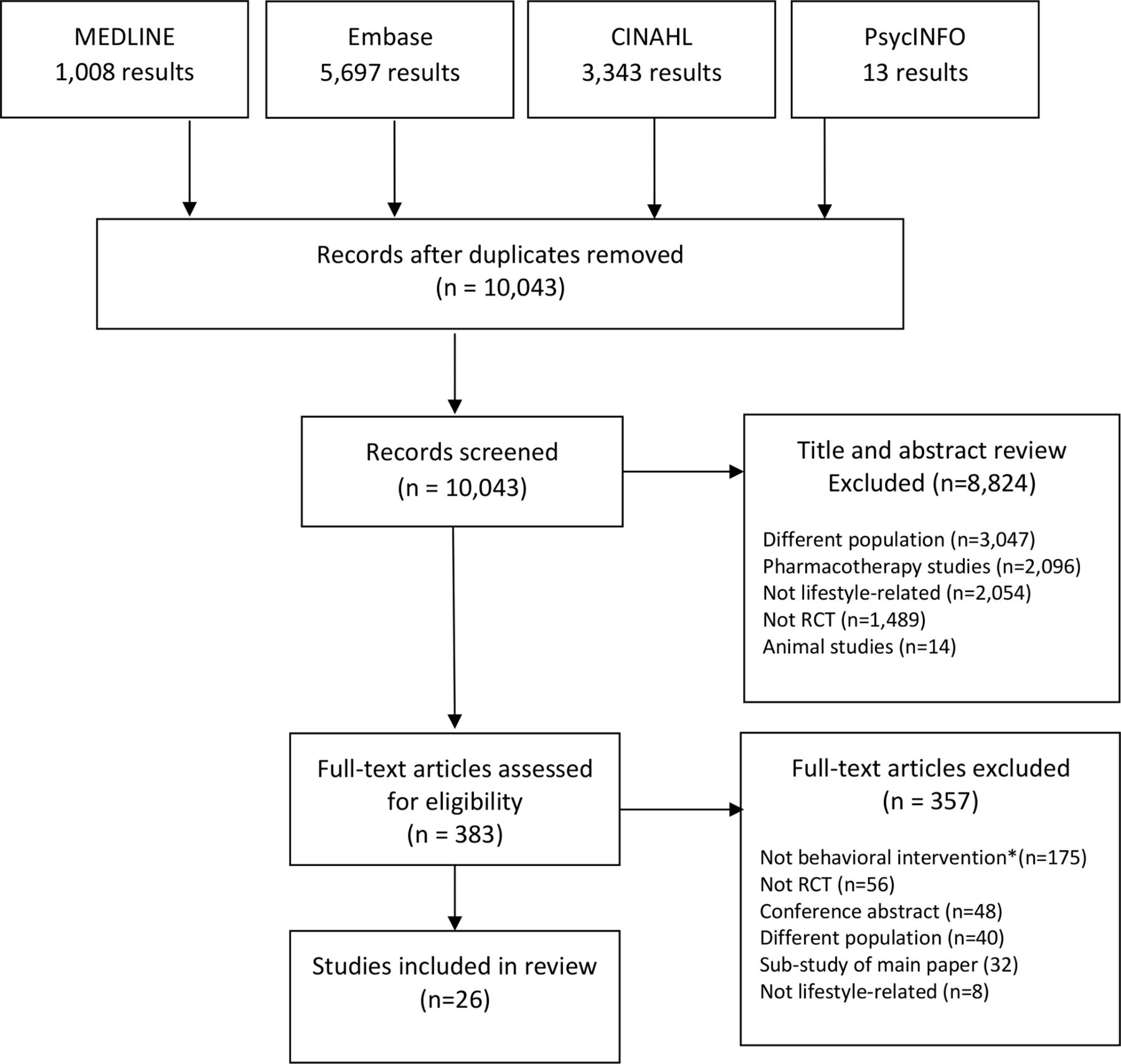
PRISMA flowchart of included/excluded studies. *A behavioural intervention explicitly describes a behaviour change technique which can be coded using the Behavior Change Technique Taxonomy v1. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Characteristics of included studies
Risk of bias assessment
Overall, the reporting of studies was relatively incomplete, particularly for the blinding of participants and personnel which was missing or unclear in every study (figure 2). Allocation concealment was unclear or at high risk of bias in 20 (77%) studies. Blinding of outcome assessment was also poorly reported with 19 studies showing high or unclear risk of bias for this domain. Domains that performed better were selective reporting with low risk of bias in 21 studies, random sequence generation with low risk of bias in 17 studies and incomplete outcome data showing low risk of bias in 13 studies.

{kind=link}
{kind=link}
Risk of bias for individual studies (n=26). MDRD, Modification of Diet in Renal Disease study.
Characteristics of the interventions
Across the interventions assessed in the 26 studies included, 11 were dietary interventions, 8 involved physical activity and 7 used any combination of diet, physical activity, weight reduction and/or smoking cessation (lifestyle).
Five studies were informed by theory, three used the Trans-Theoretical Model,30 31 one used self-regulation theory32 and another was informed by contemporary behavioural theory, in particular the self-management approach.33 Two studies used Motivational Interviewing,34 35 a counselling approach which involves behaviour change strategies.36
Only three studies included family members, friends or partners in the intervention to facilitate participant’s behaviour change (online supplementary table S2).31 37
Supplemental material
Behaviour change techniques
Table 2 outlines the number of behaviour change techniques present in each lifestyle behaviour change intervention. The number of behaviour change techniques used across interventions ranged from two to 20.
Cross matrix of behaviour change techniques and lifestyle behaviour change trials
The top five most frequently observed behaviour change techniques were instruction on how to perform the behaviour (23 interventions, 88%), social support (16, 62%), demonstration of the behaviour (13, 50%), feedback on behaviour (12, 46%) and behavioural practice/rehearsal (12, 46%). Of the 93 possible behaviour change techniques that could have been used, 12 techniques were used in more than 20% of trials, 27 were used at least once and 54 were never used. The mean number of behaviour change techniques was 5, the median was four and the range 2–20.
The two studies with the highest number of behaviour change techniques (20 and 18 in each study) were both informed by theory, with a particular focus on self-regulation and self-management.32 33
Intervention functions
Table 3 lists the intervention functions present in each study (education, enablement, training, persuasion, modelling, incentivisation, environmental restructuring, coercion and restrictions). The number of functions used across interventions ranged from one to seven.
Education
Education was used most frequently as an intervention function, present in 21 (81%) interventions (table 3). Examples of educational strategies were: nutritional label reading,38 39 a resistance training booklet for home-based exercise,40 a lecture/workshop about exercise recommendations with demonstrations,30 online education modules on lifestyle modification41 and a written ‘six-tip diet’ checklist.42
Cross matrix of intervention functions and lifestyle behaviour change trials
Enablement
Eighteen (69%) interventions used enablement. Examples include Motivational Interviewing to improve self-management of diet, lifestyle and physical activity,32 43 supportive telephone calls matching stages of behaviour change,30 self-management techniques to foster self-efficacy38 39 44 and arranging support from friends and family members and ‘buddy’ visits.31 33 Four interventions were specifically designed using a self-management approach and assessed self-efficacy as an outcome.32 33 39 44
Training
Twelve (46%) interventions included training as an intervention function. Training was used in every intervention targeting physical activity but only used in two dietary interventions and two lifestyle interventions. Examples of training include home-based exercise training, guided exercise training in a gym,40 physical therapy or cardiac rehabilitation facility45 or hospital34 and interactive cooking classes.39
Persuasion
Four (15%) interventions used persuasion as an intervention function. A dietary intervention aimed to persuade participants about dietary salt intake by displaying test tubes of salt content alongside a range of high-salt food items.46 In another dietary intervention, positive thinking was applied to participant’s goals and dieticians praised progress and focused on positive results.33 Similarly, a lifestyle intervention used positive reinforcement to increase confidence and celebrate successes related to behaviour change and also discussed lack of exercise, poor dietary habits, risks of not exercising and associated consequences.31 Only one physical activity intervention used persuasion in designing and displaying printed health messages to promote exercise.30
Environmental re-structuring
Four (15%) interventions used environmental restructuring. Two involved placing exercise equipment in the home environment (exercise bicycle, Theraband, weights and Swiss ball)40 43 and two included adding food products and equipment into the home environment (low sodium/protein meals and water bottles).33 47
Modelling
Two (8%) dietary interventions incorporated modelling as an intervention function. Educators used food models and household measuring utensils to model appropriate food portion sizes46 and food tastings provided an example of low protein meals.33
Incentivisation
Two (8%) studies used incentivisation, one in the form of ‘appreciation gifts’ including certificates and mugs33 and another included ‘self-rewards’ chosen by participants.32
Coercion and restrictions
These functions were not used in any of the interventions.
Outcomes
A description of primary outcomes and results reported in studies is included in table 4. Primary outcomes of studies in this review were diverse and were mainly physiological metrics (for example, eGFR, blood pressure, peak VO2 and sodium or albumin excretion). Only six studies included patient-reported and/or behavioural primary outcomes such as quality of life, fatigue, knowledge, self-efficacy, self-management, exercise and health behaviours.30 31 44 45 48 49
Effects of the behaviour change interventions on the primary outcome(s)
Eighteen studies (69%) showed a significant improvement in at least one primary outcome and all of these studies included education, persuasion, modelling and incentivisation as an intervention function (see online supplementary table S3). A meta-analysis of the data was not possible due to heterogeneity of outcome measures across the included studies. The heterogeneity of outcomes also meant we could not link outcomes with specific behaviour change techniques. Many studies are likely to be underpowered to detect modest effects, and so the absence of a statistically significant effect should not be regarded as evidence of no effect.
Supplemental material
Discussion
Behaviour change interventions in trials in patients with CKD mostly focused on diet and physical activity. The primary outcomes of the trials were diverse and most were biochemical outcomes (eg, eGFR, blood pressure, peak VO2 and sodium or albumin excretion), with few clinical or patient-reported and/or behavioural outcomes such as quality of life, fatigue, knowledge, self-efficacy and self-management.30 31 38 39 44 45 Only five interventions were underpinned by theory. The most frequently used intervention function was education, followed by enablement and training. Persuasion, environmental restructuring, modelling and incentivisation were used less frequently. Coercion and restrictions (which includes regulation) were not used in any of the studies. The top five most common behaviour change techniques were instruction on how to perform the behaviour, social support, demonstration of the behaviour, feedback on behaviour and behavioural practice/rehearsal. Identity, scheduled consequences and covert learning were not used in any of the studies. No association between frequency of functions or behaviour change techniques and the effect of interventions on outcomes could be identified.
The use of multiple behaviour change techniques does not necessarily lead to better outcomes and some evidence suggests that fewer techniques and the right combinations of techniques suited to the context are more effective.50–52 Education was the most frequent intervention function used across the studies, which may be because it has been consistently shown that patients with CKD lack awareness about lifestyle risk factors and have low health literacy.10 11 53 Specifically, the behaviour change technique, ‘instruction on how to perform the behaviour’, was the most frequently reported technique, used in all interventions except two. We suggest this is highly applicable because dietary interventions can involve complex dietary restrictions of sodium, protein, potassium and phosphate. Patients have sought practical advice about how to implement these restrictions.54 However, most educational strategies used a didactic approach, with health professionals verbally conveying information or providing written materials. Patients with CKD prefer multiple problem-solving and collaborative approaches, in partnership with health professionals.54 Also, written materials for patients with CKD have a reading grade of 9 (age 14–15 years), which is higher than the recommended level (grade 5).10
The intervention function ‘training’ was used in every study targeting physical activity but was only used in two dietary interventions. Patients with CKD are overwhelmed by dietary information which can be complex, restrictive and insensitive to cultural norms.54 A recent review of educational interventions for CKD patients found that including practical skills and workshops was associated with better outcomes.55 For example, a low-salt programme for Bangladeshi patients with CKD in the United Kingdom included cooking and educational sessions facilitated by Bengali workers in a community kitchen. It targeted both patients and family members who cooked their own low-salt version of Bangladeshi recipes and led to a reduction in salt intake and reduced blood pressure for participants.37 Approaches to enabling and training patients for behaviour change incorporating hands-on training may be more effective.
Our findings are similar to recent reviews of behavioural interventions for other conditions (cardiovascular disease, obesity, rheumatoid arthritis, prostate cancer and diabetes), which also found that behavioural interventions are not well-reported, not informed by theory and have diverse outcomes and modes of delivery.25–27 51 56 The behaviour change techniques associated with goals and planning, feedback and monitoring and social support have also been frequently used in behaviour changes interventions in patients with other chronic conditions. These techniques are proven strategies for behaviour change and in line with evidence-based recommendations for lifestyle modification.12 13 57
We identified and described the behaviour change techniques and intervention functions in lifestyle behavioural interventions for patients with CKD with comprehensive evidence-based frameworks. Coding of behaviour change techniques and intervention functions was systematically and independently conducted by three researchers, and risk of bias was assessed. Potential limitations relate to poor reporting. Some interventions may have used behaviour change techniques or intervention functions in their study but did not report them, or details of techniques were unclear. We contacted authors and examined all associated supplementary materials and papers to collect more information.
Lifestyle behaviour change interventions for patients with CKD appear to integrate recommended and proven behaviour change techniques and intervention functions. These techniques such as goals and planning and self-monitoring are important but focus on individual agency rather than external factors. Interventions could be improved by considering the context of behaviour change and the social and physical environment of participants. For example, most of the interventions for physical activity focused on structured exercise programme and a reliance on equipment (eg, exercise bikes). Patients with CKD need to be able to integrate physical activity in to their daily lifestyle.58 However, only one intervention for physical activity gave instructions on how to incorporate physical activity to fit in with daily activities and in environments easily accessible to patients, without the use of equipment.59 This study reported improvements in cardiopulmonary and functional capacities of overweight patients with CKD.
Optimising the social environment and arranging support from friends, family and the community may also improve lifestyle behaviour change interventions for patients with CKD. Family support was used rarely in interventions in this review and only included in two studies.31 37 However, informal caregivers play an important role in the management of CKD and are often required to change their own lifestyle behaviours to support patients with CKD.60 Characteristics of effective educational interventions for patients with CKD involved the patient’s family.55
The quality of the design and reporting of lifestyle behaviour change interventions for patients with CKD requires explicit description of behavioural strategies to ensure interventions are generalisable and replicable. There are numerous evidence-based guidelines that recommend the explicit use of behaviour change techniques for addressing lifestyle risk factors in chronic disease prevention and these may be better used when designing and reporting interventions for patients with CKD. Recently the National Institute of Health and Care Excellence in the UK published comprehensive guidelines specific to behavioural interventions and lifestyle modification.12 The WHO’s recommendations on behaviour change support this and further reinforce the need to consider the social and environmental determinants of health in changing lifestyle behaviours.57
Conclusion
Lifestyle interventions in trials conducted in patients with CKD mostly focus on goals and planning, feedback and monitoring and education. However, we suggest that interventions may be improved by using interactive and tailored training, and strategies to help patients incorporate lifestyle modification in their daily activities, and physical and social environments. Explicit application of behaviour change taxonomies may help to increase the effect of lifestyle behaviour change interventions for improved health outcomes in patients with CKD.
References
Footnotes
Contributors Research idea and study design: NE, AT, JC; data acquisition: NE, KM, VS; data analysis/interpretation: NE, AT, JC, AB, KM, VS; statistical analysis: NE; supervision or mentorship: AT, JC, AB.
Funding This work was supported by a Postgraduate Research Scholarship and a National Health and Medical Research Grant (NHMRC: 1098815).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.