Article Text

Abstract
Objectives Whether spinal anaesthesia (SA) reduces intraoperative and postoperative complications compared with general anaesthesia (GA) was investigated.
Design The meta-analysis was structured based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement. Databases (PubMed, MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials and Web of Science) were searched, and four randomised controlled trials (RCTs) and two retrospective cohort studies were included. A random-effects model with pooled risk ratios and mean differences with 95% CIs were used. Statistical heterogeneity was evaluated using the I2 statistic. Quality assessment of the studies was performed by assessing the risk of bias according to the Cochrane and GRADE methodology.
Setting Publications from January 1990 to November 2018 were included.
Participants and interventions Our study selection captured information from studies focusing on neonates born before the 37th gestational week who were scheduled for an inguinal hernia repair operation under either SA or GA.
Primary and secondary outcome measures The primary outcome measures were apnoea, postoperative ventilation and method failure rates according to predefined eligibility criteria. The duration of surgery, desaturation events <80%, hospital stay duration and postoperative bradycardia were secondary outcomes.
Results We found significantly fewer events for the outcomes ‘any episode of apnoea’ and ‘mechanical ventilation postoperatively’ in the SA group. Bradycardias were significantly less common in the SA group. In total, 7.5% of the SA group were converted to GA. The duration of surgery was significantly shorter in the SA group. No significant differences were found in the outcome measures ‘postoperative oxygen supplementation’, ‘prolonged apnoea’, ‘postoperative oxygen desaturation <80%’ and ‘hospital stay’.
Conclusions We consider SA a convenient alternative for hernia repair in preterm infants, providing more safety regarding postoperative apnoea. To the best of our knowledge, this is the first meta-analysis to include studies exclusively comparing SA versus GA. More high-quality RCTs are needed.
Trial registration number CRD42016048683
- apnoea
- general anaesthesia
- herniorrhaphy
- neonates
- spinal anaesthesia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This systematic review and meta-analysis was based on a rigorous search of the literature with maximum efficiency by combining an initial focused search with a subsequent follow-up search.
All specified outcome parameters were audited independently by two persons.
Our synthesis approach used a mixture of description and tabulation to summarise the evidence, including the strength of evidence and risk of bias.
So far, unpublished post hoc data were analysed and resulting findings are provided to ensure best evidence.
All included studies varied and were not homogeneous concerning the spinal anaesthesia and general anaesthesia techniques and the published haemodynamic and outcome measures.
Introduction
Spinal anaesthesia (SA) is a fast, simple and cost-effective method that has been used for the performance of inguinal hernias since the beginning of the 20th century.1 As it has become more established in recent years, the relevant technical skills and knowledge have matured. Thus, it is of great interest to investigate this specific local technique and compare it to the commonly used general anaesthesia (GA), which has also been under consideration in recent years due to possible damaging side effects.2–5 In neonates, GA is associated with a high risk of complications, such as bradycardia and apnoea,6 whereas SA may involve far fewer side effects. Nevertheless, GA remains the preferred choice.7 Over the last few decades, improved neonatal care has led to a significant increase in the survival of neonates delivered preterm.8 9 Prematurity is the largest risk factor for inguinal hernias, which need to be repaired at an early age.10–12 Moreover, preterm-born neonates are more likely to have pre-existing diseases such as bronchopulmonary dysplasia, which puts them at an even higher risk for developing complications. In addition, gestational age and apnoea are inversely proportionally related. Due to the increasing obligation to intervene via herniorrhaphy, investigating whether any of the common anaesthetic procedures offer advantages in this context is of paramount interest.10 Our aim was to assess which anaesthetic technique could provide better patient safety outcomes.
In this meta-analysis, we systematically analysed the current literature on SA versus GA for inguinal hernia repair in neonates born before the 37th gestational week. We looked at the incidence of apnoea, the need for postoperative ventilation, the incidence of failure of SA and more outcome parameters.
Methods
This meta-analysis and systematic review was based on the guidelines of the ‘Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols’ (PRISMA-P) statement.13
Information sources and search strategy
The PubMed, MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials and Web of Science databases were screened for relevant publications in all languages up to November 2018. The search terms were “Hernia, Inguinal/surgery” AND “(Infant OR preterm infant)” AND “(Anaesthesia, General OR Anaesthesia, Spinal)” (online supplementary figure 1). The search terms were constructed conforming to the PICOS framework to achieve the best search result (online supplementary figure 2). Additionally, the reference lists of eligible studies were screened. All databases were independently screened by KD and GS, and the results were compared.
Supplemental material
Supplemental material
Study selection and eligibility criteria
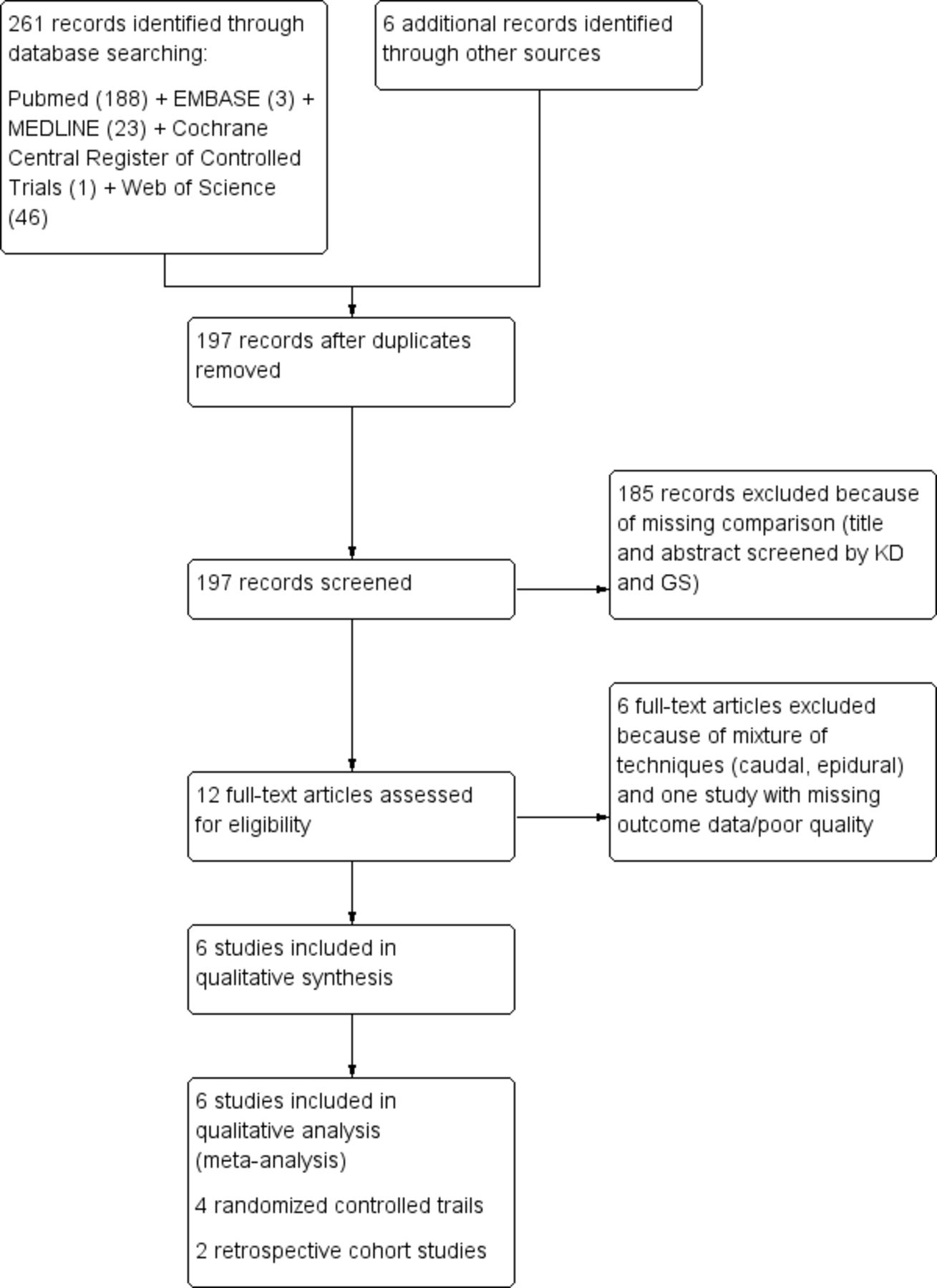
Our study selection captured information from studies focusing on neonates born before the 37th gestational week who were scheduled for an inguinal hernia repair operation under either SA or GA. Due to the small number of randomised controlled trials (RCTs), retrospective cohort studies (RCSs) were also included. The primary outcome measures were apnoea, postoperative ventilation and method failure rates according to predefined eligibility criteria. Duplicate sources were excluded. Irrelevant sources were eliminated based on their abstracts and titles. The full texts of the remaining articles were analysed and re-evaluated. A flow diagram based on the PRISMA statement depicting the study selection process was constructed (figure 1).
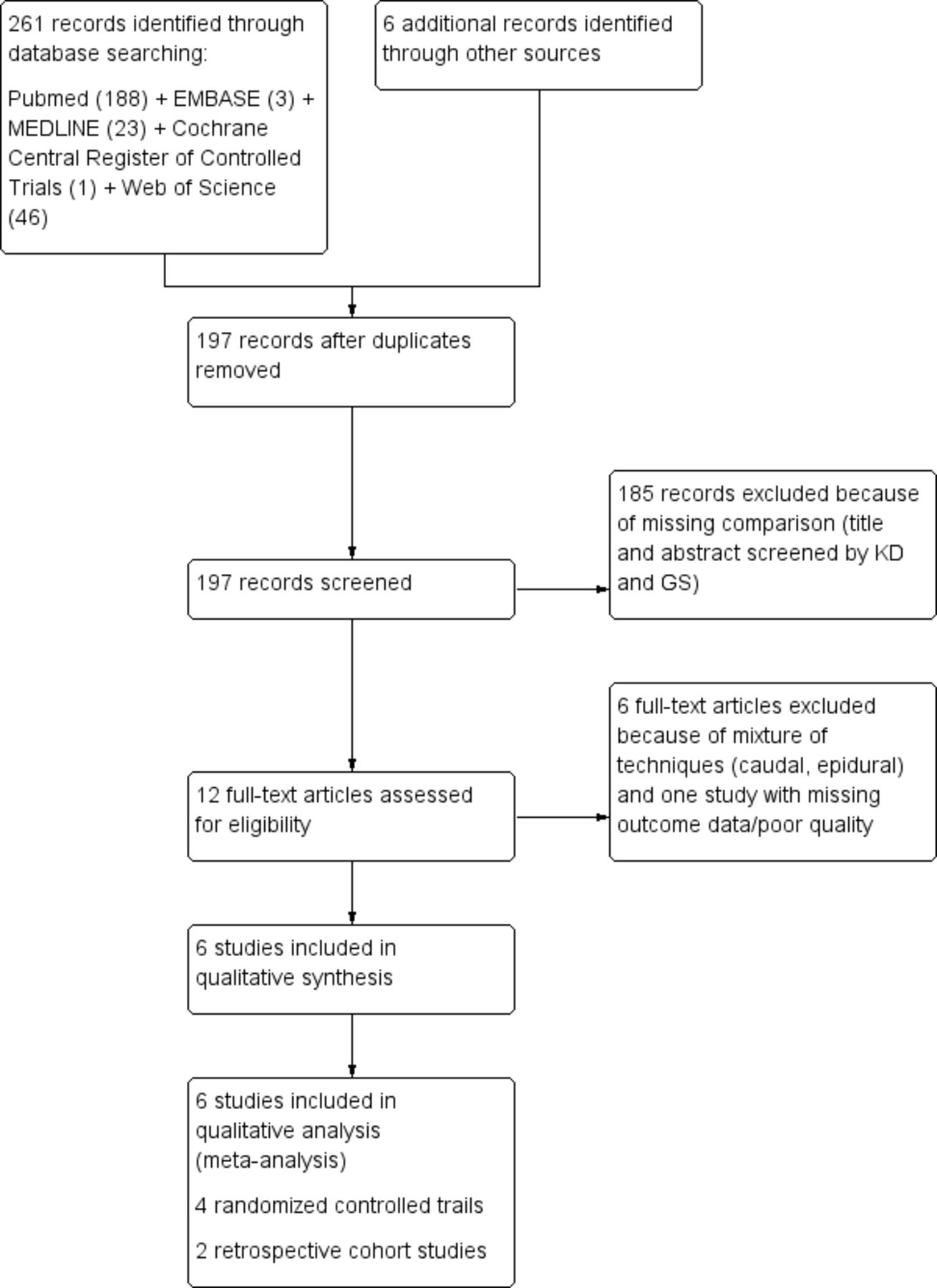
Flow diagram of the meta-analysis based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement.
Some studies compared a mixed dataset of regional anaesthesia (ilioinguinal, caudal, etc) to GA.14–18 To gather information on the subgroups and include it in our analysis, we contacted the authors. Therefore, we were able to apply our inclusion criteria and to include the subgroup data from the GAS trial.17
Patient and public involvement
Due to the methodology of this trial, neither the patients nor the public were directly involved in the research question, selection of the outcome measures, design and implementation of the study or the interpretation of the results.
Data collection process and data items
After the final sources were defined, the baseline characteristics were compiled in a database showing the name of the study, year of publication, first author, study design, number of patients, sex of the patients, postconceptional age, body weights, type of anaesthesia and anaesthetics used, pre-existing lung conditions, whether supplementary oxygen was required before surgery and whether supplemental medication was administered, for example, pain medication.
The following outcomes were collected independently by KD and GS: episodes of postoperative apnoea, need for postoperative mechanical ventilation and incidence of failure of SA as primary outcomes and the duration of surgery, desaturation events <80%, hospital stay duration and postoperative bradycardia as secondary outcomes.
The hospital stay duration was calculated based on the raw data in Somri et al.19 Pre-existing lung condition formed a supergroup for respiratory distress syndrome and a history of preoperative apnoea. Focusing on the GAS trial, we grouped all patients who ever received an endotracheal tube, methylxanthine or continuous positive airway pressure preoperatively.
Risk of bias
Review Manager (RevMan) software (Cochrane Collaboration, London, UK) was used to perform the risk of bias analysis in individual studies in the following domains: selection bias, performance bias, detection bias, attrition bias and reporting bias.20 Each study was analysed individually for these biases by KD and GS.
Publication bias is usually evaluated by a funnel plot or by further analysis, such as Egger’s and Begg’s tests. Funnel plots require a minimum of 10 studies for safe interpretation. Another option for evaluating publication bias is to analyse small-study effects. Small studies are often associated with more decisive treatment effects caused by publication bias.21 To focus on these potential effects, we looked for evidence concerning selective reporting and the selection criteria for patient populations. Selective reporting was evaluated by missing outcome data and the emphasis of non-significant outcomes.
GRADE methodology (GRADEpro, Version 20; McMaster University, 2014) was used to assess the quality of evidence across studies.22 23
Statistical analysis
RevMan version 5.3 was used to perform the statistical analyses of the selected data (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).20 The Department of Medical Statistics of the RWTH Aachen University, Aachen, Germany, supervised the methodology of the statistical analysis.
Descriptive measures, such as rates (means, SD) and their corresponding 95% CIs, were calculated using MedCalc Statistical Software for Windows, version 16.8 (MedCalc Software, Ostend, Belgium). The outcome effects were either continuous or dichotomous and are depicted in forest plots. Effect measure estimates were calculated as the mean differences (MDs) for all continuous variables and as risk ratios (RRs) for dichotomous variables with 95% CIs in a random effects model.24 25 For the MDs, we applied the inverse variance method.
Across studies, heterogeneity was determined to detect whether the results of both groups were comparable. To quantify heterogeneity, we used the I2 statistic following the Higgins and Thompson method.26 27 Heterogeneity was noted as substantial if I2 was >50% and was mentioned in our results. When heterogeneity was detected, a sensitivity analysis was performed to identify possible reasons. We considered p-values <0.05 as statistically significant. The null hypothesis was tested as a two-sided hypothesis that there was no difference in the outcome between GA and SA.
Single-zero studies were calculated assuming that 0.5 events occurred in the group.28 To investigate whether double-zero studies, which were excluded in the analysis in RevMan, and the method of including single-zero studies via continuity corrections changed our results, we used the beta-binominal regression method in SAS (V.9.4; SAS Institute, Cary, North Carolina, USA) Macro (MA_DOUBLEZERO)29 to reanalyse the data, and all differences are described in the following sections.
Results
The database search yielded 261 studies, with 6 additional studies found in the reference lists (figure 1). After removing duplicates, 197 studies were screened by title and abstract, after which 10 articles remained. After applying the eligibility criteria, six studies (four RCTs and 2 RCSs) were ultimately identified. A total of 512 patients were included (226 patients with SA and 286 with GA).
Baseline characteristics
Table 1 shows the baseline characteristics of all included studies.
Baseline data of the included studies
Risk of bias and GRADE
Our risk of bias analysis provides an indication of publication bias. All studies except Kim et al 30 and Lambertz et al 31 assigned the patients randomly to the groups, but the process of random sequence generation was described in only one study.17 The participants were easily blinded because the surgery was performed on infants born preterm, but procedural blinding was not possible due to the anaesthetists’ interventions. Somri et al 19 excluded three patients due to puncture failure and one patient due to hypothermia in the SA group. In one trial, patients were allocated to the GA group after unsuccessful puncture, and episodes of postoperative apnoea were reported in only the GA group.32 Online supplementary figure 3 shows our risk of bias graph.
Supplemental material
Very low quality evidence was detected for any episode of apnoea, and low quality evidence was detected for prolonged apnoea. Moderate quality of evidence was found for postoperative mechanical ventilation and bradycardias. The overall evidence quality was reduced because sequence generation was not described, and the sample sizes were small. Online supplementary table 1 shows the GRADE analysis table.
Supplemental material
Primary outcomes
Complete failure of the method
Complete failure of the method was defined as a change from SA to GA at any point during surgery. In total, 7.5% (95% CI: 0.04 to 0.12) of the patients undergoing SA (15 of 200 patients) were converted to GA (online supplementary table 2). In total, 28% (95% CI: 0.21 to 0.37) received more than one puncture (54 of 191 patients)17 19 33 and 16% (95% CI: 0.10 to 0.25) required supplemental anaesthesia (11 of 29 patients).17 19 31 Davidson et al 17 reported one case of high spinal block that required manual ventilation.
Supplemental material
Postoperative apnoea
The outcomes were grouped into (1) any episode of apnoea and (2) prolonged apnoea. Somri et al 19 and Welborn et al 33 defined short apnoea as a breathing pause for less than 15 s. Prolonged apnoea was defined as a breathing pause for longer than 15 s or shorter than 15 s if associated with bradycardia.17 19 30 Krane et al 32 defined apnoea as a pause lasting from 11 to 15 s.
The analysis (figure 2A) showed that SA was significantly better than GA (RR 0.45 (95% CI: 0.25 to 0.79); p=0.006) for any episode of apnoea. In the SA group, 9% (95% CI: 0.05 to 0.16) of the patients (13 of 142 total patients) suffered from apnoea, whereas 20% (95% CI: 0.15 to 0.27) of the patients in the GA group experienced any episode of apnoea (49 of 241 total patients).

Postoperative apnoea: (A) any episode of apnoea, (B) prolonged apnoea, (C) postoperative oxygen supplementation, and (D) postoperative mechanical ventilation.
The item prolonged apnoea (figure 2B) did not reach a significant difference for any of the methods (RR 0.36 (95% CI: 0.12 to 1.10); p=0.07). It occurred in 4.5% (95% CI: 0.02 to 0.10) of the SA group (6 of 133 patients) and in 11.6% (95% CI: 0.10 to 0.20) of the GA group (27 of 232 patients).
Postoperative respiratory support
Respiratory support after surgery was subdivided into the need for oxygen supplementation and the need for mechanical ventilation in any form (nasal airway, Guedel tubus, endotracheal intubation, etc).
Patients requiring postoperative oxygen supplementation (figure 2C) were more common in the GA group, but this difference did not reach significance (RR 0.71 (95% CI: 0.40 to 1.27); p=0.25). In total, 13.5% (95% CI: 0.08 to 0.22) of the patients (17 of 126) in the SA group and 16.4% (95% CI: 0.12 to 0.23) of the patients (36 of 219) in the GA group required oxygen postoperatively.
Postoperative mechanical ventilation (figure 2D) was more frequent in the GA group (RR 0.16 (95% CI: 0.04 to 0.63); p=0.009). In total, 1.9% (95% CI: 0.004 to 0.06) of the patients in the SA group (3 of 157 patients) and 13% (95% CI: 0.04 to 0.18) of the patients (34 of 255) in the GA group needed mechanical ventilation after the operation.
Secondary outcomes
Desaturation <80%
Only Krane et al 32 defined a time period of at least 10 s and recorded the events for 12 hours. Davidson et al 17 continuously recorded desaturation in the first postoperative hour and noted it every 5 min.
With regard to obtaining a desaturation of <80% (events per patient), there was no significant advantage or disadvantage (RR 0.56 (95% CI: 0.30 to 1.03); p=0.06) of one method. However, 6% (95% CI: 0.03 to 0.13) of SA patients (7 of 111 patients) and 10% (95% CI: 0.06 to 0.15) of GA patients (20 of 205 patients) underwent desaturation <80%.
Hospital stay
The mean value and SD of the hospital stay were calculated from the raw data in Somri et al.19 The hospital stay was shorter in the SA group,19 32 but this difference was not significant (MD −0.42 (95% CI: −1.27 to 0.43); p=0.33). Heterogeneity was considerable (I2=77%, p=0.01). Online supplementary figure 4 shows the results of the analysis.
Supplemental material
Bradycardia
Most of the studies defined bradycardia as fewer than 100 beats per minute,17 19 30 32 although Krane et al 32 defined bradycardia as fewer than 80 beats per minute. Davidson et al 17 recorded heart rates continuously for the first postoperative hour, and heart rates were noted in a 5 min rhythm. Bradycardia appeared more frequently in the GA group (figure 3), with an occurrence of 5.8% (95% CI: 0.03 to 0.10, 15 of 255 patients), and a significant difference was found between groups (RR 0.44 (95% CI 0.20 to 0.99); p=0.05). In the SA group, 3.1% of the patients (95% CI: 0.01 to 0.07, 5 of 157 patients) had bradycardias.

{kind=link}
{kind=link}
{kind=link}
Postoperative bradycardia.
Duration of surgery
The duration (online supplementary figure 5) was significantly shorter for surgeries performed under SA (MD −2.53 (95% CI: −4.93 to −0.12); p=0.04). Heterogeneity was detectable but under the level of significance (I2=19%).
Supplemental material
Additional analysis
Sensitivity analysis, single-zero and double-zero studies
Significant heterogeneity was detected for hospital stay duration (I2=77%). The sensitivity analysis of the hospital stay revealed that lower heterogeneity occurred (I2=42%) when Lambertz et al 31 was removed for this measure; however, excluding that study did not alter the fact that no significant difference between SA and GA was observed. The definition of hospital stay was not consistent, which was probably the main reason for the marked heterogeneity.
The outcome measures, including single-zero studies (any episode of apnoea and prolonged apnoea), were reanalysed using the SAS Macro as described, but the results equalled our primary results for both outcome measures. The double-zero outcome measures were also reanalysed using beta-binominal regression analysis in SAS. For the outcome measures, including double-zero studies (postoperative mechanical ventilation and bradycardia), the results changed such that by including the double-zero studies, no significant difference between SA and GA could be found (RR 0.17 (95% CI: 0.02 to 1.58), p=0.12; RR 0.41 (95% CI: 0.08 to 2.01), p=0.27).
Discussion
The objective of this meta-analysis was to compile all data from trials comparing SA and GA for inguinal hernia repair and to assess whether SA or GA provided superior patient safety outcomes. The findings revealed significant benefits in terms of the outcome measures for SA in the postoperative time frame for any episode of apnoea, the need for mechanical ventilation, bradycardia and the duration of surgery. We did not find any differences between the groups for the postoperative outcomes of desaturation <80%, the need for oxygen supplementation, prolonged apnoea and hospital stay duration.
In our analysis, some important data could not be captured by a single endpoint outcome, for example, prolonged apnoea. In Davidson et al 17 in the SA group, prolonged apnoea was self-resolved or resolved through stimulation in 60% of patients, and 40% of prolonged apnoea was resolved through oxygen supplementation with or without mask ventilation. In the GA group, 17% of the patients who had prolonged apnoea experienced resolution of the apnoea by itself or through stimulation, whereas 83% of the patients received oxygen supplementation with or without mask ventilation. One of the patients in the GA group even underwent cardiopulmonary resuscitation. Our outcome of postoperative mechanical ventilation also showed a significant difference between the two groups. For apnoea, there were different endpoints of observation. Between 12 hours and 5 days postoperatively, 2.9% of patients (3 of 102 patients) in the SA group and 3% (6 of 196) in the GA group underwent interventions for apnoea.17 No patients were intubated in this time frame, whereas in the GA group, one patient had to remain intubated. Many studies have emphasised the difficulty of monitoring apnoea events. Cote et al 34 noted that apnoea was recorded at a higher prevalence when the recording device was equipped with an alarm bell, which was used in only one trial. Das et al 35 observed that proper therapy for postoperative pain reduces instances of apnoea, and patients in the SA group required less pain medication than patients in the GA group.
There was a difference in the prehistory of apnoea between the two groups. Somri et al 19 reported that 3% of the patients, one patient in the SA group and three patients in the GA group, had a prior history of apnoea. Welborn et al 33 identified no patients with a prior history of apnoea in the SA group and 60% in the GA group. Davidson et al 17 reported that all patients had a prehistory of apnoea in the SA group, whereas only 79% of the patients had a history of apnoea in the GA group. This parameter can likely never be controlled, but because lung condition is very important to the risk of developing a postoperative apnoea,36 37 it might also influence the effect estimates. In addition, gestational age and apnoea are inversely proportionally related.38
In some studies,31 32 patients received some sort of sedation in the SA group. While it is never possible to exclude the need for a sedative, as the aim should always be to provide the best care for the individual, the use of sedation might have restricted the effects of SA. Additionally, many of the anaesthetics used in our comparison studies are no longer state-of-the-art anaesthetics. Using older studies in our review might be an indication of inconsistency when considering the GRADE methodology tools. Nevertheless, we believe that, for this subpoint, it is still important to investigate possible side effects, as many of these anaesthetics are still used in Europe as well as in developing countries for cost-efficiency reasons.39
Each of the methods is linked to a certain special risk. For SA, it is possible to cause a high spinal block, as was noted in one patient (0.7%). GA always has a risk due to volatile or intravenous anaesthetics, ventilation and the longer duration of surgery. In addition, 7.5% of patients undergoing SA had to be converted to GA. Comparing our findings to others, we observed variation in the failure rate, ranging from 3%40 to 15%.17 Lambertz et al 31 emphasised the anaesthesiologist’s experience as essential to ensure the maximum success rate. Overall, regarding these experiences performing spinal blocks for inguinal hernia repair, we conclude that SA is a safe method. Due to a lack of experience, it is associated with a lower success rate than GA, but it provides advantages by being technically simple and fast and limiting risks that require postoperative intervention.
Neurotoxicity was not discussed in any of the comparison studies. Patients were usually followed up until they left the hospital. Davidson et al 17 found no difference in neurodevelopment at the age of two between a sevoflurane group (of less than 1 hour exposure) and a group of patients who underwent regional anaesthesia. However, there is a major need for an investigation of the long-term effects.
The outcome parameters of postoperative ventilation and bradycardia changed to non-significant when we added the double-zero studies into our analysis. As double-zero studies do not add information to the decision regarding which treatment should be preferred, Cochrane recommends excluding these studies.41 The relative risk estimates remained approximately the same. By including the double-zero studies, the differences between SA and GA could not be classified as significantly different as the CIs became very wide. We therefore recommend not overinterpreting the results of the analysis that included the double-zero studies.
To the best of our knowledge, no meta-analysis has considered trials focused only on comparing SA to GA for inguinal hernia repair in preterm-born neonates. When we looked at other large randomised studies that also compared SA to GA for other operations in infants, it was discovered that hypotension was more frequent in the GA group and that SA patients had shorter operation durations and hospital stays.16 42 43 The regional anaesthesia methods (spinal, caudal and epidural) used were mixed in one large meta-analysis, which included studies of infants born preterm undergoing hernia repair and compared them with a GA group.44 A strength of our review is that we excluded all studies with any other type of regional method to compare the possible advantages of the two methods. Additionally, we included the selected data from the largest study by Davidson et al.17 For future investigations, we suggest a well-designed and adequately powered study with neonates born preterm who are still preterm while undergoing hernia repair, as most of the infants in our meta-analysis were not premature at the point of hernia fixation.
Conclusions
Our results suggest that SA is at least as safe as GA for inguinal hernia repair because it had an overall small failure rate and reduced the risk for any postoperative apnoea, bradycardias and the need for mechanical ventilation. Therefore, SA is a convenient alternative for hernia repair in infants born preterm. However, more RCTs with larger numbers of patients are needed to increase the quality of evidence.
Acknowledgments
Assistance with the study: We thank the GAS Consortium for the support with their data and the friendly exchange of information. We also thank Dr Risto Rintala, Dr Emily Harville and Dr Isabel Elaine Allen for their efforts and contributions in reviewing our meta-analysis.
References
Footnotes
Contributors GS and KD conceived of the study design of the review. GS and KD performed the literature search and eligibility assessment. KD performed the data extraction. GS and KD individually assessed the study quality and data analysis. TB reviewed the manuscript in terms of statistical methods analysis and structure. Clinical input and assistance with the discussion was given by GS, RR, CBE, MC, MH and CS. KD wrote the manuscript. All authors reviewed the manuscript and approved it.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.