Article Text

Abstract
Introduction The creatine kinase circuit is central to the regulation of high-energy phosphate metabolism and the maintenance of cellular energy turnover. This circuit is fuelled by creatine, an amino acid derivative that can be obtained from a diet containing animal products, and by synthesis in the body de novo. A recent retrospective study conducted in a cohort of 287 pregnant women determined that maternal excreted levels of creatine may be associated with fetal growth. This prospective study aims to overcome some of the limitations associated with the previous study and thoroughly characterise creatine homeostasis throughout gestation in a low-risk pregnant population.
Methods and analysis This study is recruiting women with a singleton low-risk pregnancy who are attending Monash Health, in Melbourne, Australia. Maternal blood and urine samples, along with dietary surveys, are collected at five time points during pregnancy and then at delivery. Cord blood and placenta (including membranes and cord) are collected at birth. A biobank of tissue samples for future research is being established. Primary outcome measures will include creatine, creatine kinase and associated metabolites in antenatal bloods and urine, cord bloods and placenta, along with molecular analysis of the creatine transporter (SLC6A8) and synthesising enzymes L - arginine:glycine amidinotransferase (AGAT) and guanidinoacetate methyltransferase (GAMT) in placental tissues. Secondary outcome measures include dietary protein intake over pregnancy and any associations with maternal creatine, pregnancy events and birth outcomes.
Ethics and dissemination Ethical approval was granted in August 2015 from Monash Health (Ref: 14140B) and Monash University (Ref: 7785). Study outcomes will be disseminated at international conferences and published in peer-reviewed scientific journals.
Trial registration number ACTRN12618001558213; Pre-results.
- creatine kinase circuit
- placenta
- nutrition
- fetal growth restriction
- fetal hypoxia
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This observational study will provide comprehensive information about maternal adaptations to creatine homeostasis during pregnancy, with each participant providing repeated biological samples across gestation and at birth (total of six time points per participant).
The recruiting sites will provide a study population with diverse ethnic, socioeconomic and dietary backgrounds to ensure our findings are broadly applicable.
The establishment of biobank and databank (<2000 individual biological samples) will facilitate further research in the low-risk pregnancy setting.
As this is a study of low-risk pregnant women, it is unlikely to be powered to identify associations between maternal creatine levels and poor pregnancy outcomes; results will be primarily descriptive.
Introduction
Cells with high energy turnover use the creatine kinase circuit to buffer fluctuations in ATP supply and demand.1 Creatine is critical for this pathway, and can be obtained from a diet containing fish, meat or dairy, as well as produced by the body endogenously, via a two-step enzymatic reaction (de novo synthesis).2–4 Creatine synthesis involves the enzyme L - arginine:glycine amidinotransferase (AGAT) converting the amino acids arginine and glycine to the creatine precursor guanidinoacetate (GAA). Methionine then donates a methyl group to GAA to produce creatine, in a secondary reaction catalysed by guanidinoacetate methyltransferase (GAMT). Creatine is taken up by cells via the specific creatine transporter SLC6A8.5
Dietary creatine supplementation has been studied extensively in non-pregnant humans, primarily as an ergogenic aid to elite athlete training, due to its enhanced ability to supply energy to cells with high energy demand.6–10 Despite the increased metabolic load of pregnancy,11 12 and pregnancy-induced hormonal effects on many amino acids and protein availability, little is known about the role of creatine in supporting energy homeostasis in the mother and the developing baby.12–15
Studies conducted in preclinical animal models provide evidence to suggest that creatine is a critical cellular energy metabolite for pregnancy, and that maternal dietary creatine supplementation during gestation reduces perinatal mortality and severe multiorgan morbidity after hypoxic insults.14 16–20 Our previous retrospective collaborative study in a pregnant human cohort showed maternal creatine levels appear to be related to fetal growth, with increased creatine concentrations in the mother’s urine being associated with increased birthweight centile and length of her baby.21 Heazell et al also demonstrated in a matched case–control study that creatine levels were reduced by 20% in the serum from women who had an adverse pregnancy outcome (composite of stillbirth, preterm birth, small for gestational age or perinatal asphyxia).22 These data support the theory that there is a creatine requirement during pregnancy. Most recently, a seminal study describing the expression of the creatine synthesising enzymes AGAT and GAMT, and the production of creatine by human placental tissue in vitro, suggests that the placenta may contribute to meeting maternal and fetal creatine requirements during pregnancy.23 Taken together, preclinical and observational clinical studies indicate that creatine may be an essential metabolite during pregnancy and that adequate levels of creatine during pregnancy may be critical for optimal fetal growth and survival.
The prospective study outlined in this protocol will characterise creatine homeostasis in a low-risk pregnant population across gestation and at birth. The overall aim of this study is to further our understanding of the creatine kinase circuit in pregnancy. Specific considerations will include whether dietary preferences impact maternal creatine concentrations, the role of the placenta in creatine production and whether maternal creatine concentrations are associated with pregnancy outcomes.
Objectives
Determine maternal concentrations of creatine, creatine kinase, arginine, glycine and methionine in blood and urine samples over five time points throughout pregnancy and then at birth.
Determine placental and cord blood concentrations of creatine, creatine kinase, arginine, glycine and methionine, along with molecular analysis of the creatine content, synthesis and transport in placental tissues at birth.
Determine if maternal dietary intake of animal protein affects creatine concentrations across pregnancy.
Determine whether there is any association between creatine concentrations across pregnancy and at birth with maternal characteristics in pregnancy and neonatal outcomes, specifically fetal birth weight and length.
Methods and analysis
Study design
This is a prospective observational cohort study in pregnant women, developed in reference to the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for cohort studies24 and the Global Pregnancy CoLlaboration site guidelines.25
Patient and public involvement
Participants were not asked or offered the opportunity to participate in the study design. The researchers did consider the study requirements in relation to pregnancy care and scheduled all appointments to coincide women’s visits to antenatal clinics.
Setting
This study includes pregnant women attending low-risk antenatal clinics and planning to birth at Monash Health, Melbourne, Victoria.
Participants/Recruitment
Women aged 18–40 years who have a singleton low-risk pregnancy are invited to participate. Women who have a known significant pre-existing major medical condition or who have been assessed as high risk are excluded (table 1). As pregnancy is a dynamic state, women can develop conditions or subsequent diagnoses as pregnancy progresses. Women who have a significant change in their health status or the status of their pregnancy, or who require transfer of care to a high-risk clinic, are subsequently excluded (box 1).
Comparison of inclusion and exclusion criteria
Subsequent exclusion criteria
Major congenital fetal abnormality.
Change of birth venue/model of care, during pregnancy.
Disclosure of ongoing substance use/alcohol or drug dependency.
Exacerbation of previously stable medical condition now requiring active intervention and transfer to a high-risk pregnancy clinic.
Development of significant new medical/pregnancy condition requiring active intervention and transfer to high-risk pregnancy clinic.
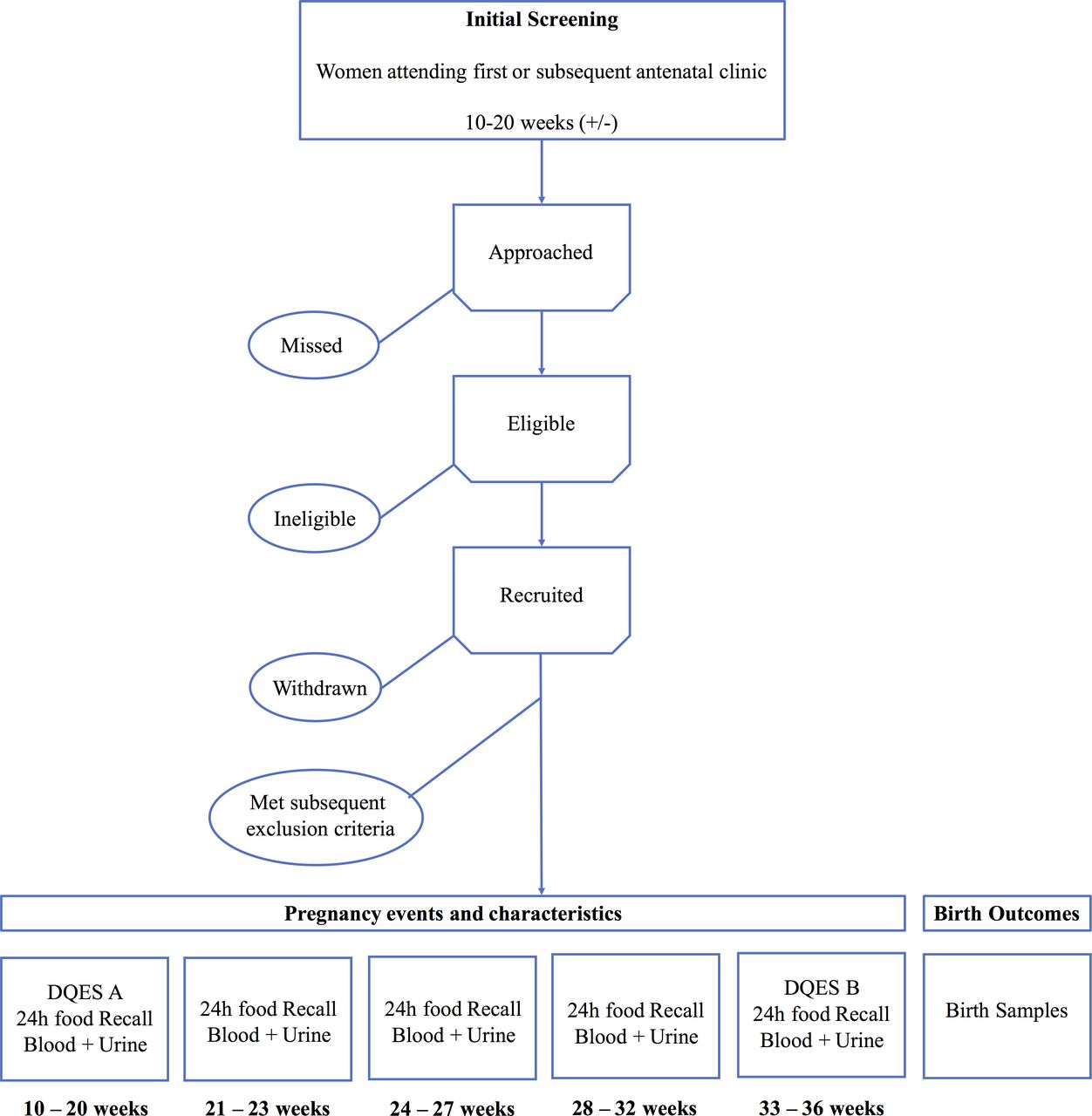
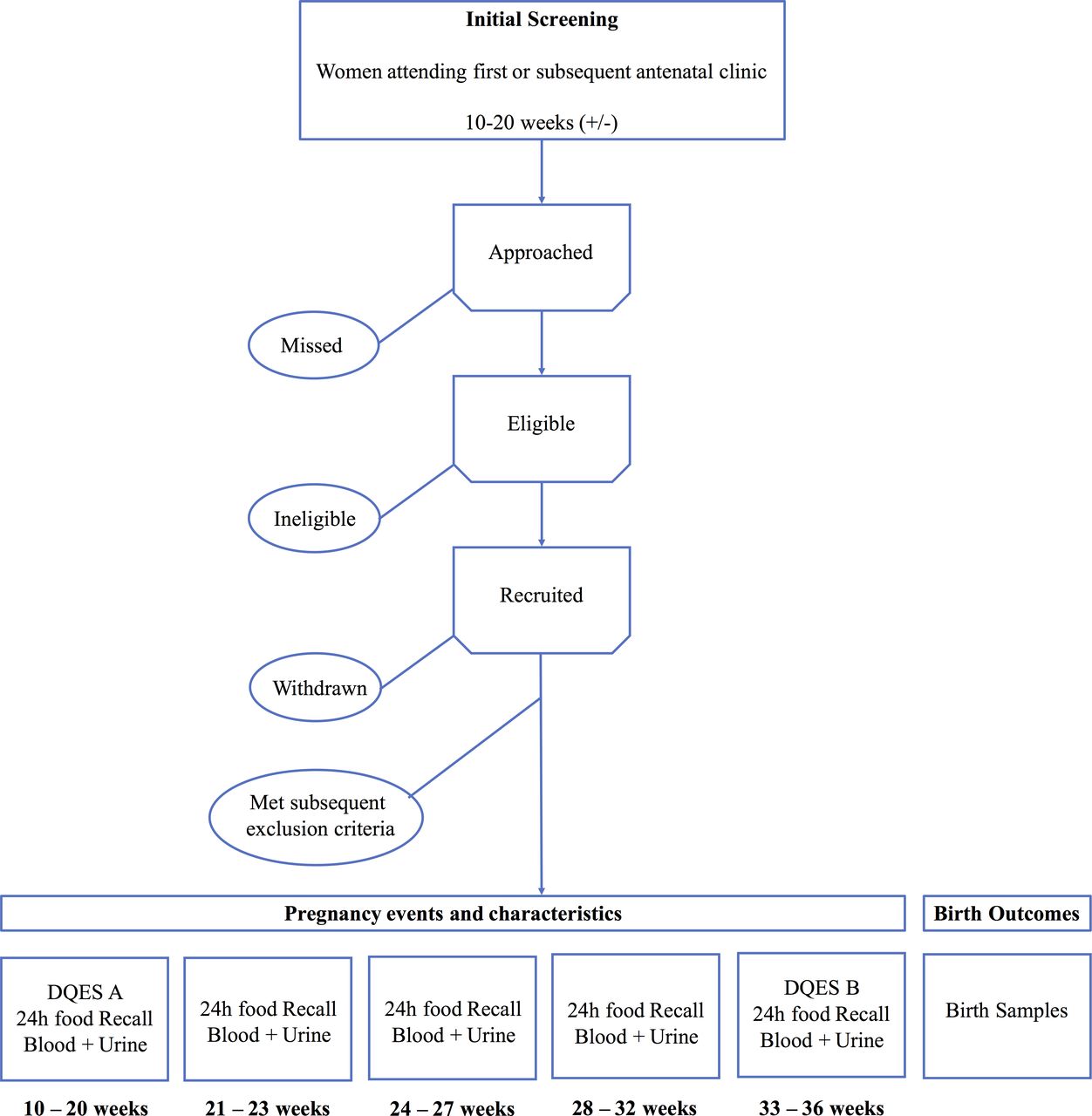
Women are approached by the researcher and the study aims and requirements discussed in detail. If women express an interest, a patient information and consent form is provided. Women either choose to consent at the first or subsequent visit to the antenatal clinic (between 10 and 20 weeks). After providing informed consent, blood and urine samples and 24-hour food recalls are collected at five antenatal visits between 10 and 20 weeks (time of consent), 21–23 weeks, 24–27 weeks, 28–32 and 33–36 weeks, and then at birth (figure 1). At the first and the last antenatal visit, women complete an online food frequency survey, Dietary Questionnaire for Epidemiological Studies (DQES V.2). Women receive a birth kit at the 24–28 week antenatal visit and are reminded to bring this to the hospital on the day of delivery. The kit contains collection apparatus and detailed instructions for staff on sample collection and storage. Consenting women may choose to biobank their samples for future perinatal research studies approved by Monash Health.
{kind=link}
Schematic overview of study recruitment and sampling regimen. Pregnancy events and characteristics include sociodemographic parameters, relevant medical history, body mass index, blood pressure and gestational weight. Birth outcomes include labour and delivery outcomes, type of onset of labour, labour stage time points, drug use, colour of liquor, mode of delivery and blood loss, and neonatal parameters including gestational age, gender, Apgar scores, weight, height, head circumference and length of hospital stay. DQES, Dietary Questionnaire for Epidemiological Studies; weeks, number of weeks’ gestation.
Primary outcome measures
Concentrations of creatine, creatine kinase, arginine, glycine and methionine are measured in maternal plasma and urine at five time points during gestation, in cord vein and arterial plasma, and placental tissue at birth. Placental mRNA and protein expression of the creatine transporter (SLC6A8), AGAT, GAMT and creatine kinases will also be analysed, along with placental enzymatic activity of AGAT and GAMT, to determine placental creatine synthesis and storage.23
Secondary outcome measures
Macronutrient and micronutrient dietary intake of women will be analysed in FoodWorks V.8 (Xyris Software) to determine if variations in dietary intake are associated with creatine concentration.
Frequency and portion sizes of major food groups (before and during pregnancy) will be measured using the food frequency survey, DQES V.2. Frequency and portion sizes of major food groups will be determined from the raw data and analysed by the Cancer Council Victoria’s purpose-made software program. A report on each participant will be provided. Responses will be converted to daily equivalent frequencies (DEF).26 The DEF and portion sizes (multiplied by the portion size factor) will be used to calculate the average daily intake of the foods listed in the FFQ; this is then combined with data from The Nutrient Data Table for Use in Australia (NUTTAB95) to calculate nutrient intake.27
Sociodemographic data, pregnancy events and birth outcomes data are also collected. Sociodemographic parameters include maternal age, country of birth, ethnicity and education level. Relevant medical history will capture any pre-existing clinical variables such as hypothyroidism or other correctable nutritional deficiencies. Pregnancy parameters include body mass index (BMI) at booking, blood pressure readings and gestational weight gain (GWG) over pregnancy. Significant antenatal events include diagnosis of gestational diabetes mellitus, hospitalisations, enhanced maternal monitoring due to blood pressure changes or enhanced fetal monitoring due to suspected fetal growth restriction. Labour and delivery outcomes will be captured and will include type of onset of labour, labour stage time points, drug use during labour and colour of liquor, mode of delivery, and blood loss. Neonatal parameters include gestation at birth, gender, Apgar scores, weight, height and head circumference, and length of hospital stay.
Sample collection and processing
Antenatal sample collection
Blood is collected into lithium heparin tubes for collection of plasma and kept on ice until processing (note: creatine is stable in whole blood, kept on ice, for up to 8 hours). Whole blood (4×250 μL aliquots) is taken before subsequent centrifugation for isolation of plasma (400 g, 20 min, 4°C). Plasma aliquots (10×250 µL) are then stored at −80°C. Urine is collected and kept on ice until processing (within 8 hours). The sample is transferred to a 50 mL Falcon tube and centrifuged (400 g, 20 min, 4°C), before being aliquoted (10×500 µL) and stored at −80°C. Date and times are recorded for sample collection, sample processing start and completion, and subsequent freezer storage.
Placental processing
The placenta is trimmed of membranes and cord (1 cm long cord segment placed in optimal cutting temperature (OCT) compound and frozen, membrane rolled and fixed in buffered formalin) before obtaining placental weight. For molecular and biochemical analyses, 4× ~2 cm2 pieces of placenta from four healthy cotyledons (one in each quadrant of the placenta) are sampled. These full thickness pieces are washed in four sequential saline washes to remove excess blood. One square is dissected into two pieces, one fixed in buffered formalin and the other placed in OCT and frozen. Remaining squares are dissected into 0.2 cm2 pieces, pooled (8×5 piece aliquots) and stored at −80°C for future molecular analysis.
Sample analysis
Amino acids and metabolites will be measured using triple quadrupole mass spectrometer coupled to liquid chromatography, to determine the concentrations of creatine, GAA, phosphocreatine, arginine, glycine and methionine in maternal blood and urine throughout pregnancy and in cord blood at birth.28–31 Creatine kinase will be measured in maternal blood and urine throughout pregnancy and in cord blood and placenta at birth using a commercially available creatine kinase activity assay. RNA and protein will be extracted from placental tissue using standard laboratory techniques. Real-time quantitative PCR and western blot analysis will be used to assess expression patterns of the creatine transporter (SLC6A8), the creatine synthesising enzymes (AGAT and GAMT) and creatine kinases (mitochondrial and cytosolic).
Potential sources of bias
Selection bias and loss to follow-up
We are recording the total number of women who are approached and are potentially eligible for the study. The number of participants subsequently excluded or withdrawn is recorded. Potential selection or sample bias, along with loss to follow-up, will be reported in subsequent publications. Loss to follow-up is minimised with timing of research sampling coinciding with standard clinical care. Women routinely receive a reminder message prior to their next appointment.
Unpredictable nature of birth
To enhance birth sample collection, women are provided with a birth kit and reminded at subsequent appointments to bring this on presentation to hospital. A computerised alert is placed in their electronic health record. A study sticker is attached to the hand-held maternity record to alert staff to study participation. Monash Health midwives are involved in the birth sample collection. Feedback and reporting of study milestones and achievements occur routinely to enhance staff commitment and engagement.
Maternal diet determination
While the DQES and 24-hour food recall surveys are both validated tools to determine macronutrient and micronutrient intake, all currently available diet assessment tools are prone to bias and are not well validated in pregnant populations.32–34 To minimise recall bias within the 24-hour food recall surveys, these are conducted over five time points and cross-referenced with the researcher at each time point to enhance participant recall. Multipass food interview techniques are also employed to enhance recall and validity of data assessment and enhance correct classification of macronutrients in pregnancy.
Misclassification of maternal factors/confounder
GWG in pregnancy is often poorly captured during routine antenatal visits. We record women’s weight at each research time point over pregnancy, on the same industrial scales in the antenatal clinic. While prepregnancy weight is self-reported, we determine the first BMI at the earliest visit using digital scales and height measures. Country of birth may not always reflect ethnicity, so to minimise this bias we establish both country of birth and ethnicity.
Sample blinding
Samples are de-identified at the time of collection and given a sequential identification number. Scientists analysing the biological samples are blinded to the maternal demographics, pregnancy and birth outcomes.
Data handling
De-identified data are collected, entered and stored in our custom secure database by the study coordinator. Sample processing forms are entered via a Google Drive secure network and linked to de-identified data via a unique identifier.
Sample size and statistical analysis
This study will be the first prospective study of creatine and associated metabolites across pregnancy and at birth in a normal healthy pregnant population. It overcomes the limitations with regard to generalisability and bias in the diet measurements in our previously published study. Findings from this study will inform future studies of effect sizes and associations. Objectives 1 and 2 are descriptive only. With regard to objectives 3 and 4, to our knowledge there is no software that allows sample size determination for multilevel mixed models regression. As such, no formal power calculations have been undertaken. Despite the limitations of our previous study, we were sufficiently powered to determine associations between plasma and urine creatine and birth weight. We have therefore determined a sample size of 300 for this prospective cohort study.
All data will be assessed for normality. Appropriate descriptive statistics of the study sample will be tabulated. The association between maternal age group (<20 years, 20–30 years and 30 plus), BMI (<19, 19–24.9, 25–29.9 and ≥30), maternal ethnicity, diet, GWG, and urine and plasma creatine over pregnancy will be determined using linear mixed models. Maternal concentrations of creatine, creatine kinase, arginine, glycine and methionine in blood and urine samples will be summarised and graphically presented over the five time points. The correlation between circulating and excreted creatine, amino acids and metabolites, at each of the gestation points, will also be determined.
As this is the first prospective human work on the creatine kinase circuit at birth in both cord blood and the placenta, we will also determine the Interclass/interclass correlation coefficient (ICC) and agreement between placental and cord creatine concentrations at birth. Placental and cord blood concentrations of creatine, creatine kinase, arginine, glycine and methionine, along with molecular analysis of the creatine transporter (SLC6A8) and synthesising enzymes AGAT and GAMT in placental tissues, will be graphically determined at birth. The association between potential confounders such as dietary intake, blood pressure, BMI, physical activity level and GWG across each time point in pregnancy and maternal creatine (plasma and urine) over pregnancy will be assessed. Multivariate linear mixed models will be used to determine the associations between creatine concentrations (and associated factors), maternal diet over pregnancy as well as with growth outcomes, adjusting for potential confounders.
Ethics and dissemination
The increased blood sampling and 5-hour abstinence from meat/fish were the primary ethical considerations in our study. These were addressed prior to ethics approval. Study outcomes will be disseminated at international conferences and published in peer-reviewed scientific journals. Lay reports will be made available to study participants on request.
Discussion
This is a prospective cohort study in low-risk pregnant women to measure creatine homeostasis over pregnancy and at birth. This study will enhance our understanding of the potential impact maternal factors, including diet and ethnicity, may have on maternal creatine homeostasis. These studies will also enhance our understanding of the role the placenta plays in creatine homeostasis during pregnancy. It is beyond the scope of this study to capture all pregnancy populations. As this is a study of low-risk pregnant women, it is unlikely to be powered to identify associations between maternal creatine levels and poor pregnancy outcomes. Results will be primarily descriptive; however, data collected in this population may be used to compare with higher risk pregnancy populations in the future. Overall, this research will help establish the framework on which to build future studies of maternal dietary creatine supplementation during gestation to improve pregnancy outcomes. In addition, the development of a new biobank of antenatal samples will also provide a valuable asset for future research endeavours in this field.
Acknowledgments
We wish to thank the scientific support staff including Rod Snow, Greg Kowalski and David Walker and the clinical support staff Euan Wallace and Kirsten Palmer for their expertise in their fields. We are grateful to Joanne Mockler for assistance with preparing the HREC for this project and to Ann Doran for commencing the recruitment process. Thanks to Annike Griffey, Kathryn Shearer, Natasha Juckhov and Tuzana Nawar for assistance with consenting and recruiting. Thanks to Nadia Bellofiore, Jared Mamrot, Lara Rijkmans, David Roberts, Cody Thomas, Alex Crough and Tuzana Nawar for their assistance with sample processing.
References
Footnotes
Patient consent for publication Not required.
Contributors HD conceived the study design. MD-T performed power and sample size calculations. HD and SE developed and executed protocols for sample collection and processing. DdG drafted the manuscript and leads study recruitment and coordination.
Funding Funding to initiate this study was provided by the Stillbirth Foundation of Australia. Additional funds for the use and analysis of the dietary questionnaires are provided by the Andrea Joy Logan Trust. During this period, HD was supported by an NHMRC Career Development Fellowship and a Cerebral Palsy Alliance Career Development Grant. SE and MD-T both held NHMRC Early Career Research Fellowships. No funding body had a role in the study design, data collection, analysis and interpretation, or writing of this manuscript.
Competing interests None declared.
Ethics approval This study was approved, as described in the text (with subsequent minor amendments), in August 2015 by Monash Health Human Research Ethics (approval number 14140B) and Monash University (approval number 7785).
Provenance and peer review Not commissioned; externally peer reviewed.