Article Text

Abstract
Introduction There seems to be little information on interactional patterns of enabling and constraining factors contributing to HIV care engagement across systems and across time. Understanding these patterns from a (micro–meso–macro–exo) systems perspective can provide rich insights on relevant social networks affecting transgender populations. In this review, we will synthesise the wealth of literature on transgender persons’ engagement in the HIV care continuum.
Methods and analysis We will perform a networked systems approach to qualitative evidence synthesis of relevant qualitative research data generated from primary qualitative, mixed-method and evaluation studies exploring HIV care engagement among diverse transgender populations. Studies not using qualitative methods and studies not published in English will be excluded from this review. Empirical studies will be identified via a search in major databases such as PubMed, Scopus, ERIC, Embase, Web of Science, Sociological Abstracts, PsychInfo and Social Services Abstract in January 2019. Two reviewers will independently screen the studies for inclusion, assess their quality and extract data. In case some of the system levels in the network are ill-covered by empirical studies, non-empirical studies will be considered for inclusion. The qualitative evidence synthesis includes a summary of descriptive data (first order), an exploration of relationships between system levels or their components (second order) and a structured summary of research evidence through narrative synthesis. The narrative synthesis will be extended with an overall social network analysis that visualises important nodes and links cutting across ecological systems.
Ethics and dissemination Ethical approval is not required to conduct this review. Review findings will be disseminated via peer-reviewed academic journals and a targeted information campaign towards organisations that work with our population of interest.
PROSPERO registration number CRD42018089956.
- qualitative research
- public health
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
We will use a theory informed networked systems approach to systematically synthesise qualitative evidence.
Findings will provide nuanced information on the challenges faced by specific transgender populations.
Strategies to include relevant quantitative evidence in the networked system approach need to be explored and considered for future updates.
The advancement of health technologies and services addressing the HIV epidemic (eg, introducing antiretroviral therapy (ART)) in the global and local scale made HIV/AIDS a chronic and manageable health condition. However, HIV health disparities still exist among various vulnerable groups, such as men who have sex with men (MSM) or transgender persons, in light of the HIV care continuum (eg, awareness of HIV status, availing early HIV care, retention in care, adherence to ART and viral suppression). Findings from a meta-analysis by Baral and colleagues1 have shown a 19% worldwide HIV prevalence and a 49-fold increased odds of HIV infection among transgender women compared with non-transgender population. Moreover, the distribution of HIV prevalence vary across transgender subpopulations and geographical regions across the globe. For example, transfeminine people of colour in the USA and some ethnic minorities in Europe, as well as transfeminine sex workers in Latin America, were identified to be highly vulnerable to HIV.2 Indeed, public health interventions may need to be more sensitive in responding to differential health outcomes rooted in wider societal and cultural systems of stigma and oppression.3 4
The purpose of this review project is to systematically synthesise the wealth of literature on transgender persons’ engagement in the HIV care continuum (ie, unaware of HIV infection, aware of HIV infection (not in care), receiving/psychological care but not HIV care, entered HIV care but not lost to follow-up, cyclical or intermittent user of HIV care and fully engaged to HIV care) using a systems perspective. Existing literature on transgender HIV healthcare emphasised the institutional, provider and patient level barriers to effective and sustainable engagement.5 6 Across these levels of engagement (ie, from personal to structural levels), stigma related to minority stress is systematically reproduced and felt by transgender persons.7 8 Although there has been improvement in crafting evidence-based HIV interventions specific to transgender populations, structural determinants such as budget constraints or weak funding patterns that cater to healthcare needs and services targeting these groups is still a problem.9 As such, evaluating studies on HIV care engagement among transgender people can benefit from a systems perspective because it can provide important insights on how causal structures change over time, as well as the ‘identification of leverage points, anticipation of unintended consequences and unexpected results, and comprehensive assessment of stakeholder views’10 (p. 258).
To synthesise findings across levels of the HIV care continuum, we will adapt a networked analytical approach to evidence synthesis based on Bronfrenbrenner’s Ecological Systems Theory.11 12 Recent work of Neal and Neal12 redefined an ecological environment or setting as ‘an overlapping arrangement of structures, each directly or indirectly connected to the others by the direct and indirect social interactions of their participants’ (p. 727). This reformulation of setting gives primacy to its interactional dimension (first order), rather than a spatial one (second order). In this view, the lens in which we synthesise findings caters to multiple and overlapping social networks, interactions or relationships wherein the (transgender) person is construed as simultaneously agentic and embedded in larger social structures or settings (eg, family, medical institutions, culture and laws). Instead of previously viewing ecological settings as ‘passive’ social holders where people interact, a networked approach reframes the focal unit of a review project into mapping interactive patterns or flows of enabling and constraining forces across time wherein (trans) people are embedded in. In particular, we aim to critically evaluate the enabling and constraining interactional patterns influencing transgender persons (dis)engagement with HIV prevention and treatment programmes.
Background
Health disparities and the HIV care continuum
Health disparities still contribute to the challenges documented across the broad spectrum of HIV care continuum.13 14 In this context, an important barrier to HIV care engagement is access to HIV programmes and services experienced by diverse ‘at-risk’ groups.15–17 Scoping the HIV care literature, the often sedimented intersections of risk are marked by social, political, cultural and geographical axes of gender, sexuality, age, race or economic wealth inequalities.18–22 In turn, these differential axes are strongly linked to poor access to different steps of health services that fall under the HIV care continuum such as HIV testing and awareness of HIV status, cluster of differentiation 4 cell count, access to health insurance, HIV care linkage and retention, adherence to ART and viral suppression.23–26
Among various at-risk groups, an underlying mechanism that perpetuates the intimate coupling between health disparities and practical outcomes is enacted through forms of stigma and discrimination.27 For example, recent reports on violence against transgender persons in Pakistan or the USA reflect a form of stigma experienced in their everyday lives, whereas other countries like Malaysia and Indonesia endorsed punitive laws and policies that convey more ‘fossilized’ or structural forms of discrimination.28–31 Specifically, in some countries (eg, Ukraine and China), provision of HIV care services and medication may also intersect with other structural policies (eg, drug policies) that underpin violations of human rights issues (eg, coerced treatment and rehabilitation, and harassment) among certain vulnerable HIV subgroups like those drug injecting.32 33 In this contexts, some scholars have conceptualised minority stress experienced by groups with stigmatised identities (eg, transgender and MSM) to explain negative health outcomes.34–37 We can infer from the theorising of stigma and minority stress that health disparities depict a bounded or limited exercise of one’s life choices to improve both physical and mental well-being. These ideas are reminiscent of the complex relationship between personal agency (ie, choice-based life conduct) and social structures (ie, life chances) evident in critical health literature.38–40 In other words, life chances are unequally structured and limit personal agency in the context of healthcare access, treatment and medication.
Recent review studies on HIV stigma and HIV test reuptake advanced innovative approaches to generate programme theories in this domain. For example, Thapa and colleagues41 42 developed a scoping review from a realist orientation that further unpacks possible casual links between context, mechanism and HIV programme outcomes in low-income and middle-income countries. Such review protocols that are attentive to structuring mechanisms embedded in context, or in our case settings, are vital in synthesising evidence often (re)produced in complex systems. However, theory-driven and context-critical review projects are still scant. Thus, it is within this overarching critical systems perspective that we contend the need to employ analytical approaches to review projects that recognise the duality of agency and structure in synthesising findings about HIV healthcare disparities.
Introducing our review case
In the past years, we have witnessed an increase in the number of studies investigating HIV disparities among transgender persons as a subpopulation worldwide.1 As a vulnerable community, transgender persons experience multiple negative stressors (eg, layered stigma and discrimination) accruing over time and cutting across personal, social, cultural and systemic spheres of life.43 44 In turn, these pre-existing marginalising conditions significantly contribute to poor physical and mental health outcomes. In the context of HIV care, transgender persons, in general, are found to have low HIV status awareness, uptake of ART, linkage and retention in care and virological suppression.45–47
The work of Poteat et al 7 further articulated how health disparities faced by transgender persons are embedded in stigmatising healthcare encounters, social interactions or networks. In a health provider–patient relationship, interpersonal stigma is reinforced in subjective experiences of prejudice, ambivalence, uncertainty and discrimination. Some scholars, however, identified provider and patient level barriers to healthcare alongside institutional barriers.48 Robust findings on barriers to transgender healthcare across the different levels are manifested in forms such as the risk of denial of care and treatment, concerns about confidentiality, transphobia, perceived cost of medical care and provider’s lack of medical knowledge related to transgender issues.49–52 These barriers to transgender healthcare reflect the continuous challenge of making transgender lives visible against an insidious politics of social erasure.53
In response to these challenges, more researchers now focus on explaining factors that influence effective engagement in HIV care prevention and intervention programmes specific to transgender contexts.54 55 For example, scholars further identified factors contributing to vulnerabilities of distinct subgroups such as trans women of colour, transgender youths (often collapsed as part of lesbian, gay, bisexual and transgender (LGBT) youths), trans women who are sex workers, trans men and trans women living with HIV.56–60 Scholars and practitioners also explored innovative modes of delivering relevant HIV programmes to enhance reach and coverage such as introducing HIV self-testing, using online platforms and face-to-face or blended approaches.61–63
Some of the studies have also explained how the social networks and social support positively affect transgender individuals’ intrapersonal factors, such as psychological well-being and self-efficacy to cope with minority stress or stigma and increase their ability to access HIV care.64 65 However, transgender individuals with less social support might address psychological challenges more negatively, which may ultimately influence their HIV care-seeking decisions, especially in the latter stages of treatment (eg, outpatient HIV care). Analysing a large sample of HIV infected adults enrolled in various clinics (n=22, 984), the study of Fleishman and colleagues66 examined the establishment, retention and loss to follow-up in outpatient HIV care. Their findings showed that 21.7% of patients never established HIV care after initial visits; among those who established HIV care, only 20.4% had regular visits to monitor their condition and remained in care indefinitely. Unfortunately, authors excluded from the analysis a small number of transgender people receiving outpatient HIV (n=156) for reasons they have not explicitly articulated. Nevertheless, the sheer low number of transgender people enrolled in outpatient care shows a gap in HIV care engagement that needs to be addressed.
Collectively, these studies tackle different phases on the HIV care continuum or cascade, starting from HIV diagnosis, linkage, retention and re-engagement to HIV care.67 However, we argue that distilling concrete and contextualised insights from existing studies on transgender persons and their engagement in HIV care may be difficult because: (A) a systematic approach to combining insights from studies that synthesised the enabling and constraining interactions related to engagement among different transgender groups across the levels in the HIV continuum is lacking; (B) lack of analytical approach to review projects that recognises the duality of agency and structure in synthesising various findings; and (C) experiences of transgender persons are often homogenised in HIV interventions and thus de-emphasise the contextual structuring mechanisms such as race, social class, age, HIV status and so on and how these mechanisms ultimately link with relevant HIV prevention and treatment. In response to our own plead for a more holistic approach to studying the literature on transgender persons’ (dis)engagement with care, we propose to work from an Ecological System Theoretical Perspective, further outlined below.
Theoretical framework
We mainly adapt a networked perspective12 to Bronfrenbrenner’s ecological systems approach to identify, sort and review existing studies on engagement in HIV care prevention and interventions among diverse groups of transgender persons. The choice of analytical lens is mainly informed by our desire to refocus and contribute to greater understanding of the interplay between agency and structures in public health interventions.39 This perspective promotes the idea that the person (ie, transgender persons) is embedded in networked settings (ie, microsystem, mesosystem, exosystem, macrosystem and chronosystem) wherein a setting is a pattern of social interactions between various stakeholders that occur in particular spaces.12 As such, the synthesis is sensitive to the active role of transgender persons (ie, agency) as they (re/dis)engage in life affirming and/or crippling encounters within HIV healthcare systems or structures. For this review project, we operationalise the elements of perspective given the following (but not limited to these) parameters:
Microsystem: a set of people engaged in social interactions—that includes the (focal) transgender person who experiences a host of process enablers and constraints (eg, set of patterned interactions between transgender persons and immediate stakeholders such as family and peer contexts).
Mesosystem: interactions between two or more microsystems or superimposed levels of interacting structures and determinants; does a study account for how people from two different settings interact to shape engagement in the HIV care continuum? (eg, transgender persons interacting with medical/health professionals).
Macrosystem: set of prevailing sociohistorical process/events (eg, gender/sexual identity ideologies) about transgenderism and HIV indirectly shaping the pattern of social interactions between transgender persons and other stakeholders; how do these meanings influence care engagement in the HIV care continuum?
Exosystem: existing antihomosexuality laws and policies on (public/private) healthcare indirectly affecting care engagement in the HIV prevention and treatment programmes; type of country (eg, low income and middle income).
Chronosystem: patterns of continuity or change in the interactions across levels of the HIV care continuum (eg, changes in the type of social support or felt stigma from initial seeking of HIV treatment, adherence to retention) and across ecological settings (eg, changes in health or LGBT policies).
We will use this networked perspective as a logical structure for our systematic review. In the first order analysis, process enablers and constraints describing the spectrum care engagement with HIV prevention and treatment programmes are identified and mapped across the different ecological systems. In the second order analysis, different patterns of interactions between (focal) transgender persons and other stakeholders (eg, family and doctors) are mapped and thematised (ie, enabling and constraining) in relation to the spectrum of user engagement in HIV care continuum.
Methods
We have registered this study on PROSPERO.
Objectives and research questions
The objectives of this review protocol are to increase our understanding of: (A) interaction patterns between different system levels that influence transgender persons’ engagement with HIV prevention and care programmes and (B) the role of context, culture and personal dispositions in different levels of care engagement. In addition, we aim to formulate suggestions on how to positively influence care engagement of different transgender population groups.
The following questions will be guiding the review project
What are the enabling and constraining patterns of interactions between transgender persons or transgender subgroups and other stakeholders in relation to programme engagement and HIV treatment outcomes?
How do these different patterns of interactions relate to the different ecological settings identified (ie, micro–meso–macro–exosystems)?
What are the changes, if any, in these patterns of interactions across levels of HIV care engagement? What are the changes, if any, in these patterns of interactions across ecological systems (ie, chronosystem)?
Search strategy
Information resources
We will perform a systematic electronic database search in the following databases: PubMed, Scopus, ERIC, Embase, Web of Science, Sociological Abstracts, PsychInfo, Social Services Abstract in January 2019. We will also perform an opportunistic purposeful searching process in ‘Google Scholar’ and Proquest Dissertations and Theses in order to retrieve potential unpublished documents related to the topic of interest to enhance the possibility of identifying ‘grey’ literature. The search will follow an iterative process wherein additional studies or references will be culled from primary studies that might suggest contextual variations, user engagement in HIV care continuum, facilitators and barriers, and other transgender subgroupings. The publications included are written in English.
Search terms
The key search terms are as follows:
‘HIV’ OR ‘Human immuno-deficiency virus’, OR ‘Acquired immuno-deficiency Syndrome’ OR ‘AIDS’ OR ‘HIV/AIDS’ OR ‘HIV positive’ OR ‘HIV negative’
AND
‘continuum’ OR ‘cascade’ OR ‘HIV testing’ OR ‘awareness’ OR ‘HIV status’ OR ‘disclosure’ OR ‘cluster of differentiation 4 cell count’ OR ‘CD4 cell count’ OR ‘linkage to care’ OR ‘linkage to HIV care’ OR ‘HIV care retention in care’ OR ‘adherence OR viral suppression’ OR ‘ART initiation’ OR ‘Antiretroviral Therapy’ OR ‘Highly Active[MeSH]’ OR ‘Anti-Retroviral Agents[MeSH]’ OR ‘Antiviral Agents[MeSH]’ OR ‘HIV treatment access’
AND
‘transgender women’ OR ‘transgender men’, ‘trans women’ OR ‘trans men’ OR ‘TG’ OR ‘TW’ OR ‘trans feminine’ OR ‘trans masculine’ OR ‘transgender persons’ OR ‘FTM’ OR ‘MTF’ OR ‘female to male’ OR ‘male to female’ OR ‘MSM’ OR ‘men who have sex with men’ OR ‘transgender’ OR ‘hijra’ OR ‘kathoey’
AND
‘Evaluation’ OR ‘programs’ OR ‘engagement’ OR ‘HIV testing’ OR ‘self-testing’, ‘Pre-prophylaxis’ OR ‘PreP’ OR ‘reducing stigma’ OR ‘online’ OR ‘face to face’ OR ‘short term care’ OR ‘long term care’ OR ‘HIV testing’ OR ‘satisfaction with care’ OR ‘treatment adherence’ OR ‘treatment retention’ OR ‘treatment effectiveness’ OR ‘HIV counseling’ OR ‘mental health services’ OR ‘medical services’ OR ‘psychological services’ OR ‘help seeking behaviors’ OR ‘implementation’ OR ‘stigma’ OR ‘social support’ OR ‘awareness’ OR ‘health evaluation’ OR ‘religion’ OR ‘anti-gay’ OR ‘anti-homosexuality’ OR ‘anti-discrimination’.
Study inclusion and exclusion criteria
Study types
The review process will include published and unpublished primary studies presenting qualitative or mixed research evidence to understand the enablers and constraints or the contextual factors influencing effect of the interventions. The empirical qualitative studies that are to be included should use recognised qualitative methodologies/methods of data collection (eg, individual interviews, focus group discussions, ethnographic interviews and participant observation) and analysis (eg, thematic/content analysis, phenomenological approaches, narrative analysis, constant comparative method and discourse analysis). The mixed methods studies should include qualitative research information that describes (the interaction of) process and implementation factors with engagement in care or with particular outcomes achieved.
We will only include evaluation studies in our review when they contain qualitative, process and implementation related research information that helps to explain whether, how and why particular interventions worked out to produce certain outcomes. For domains of study that are not well covered by empirical research evidence, we will also include textual, opinion, theoretical or other non-empirical research studies.
Screening
An initial screening of title, abstracts and keywords of the documents that will be identified in the initial search will be performed. Two reviewers will independently assess the relevance of the content for further synthesis using the following criteria:
In the first phase, the following criteria will be looked on for inclusion:
The abstract describes/refers to outcome measures related to at least one of the levels of the HIV care continuum (aware of HIV infection; receiving/psychological care but not HIV care; entered HIV care but not lost to follow-up; cyclical or intermittent User of HIV care; and fully engaged to HIV care).
The (intervention) study enrolled or included transgender persons and are transgender persons identifiable as a subgroup within a potential larger group of participants studied.
The abstract reports on empirical methods that study enabling and constraining factors and their impact on particular outcomes and/or apply methodologies to qualitative data collection and analysis as described above.
The publication is written in English.
Included papers have been published before 1 January 2019.
In the second phase, the abstracts from the first phase will be checked specifically against any one of the following three criteria:
Does the abstract refer to either/both enablers and constraints with user engagement among any transgender subgroups?
Does the study describe/evaluate experiences, understandings or levels of engagement of transgender persons related to HIV prevention and treatment programmes?
Does the abstract report feature of the cultural context (of the study/intervention) such as, but not limited to, time period, ethnic groupings, age groupings or socioeconomic groups?
Does the abstract explicitly report on the mode of service delivery for HIV prevention and intervention?
Abstracts will be coded as ‘Yes’ if either one of the four inclusion criteria are satisfied, and ‘No’ if none of the criteria are met. After the screening of abstracts for the second time, the full text of articles will be retrieved and evaluated by two independent reviewers to ensure that one or more of our inclusion criteria are met and the study/intervention should be included in the review. Disagreements about articles to be included and excluded will be resolved through consensus between the reviewers. We will use EndNote X8 to import references from the databases, delete the duplicate references, perform the preliminary screening of the titles and abstracts and store the references that are included for the full-text review.
Quality appraisal
To assess the quality of primary studies, the Mixed Methods Appraisal Tool will be used. It is one of the few tools that developed a consistent set of assessment criteria for use in reviews that include a diverse range of empirical study designs, while maintaining its sensitivity to the specific characteristics of qualitative, quantitative and mixed-method studies. It offers a separate set of criteria for each of these study types. The quality of non-empirical studies, text and opinion will be evaluated by using JBI QARI critical appraisal tool. We will not make decisions to exclude any of the studies based on the study quality. Papers will be selected based on the relevance of the study topic for the review and its contribution to the development of the ecological system theory. However, the quality of the studies is discussed to provide readers with a baseline measurement of quality.
Population
In this review project, transgender is defined as persons whose gender identity or expression is different from their sex labelled at birth (eg, trans women are people who identify as female/woman or on the transfeminine spectrum but who were labelled male sex at birth). Although gender identities are culturally complex and fluid, an exhaustive definition of gender identities or expressions is beyond the scope for this review project. We also include transgender persons irrespective of HIV status or whether they have undergone sexual reassignment or surgical procedures. The studies that have both trans participants and other population groups (eg, health workers and general population) may provide information to understand the interaction patterns between different system levels influencing transgender persons’ engagement with HIV prevention and care programmes and thus should be included for synthesis in the review. Since our review is targeted among transgender people, only the data related to the transgender people’s engagement with HIV care will be synthesised.
Topic/outcomes of interest and what we evaluate
We consider all papers related to exposure (ie, exploratory or explanatory) and evaluation type of studies related to engagement with treatment/care in any level in the HIV care continuum.68–70 HIV care continuum is understood as the series of steps a person with HIV takes from initial diagnosis through their successful treatment with HIV medication. Each level in the continuum is further operationalised in terms of HIV prevention/treatment outcomes (see table 1):
Level of HIV care continuum in terms of prevention/treatment outcomes
Patient and public involvement
There was no patient and public involvement in this protocol.
Data extraction, analysis and synthesis
Data extraction (selection and coding)
Studies will be included in the review based on relevance, that is, the extent to which they inform the research questions and clarify or refine the application of an ecological systems perspective. Data will be extracted from the article based on a data extraction tool by the lead author.
The following extraction dimensions are considered:
Study identification details: authors, title, country, publication date and date of study.
Qualitative type of research studies: purpose, research questions, methodology/framework, methods, process enablers and constraints to user engagement.
Intervention process and implementation characteristics and objectives (process evaluation) as reported in quantitative, qualitative or mixed studies: details of what was done in a programme, duration, target subgroup, study type, comparison, mode of service delivery, participants actual participation in the programme (ie, reach), participant drop-out rates (ie, attrition), participant’s attitudes or feeling about the programme (ie, participant engagement), provider’s attitudes or feelings about the programme (ie, provider engagement), time of the evaluation, level of evaluation and method of evaluation, perceived or actual effectiveness and challenges of mode of service delivery.
Factors influencing implementing evaluation studies (action model): implementing organisation, implementer, associate organisations and community partners and target population.
Where reported, the change model of the intervention study: articulation of a priori programme theory/model of change pathways.
Narrative description of association between role out of programme and outcome.
Type of transgender subgroup: gender identity? Sexual orientation? HIV status? Other characteristics? (eg, young/old).
Mechanisms/processes or reported underlying assumptions: for quantitative, qualitative or mixed research studies, descriptions of how and why specific process enablers and constraints are important to consider for particular transgender subgroup; for evaluation type of research studies, descriptions on how and why the programme may have worked in particular contexts.
Geographical context (if applicable): description of the location of the research.
Cultural context (if applicable): description of cultural features such as, but not limited to, the following: time period, groupings based on ethnic, age, socioeconomic status, age, gender or lifestyle dimensions.
Groups represented in the paper (for textual non-research studies only): to whom the paper refers or relates to.
State allegiance/position (for textual and non-research studies only): short statement summarising the main thrust of the publication.
Logic of argument (for textual and non-research studies only): an assessment of the argument’s presentation and logic. Is other evidence provided to support assumptions and conclusions?
A randomly selected 10% of the retrieved studies will be checked by a second member of the research team to pilot the data extraction form and where necessary optimise it to prevent from ambivalence in the extraction tool proposed that may lead to disagreements on the type of papers selected for the review.
We will use the networked systems approach, operationalised in the background section, to first organise and map enablers and constraints to engaging with prevention and treatment programmes on the HIV care continuum among transgender persons. Second, the relevant layers of the ecological systems perspective will be used as guidance to interrogate and unpack salient conditions and processes (ie, in the framework, this refers to the networked systems) that explain why and how conditions/systems interact to impact treatment outcomes and experiences of the transgender population. Third, we will organise and map networks of stakeholders including a description of the nature of their interactions (ie, labelling arrows/connections between nodes). Fourth, an analysis of similar and unique factors per transgender subgroup in relation to opportunities/challenges of modes of service delivery (ie, technology based, face to face, combination and so on) will be conducted.
When extracting data, if an article does not include relevant information to a review question, the extractor will record ‘Not reported’. Direct quotations from the articles are valuable source of information and will be accompanied by the page number from which the quote is taken. Combination of elements or categories from the data extraction tool will be used to form relevant evidence tables to answer the research questions. The data extraction form will be pilot tested on at least five purposely selected articles.
Strategy for data analysis and synthesis
The analysis and synthesis will follow the following steps:
Organisation of extracted data into evidence tables: the data extracted from each study using the data extraction tool will be summarised and organised in one or more evidence tables. The evidence tables will also include the link back to the source papers. Extraction of relevant categories are guided by an ecological systems framework (see summary of data extraction tool).
First-order analysis of linking ecological systems to levels of engagement: using a 2×2 nested matrix (see sample table 2 below), the first order of analysis describes how ecological systems link or interact with levels of user engagement in HIV care among transgender persons. Each ecological system (column) is further divided into the identification of enablers and constraints. The combination of these processes is content analysed (ie, identification of categories and frequencies/weights/percentages) in relation to the six levels of care engagement. In general, each cell describes the relative weight of processes in relation to a specific level of care engagement.
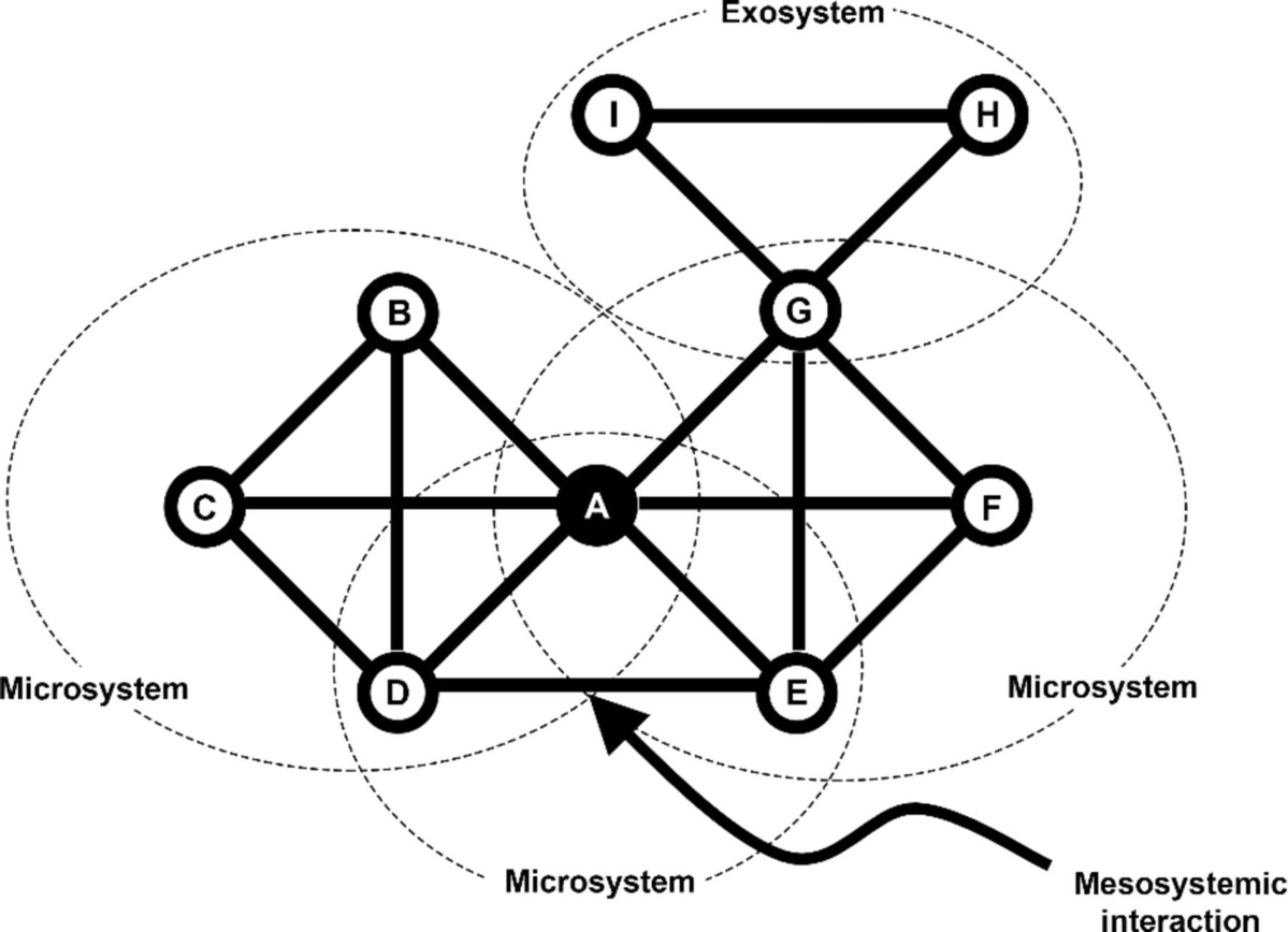
Second-order analysis of mapping patterns of interactions between stakeholders using a social network model/s (ie, nodes and connectors), the second order analysis describes the (shared and unique) patterns of interactions between stakeholders—including transgender persons (focal) arranged either by transgender groups, modes of service delivery, contexts (eg, sociocultural contexts—western/Asian/eastern) and so on. In the literature, social network analysis is mainly used to make sense of patterns of relationships among interacting members of a group/network.71 Interactions between members can be described in terms of nature of participation, degree of influence, group cohesion, degree of connectedness or centrality of members in relation to group/network behaviour.72–74 More recently, this method of analysis has also been applied to explain interactional processes in HIV prevention and care.75 However, in conducting systematic reviews, this analytic technique has not been applied to organise process and implementation related evidence and qualitative findings from a network perspective.
In this review project, we define each node as representing a relevant stakeholder, whereas the connectors show the strength of relationships or relative weight between stakeholders across overlapping ecological systems. The strength of relationship between stakeholders is determined through the frequency of citations in reviewed articles (ie, the article needs to explicit link stakeholders or identify the relationship as important to increase user engagement in HIV care). Taken from Neal and Neal’s proposed ecological network model, see hypothetical figure to illustrate sample mapping of interactions among transgender persons. Mapping can also be performed per transgender subgroups (see figure 1).
Performing a narrative synthesis. The last step includes weaving a coherent narrative that relate significant patterns in the matrix and relationships in the networked models. The mapping exercise will mainly inform new insights regarding: (A) the dynamics between process enablers and constraints per system as it intersects with different levels of user engagement in HIV care; (B) the evaluation and improvement of existing HIV prevention and evaluation programmes based on user engagement among transgender groups; (C) the nuancing of transgender groups and how it impacts culturally sensitive engagement with different stakeholders and (D) the identification of key relationships (ie, alliance/collaborations) between transgender groups and other sstakeholders that can impact mode of service delivery.
The 2×2 nested matrix of HIV care engagement across ecological systems

{kind=link}
Networked model of ecological systems, focused on transgender persons.
Knowledge dissemination
Results of this study will be disseminated to academic and non-specialist audiences through peer-reviewed publications, conferences and presentations to policymakers and practitioners. Evidence generated from this synthesis will be used to inform the development of a theory-driven, context-critical and evidence-based interventions aimed at targeted information campaign towards organisations that work with the population of interest.
Discussion
This review protocol emphasises the importance of a system-based perspective to study the complexity of interaction patterns of vulnerable populations, in this case transgender people. It takes a temporal dimension (chronosystem) into account to study how flows or patterns of interactions may persist or change under the influence of different systemic levels, in this review identified as microsystem, mesosystem, macrosystem and exosystem. It will contribute to a fuller understanding of the interactional patterns that either enable or constrain transgender persons’ engagement with HIV care programmes.
The Joint United Nations Program on HIV/AIDS’ (UNAIDS) aims for 90% of people living with HIV to know their status, 90% of people with diagnosed HIV infection to receive ART and 90% of people taking ART to be virally suppressed.76 The strategy also sets a target for key populations, including transgender people. Of all populations affected by HIV, evidence suggests that transgender population has the heaviest HIV burden worldwide.1 However, transgender population is among the groups who are often left out from mainstream HIV care interventions, and little is known about HIV linkage and care outcomes among transgender population.55 UNAIDS 90-90-90 strategies are unlikely to be effective for transgender people without an enabling environment that enables for an easy access to healthcare for transgender people.77 Thus, a synthesis of qualitative evidence, which combine and analyse evidence from individual qualitative studies, would address implementation considerations and clarify the interplay between stakeholders, health systems and context among hard-to-reach population groups (transgender population) across diverse country settings and complex health systems.
One of the preconditions to increase access to HIV care programmes among at-risk population groups, including transgender people, is the reduced level of stigma in the community and healthcare. However, stigma reduction interventions are seldom implemented and those implemented do not sufficiently consider contextual influences while addressing complex health behaviours, such as HIV test uptake, initiation of ART and retention in care.42 Our review may provide evidence to understand the essential components that should be considered in any stigma reduction interventions in terms of addressing transgender people’s access to HIV care cascade. For example, unless equal rights for transgender population are ensured by law, HIV care interventions may not be effective to increase the participation of these specific population groups in HIV care and prevention. Thus, policies, such as legal and social recognition of same-sex relationships or marriage and protection of sexual minority people from discrimination, should be implemented along with HIV care interventions to reduce stigma and increase access to HIV care among the vulnerable and hard-to-reach population groups.78
One can imagine that in a context where transgender population and people living with HIV both are stigmatised, access and uptake of HIV-related services among transgender people would increase when such services are offered at a non-clinical setting because of easy access and perceived confidentiality. Examples of HIV care services in a non-clinical setting include home-based HIV testing, self-testing for HIV and home-based care and treatment programmes. However, in a conventional clinic set up, involving transgender people in providing HIV care could be promising to reduce discrimination at healthcare. These important intervention approaches could be adapted and prioritised while targeting transgender population to link this population and insure retention in HIV care programmes. Therefore, the qualitative evidence generated by the review could be useful for policymakers and programme managers.
Our review might have some limitations. A key limitation of this review that we will only include the studies written in English. As a result, our review may miss some studies written in other languages. However, we will include and synthesise research evidence generated from multiple types of studies (ie, quantitative, qualitative and mixed methods) providing information about enabling and constraining factors of interventions, contexts and mechanisms of change related to particular outcomes, surrounding the HIV care continuum among transgender people. We also encourage authors to adapt or translate the framework in their local context and consider other relevant dimensions such as transgender subgroupings, cultural-specific facilitators and barriers to treatment adherence. In this way, the review will bring together a comprehensive and context sensitive to the analysis and synthesis.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
Footnotes
Patient consent for publication Not required.
Contributors NC conceived of the protocol and was responsible for the conceptualising the framework and overall design, tables and figures. ST and KH were responsible for refining the search strategy and planning the strategies for quality appraisal, data extraction, analysis and synthesis. The initial draft of the manuscript was prepared by NC then circulated among all authors for critical revision. All authors helped to evolve the writing of the literature review, framework, data extraction, analysis and synthesis plans and critically revise successive drafts of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.