Article Text

Abstract
Objective The benefits of internal whistleblowing or speaking-up in the healthcare sector are significant. The a priori assumption that employee whistleblowing is always beneficial is, however, rarely examined. While recent research has begun to consider how the complex nature of healthcare institutions impact speaking-up rates, few have investigated the institutional processes and factors that facilitate or retard the benefits of speaking up. Here we consider how the efficacy of formal inquiries within organisations in response to employees’ speaking up about their concerns affects the utility of internal whistleblowing.
Design Using computational models, we consider how best to improve patient care through internal whistleblowing when resource and practical limitations constrain healthcare operation. We analyse the ramifications of varying organisational responses to employee concerns, given organisational and practical limitations.
Setting Drawing on evidence from international research, we test the utility of whistleblowing policies in a variety of organisational settings. This includes institutions where whistleblowing inquiries are handled with varying rates of efficiency and accuracy.
Results We find organisational inefficiencies can negatively impact the benefits of speaking up about bad patient care. We find that, given resource limitations and review inefficiencies, it can actually improve patient care if whistleblowing rates are limited. However, we demonstrate that including softer mechanisms for internal adjustment of healthcare practice (eg, peer to peer conversation) alongside whistleblowing policy can overcome these organisational limitations.
Conclusion Healthcare organisations internationally have a variable record of responding to employees who speak up about their workplace concerns. Where organisations get this wrong, the consequences can be serious for patient care and staff well-being. The results of this study, therefore, have implications for researchers, policy makers and healthcare organisations internationally. We conclude with a call for further research on a more holistic understanding of the interplay between organisational structure and the benefits of whistleblowing to patient care.
- internal whistleblowing
- speaking-up
- raising concerns
- health quality improvement
- resource limitations
- simulations
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- internal whistleblowing
- speaking-up
- raising concerns
- health quality improvement
- resource limitations
- simulations
Strengths and limitations of this study
This work uses computer simulations to test the utility of several whistleblowing policies in a variety of organisational contexts. This methodology offers a fast and cheap mechanism for detecting potential problems in implementing whistleblowing policy.
This work is one of the first to use simulations to analyse the repercussions of whistleblowing policy when report resolution is constrained by time, accuracy and effectiveness.
All models will oversimplify the complex dynamics of a working healthcare institution. The below models suggest that certain policy may require organisational restructuring to maximise its utility. However, empirical study is required to diagnosis whether existing healthcare organisations are as vulnerable as the models suggest.
Introduction
The act of employees reporting poor practice has been variously labelled as whistleblowing, ‘raising concerns’ or ‘speaking up’. The use of the latter two terms have become more commonly used within healthcare, as the term whistleblowing is often regarded as having negative connotations related to ‘grassing’ or ‘snitching’ on colleagues.1 2 The terms are often used interchangeably (as we do here), as seen in the current National Health Service (NHS) policy document in this area titled ‘Freedom to speak up: raising concerns (whistleblowing) policy for the NHS’.3
This paper focuses on employees who whistleblow, or speak up, internally within their organisations when they witness poor care, rather than speaking up to external organisations such as healthcare regulators or law enforcement agencies. Poor care has been defined as involving acts of neglect, abuse or incompetence and should be differentiated from error which is the unintended consequence of a genuine mistake or mistakes.4
The frequency with which poor care occurs within healthcare is difficult to measure or predict, and any attempt at estimation is hampered by complexity and that healthcare employees have long reported reluctance in raising concerns within the organisations in which they work. For example, recent inquiries into systematic failings in the UK healthcare sector5–7 suggest that incidents of poor care of the most egregious type occurred on multiple occasions, in multiple settings, over a prolonged period of time. In addition, a survey of nearly 1600 nurses found that 73% of respondents felt they were too understaffed to provide safe, dignified and compassionate care.8
Whistleblowing in healthcare
In the healthcare sector, few disagree that care is improved where employees are able, willing and supported within their organisation to speak up about poor care. In the long term, employee internal whistleblowing may even prove cost-effective to the institution.9 10 Despite this, employee internal whistleblowing is still not ubiquitous.11 Whistleblowing rates differ by nation states,12–14 workplace culture15–17 and organisational topography.1 18 For example, employee surveys show that whistleblowing rates are correlated to the perceived efficacy of and institutional/managerial response to reporting.19 20 Similarly, more proximate sociocultural workplace dynamics and a sense of loyalty to work colleagues have also been shown to negatively affect whistleblowing behaviour.2
Unfortunately, employees’ hesitation to report poor practice is often warranted, as whistleblowers face bullying by colleagues, negative emotional/physiological effects and job loss.21–25 Health employees appear cognizant of these dire consequences and often refuse to whistleblow for fear of reprisal and an apprehension about the efficacy of reporting.26–28 As a consequence, significant research, policy and legislation has sought to curb such reprisals and to protect whistleblowers.29–34 The implication being that improved protection will always lead to an increase in whistleblowing and a subsequent reduction in poor practice leading to benefits to patient care and employee well-being.
Given all the moving parts of an institution, it has been argued that culpability for the lack of whistleblowing cannot be placed solely on the healthcare worker.35 However, while research and governmental inquiries have provided insights into the complex nature of healthcare institutions and the cultural factors that inhibit whistleblowing, surprisingly little empirical work has considered how internal institutional processes could actually inhibit or promote the benefits of employees speaking up.
Promoting whistleblowing in the workplace: an exemplar
A notable success story in terms of an institutional attempt to increase the numbers of concerns raised internally by employees comes from the Virginia Mason Medical Center (VMMC) in Seattle, USA. In 2002, VMMC introduced the Patient Safety Act (PSA) system following a staff survey that showed that most employees believed that if they raised concerns they would be punished and that information generated from concerns would not improve the safety of care. The PSA system encourages employees to report actual safety lapses (such as medical errors) and near misses in safety and also all events that could impact on the safety and well-being of a patient. As a result of the introduction of the PSA system, from March 2002 to January 2014 staff raised concerns a total of 43 615 times. This has grown from an annual reporting frequency of 10 or so concerns a year in the period 2002–2004 to 850 concerns a month in January 2014. As a result, between 2004 and 2014, there was a 74% reduction in insurance liability premiums paid by staff, indicating a major shift in ‘risk perception’ by insurers. Factors underpinning this success include the introduction of a learning culture, where instead of criticising or silencing employees who speak up, managers and executives were trained to offer support and resources to fix issues that concerned staff. In addition, VMMC openly share with staff information about how their concerns have led to improved safety outcomes and how, rather than victimising those who speak up, employees who raise concerns are welcomed and valued.36
Although there is little in the way of robust research that evaluates the success of the PSA system, the Department of Health in England cite VMMC as an institution worthy of imitation for using ‘openness to drive a safer culture of care’37 (p. 8). In an attempt to generate similar levels of openness and organisational learning, NHS England announced a number of strategies to encourage employees to raise concerns.38 These include the introduction in 2015 of ‘Freedom to Speak Up Guardians’ (FTSUGs) situated in each NHS organisation, supported by a National Freedom to Speak Up Guardian team, who together are tasked with making the raising and addressing of employee concerns ‘normal practice’ (p. 71) throughout the NHS.
In the near total absence of published studies or descriptions of similar initiatives, the introduction of FTSUGs is founded on a variety of assumptions that raise a host of interesting questions. For example, if the drive to normalise employee speaking up as routine practice is successful then:
Will patient care improve?
Are resources within the system able to cope with potentially hundreds or thousands of complaints per month?
What are the effects, if any, of any delays in responding to concerns on patient care and on employees’ propensity to raise concerns in the future?
In relation to the second question, it is worth recalling that VMMC, a relatively modest healthcare organisation consisting of one 350 bed hospital facility and nine satellite units employing 5000 staff, received over 800 reports of concern from staff in January 2014, although after 12 years of promoting and raising awareness of their employee concerns system. Here we set out to analyse how such an increase in whistleblowing rates can affect both the patients and the institution.
In this paper, we explore the limits of the a priori assumption that internal whistleblowing to workplace colleagues, line managers or administrators always augments the quality and safety of patient care. To answer these questions, we develop an agent-based mathematical model that considers the effects of whistleblowing on patient care. The employment of mathematical and computational modelling to investigate policy initiatives has long been employed in many sectors but, to date, has been underused in the healthcare arena.39 Applying such tools permits us to validate hypotheses without significant cost, or at a scale and rate that would be difficult to achieve with conventional research methods. In addition to addressing some taken-for-granted assumptions about employee whistleblowing, the results of testing the model will also expedite conversation between policy bodies, regulators and those charged with supporting whistleblowing in practice.
Methods
Patient and public involvement
In this work, we use computational models to attempt to better understand the repercussions of policy and organisational structure on the utility of speaking up. This method did not involve public participants or patients.
Model overview
Here we model the utility of informational transparency and whistleblowing in the healthcare sector. For the purposes of this study, the healthcare institution is composed of the following variables:
Patients.
Healthcare workers.
The practices employed by the healthcare workers that affect patient care.
The model is initialised with 20 000 workers, where 90% of practice is good and 10% of practice is bad. The game is partitioned into 10 000 rounds. During a round of play, the following events occur in order:
Round
With some likelihood i (informational transparency), a healthcare worker receives information about a coworker’s practice (eg, through working alongside and observing coworker’s practice).
If the worker believes the practice is poor, they raise concerns internally and demand an internal inquiry with probability w (propensity to whistleblow).
When a whistleblowing report is filed, then the inquiry is added to the investigation list.
Whistleblowing inquiries are resolved.
Finally, patients receive care. We assume that patients receive care equal to the fraction of good practice in the institution.
Filing and resolving whistleblowing inquiries
When the whistle is blown on a practice, a report is filed and added to the list of current whistleblowing investigations within the institution. Each investigation takes X=100 rounds to finish. We presume the inquiry is 100% accurate in its appraisal of the practice. If the inquiry is the result of bad practice, then the practice is immediately removed from the institution and replaced with good practice.
The investigation list contains all the practices currently under investigation. Each inquiry has a counter representing the number of rounds left until the investigation is complete. For example, if three practices are currently under investigation, then the list might appear as:
Practice ID #145: 45 rounds left before completion.
Practice ID #2395: 3 rounds left before completion.
Practice ID #89: 100 rounds left (just added to the list).
After each round of play, a round is subtracted from the number left until each investigation on the list has been completed. When the counter reaches zero for a practice, it is resolved, and the practice is set to good, improving patient care. The Matlab code used to run all simulations can be found in online supplementary material A and B.
Analysing the results
After 10 000 rounds of the game, the average number of good practices in the institution is calculated over all rounds. This represents the average patient care at the institution. The game is run for different parameter values, and the best model for patient care is analysed.
Model 1: the (utopic) baseline
Here we consider how patient care is affected by both informational transparency within the institution (i=[0,1]) and the propensity to whistleblow (w=[0,1]). If i<1, then there is a lack of informational transparency in the institution; workers do not always know the practices of their colleagues. If w<1, then workers do not always speak up when witnessing poor practice. We consider patient care over all possible values of i and w, analysing how differing values of transparency mixes with varying rates of whistleblowing to affect patient care.
Results
Figure 1 represents patient care over a parameter sweep of i and w. The colour shade depicts patient care. Clearly, patients receive the best care (the lightest shaded area) when information is transparent (i=1) and when employees always raise concerns (w=1).
Average patient care after 10 000 rounds.
Discussion
These results support the presumption that informational transparency and speaking-up both increase patient care. Patient care is best where employees’ practices are fully transparent to others and employees within an organisation have a propensity to raise concerns.
Model 2: finite resources: when patient care is improved by not speaking up and obfuscation of information
The previous model presumes that the time taken to review an inquiry is independent of the number of reviews currently being processed. This is not a practical assumption when resources are finite. For example, if resources are committed to looking into practice A, it may delay the inquiry into practice B. Here, we consider the repercussions of finite resources on patient care. Whenever an employee speaks up and adds a new practice to the inquiry list, a 10% increase in time is added to each inquiry. Since it takes 100 rounds to resolve an inquiry, a 10% increase means that 10 rounds are added to each inquiry in the list.
For example, presume the current inquiry list is:
Practice ID #145: 45 rounds left.
Practice ID #2395: 3 rounds left.
Practice ID #89: 100 rounds left.
If a healthcare worker raises concerns on another practice, then the resulting list would appear as:
Practice ID #145: 55 rounds left.
Practice ID #2395: 13 rounds left.
Practice ID #89: 110 rounds left.
Practice ID #9845: 130 rounds left.
Ten rounds are added to each existing inquiry. Furthermore, the new inquiry (ID #9845) starts with 100+30 rounds, because 30 rounds are added for each pre-existing inquiry already on the list.
Results
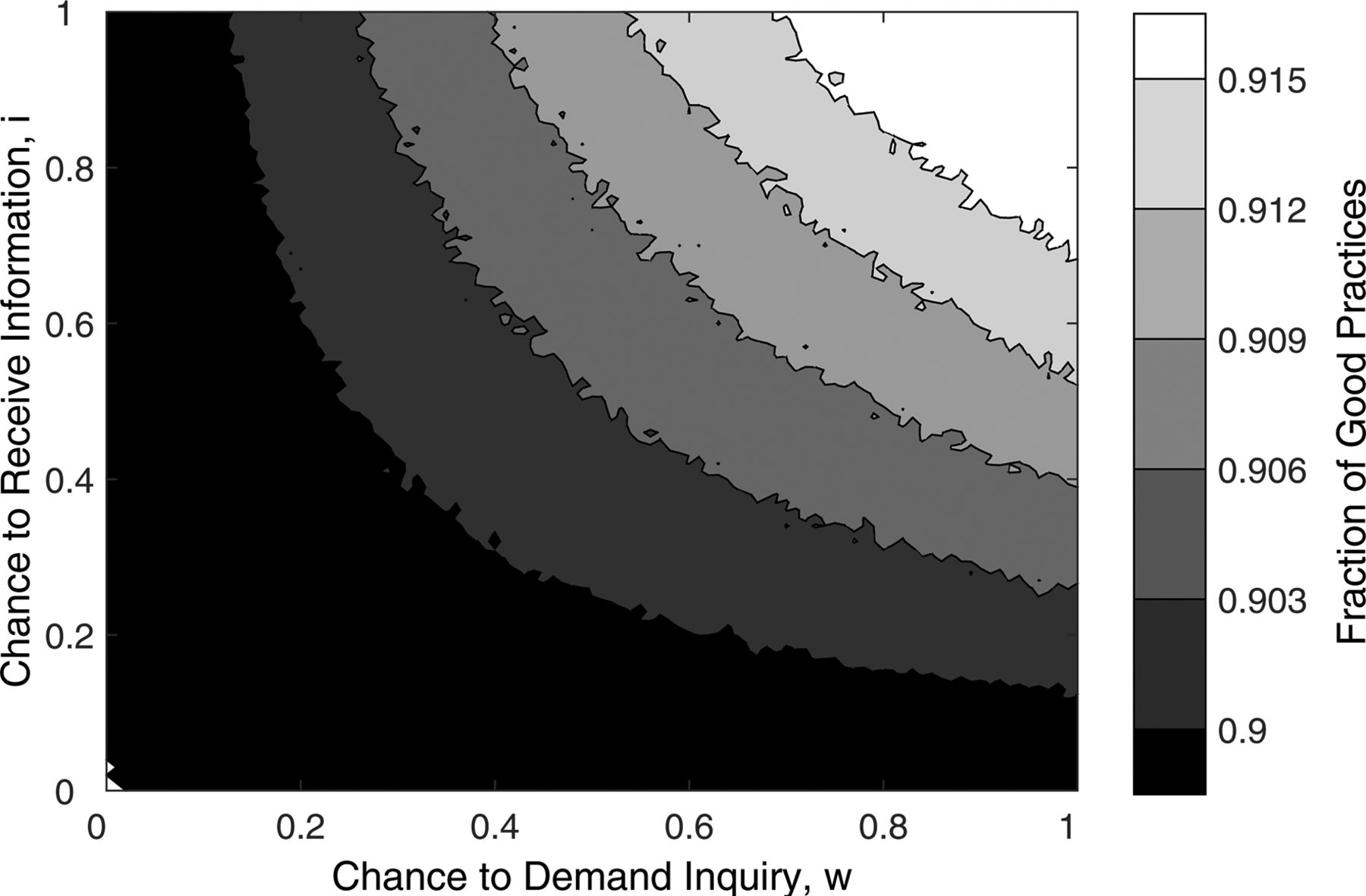
As a result of adding a 10% delay, figure 2 illustrates that informational transparency and frequent whistleblowing inhibit the correction of bad practice. If information is transparent (i=1), then patient care is best if workers only report their concerns at a rate of approximately 50%–60% of all poor practice observed. Furthermore, if policy dictates that every employee should speak up whenever they witness poor practice (w=1), then it is best for patient care if information is partially obfuscated, with workers only receiving and/or responding to information about a bad practice with a frequency of 50%–60%.

Average patient care after 10 000 rounds when inquiry time is increased by 10% per additional review.
Discussion
Model 2 shows that while raising concerns leads to the eventual improvement of a practice, where there are finite resources, it also delays internal investigation into existing and future employee concerns. This is problematic, as delays prolong the amount of time that potentially damaging practices are in circulation. Delays may also result in staff becoming disillusioned with a lack of timely response, possibly concluding that the organisation is uninterested in their concerns.
Delays and employee disillusionment can quickly be communicated to other employees potentially resulting in disenchantment.40 Paradoxically, therefore, occasionally not observing/learning about a bad practice (ie, lack of transparency), or not whistleblowing may lead to improved patient care through more timely resolution of and learning from existing investigations.
It is worth noting that delaying the resolution of an investigation by 10% is rather small. If we presume that the institution’s resources for investigating concerns is static, then the percentage delay would be 100%. Furthermore, we are presuming that the resources required to maintain an impressive efficiency of 10% does not negatively impact the resources employed for direct patient care. Both assumptions are fairly generous, but even at 10%, it is still not efficient enough to overcome the utility of failing to speak up or informational obfuscation.
In the healthcare sector, significant research, regulation and policy imperatives have sought to increase the rates of speaking up by employees and informational transparency. Here we demonstrate that increasing formal whistleblowing rates may not always prove beneficial within a context where resources are finite, as delays can occur in organisational learning and subsequent correction of existing bad practice. Yet, issues of resourcing are seldom discussed in the context of speaking up. This may be explained by recent health policy focusing on ensuring workplace cultures that promote and support internal employee speak-up cultures, with little focus on the resources required to respond to concerns. For example, the aforementioned FTSUG initiative in NHS England, if successful, may lead to the normalisation of speaking-up as a workplace activity. This is likely to increase resource demand within organisations to meet the requirement of investigating the increased numbers of concerns being raised. However, no additional resources have been provided for this activity at a time where NHS England is experiencing severe financial pressures.41 This may account for 51% of FTSUGs reporting having no ring-fenced time to undertake the role, with over 70% having 1 day or less.42
The result of the model presented here suggests that even in a world where successful implementation of FTSUGs mean that whistleblowers do not fear sanctions, it may not be in the institution’s or patients’ best interest if employees always formally speak up internally. If resources are even slightly constrained, some reduction in internal speaking up may produce better patient care by enabling existing investigations into bad practices to be resolved more quickly. This adds credence to the idea that the effects of whistleblowing cannot be considered in isolation43 and that organisation topography may impact the efficacy of internal reviews.18
Model 3: more efficient reviews
In this model, we delve into the underlying mechanisms of model 2 and demonstrate how additional resourcing or other means of achieving increased efficiency in processing inquiries empowers whistleblowing and informational transparency. Previously, each inquiry took 100 rounds to process. Now, we reduce the number of rounds per inquiry to 50. An additional 10% is still added to each inquiry when a concern is raised, but since the initial inquiry is 50, only five rounds are added.
Results
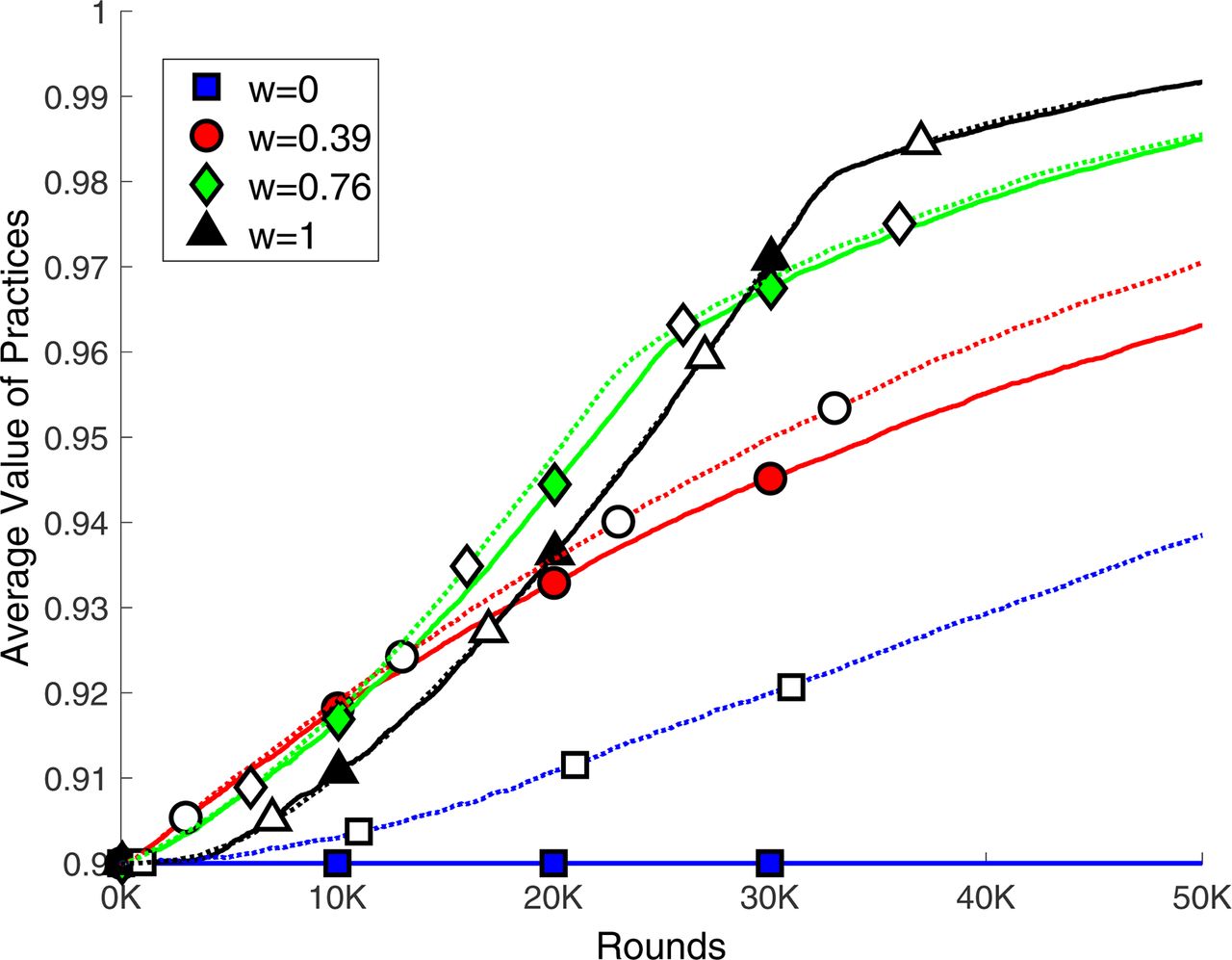
Figure 3 juxtaposes model 3 to model 2 over 50 000 rounds for certain whistleblowing rates. Previously, we considered the results of the simulation after 10 000 rounds, but including 50 000 rounds adds clarity to the underlying dynamic. Each line represents the average number of good practices in the institution over time for a given whistleblowing rate. The solid lines depict model 2, where the initial inquiry requires 100 rounds. The dotted lines depict a more efficient institution where inquiries require 50 rounds. The chance of attaining information is held static at 100% (i=1), and patient care is measured against different rates of speaking-up. The square line represents an institution where no one whistleblows (w=0); consequently, the number of good practices never increase. The other lines represent different rates of speaking-up, ranging from 39% (w=0.39) to always whistleblowing (w=1). We compared a 39% whistleblowing rate to a 76% whistleblowing rate because such rates are grounded in reality. In a large-scale Norwegian survey, 76% of those in the public sector who perceived wrongdoing raised concerns.19 In similar studies in both the UK38 and Australia,44 only 39% of those who observed wrongdoing raised concerns. It has been argued that one of the reasons for this whistleblowing disparity between institutions rests in the efficacy with which the institutions handle concerns.19 20

Percentage of good practice when a concern is resolved over 50 000 rounds for different whistleblowing rates and processing efficiencies. The chance to receive information about bad practice is held static at 100% (i=100). Solid lines: reviews initially take 100 rounds (model 2). Dotted lines: reviews take 50 rounds (model 3). Squares: no one ever blows the whistle, w=0. Circles, diamonds and triangles: w is 39%, 76% and 100%, respectively.
When inquiries require 100 rounds (solid lines), for the first 10 000 rounds, patient care improvements are hindered by constant whistleblowing. Since high whistleblowing rates result in frequent inquires, the resolutions of existing inquiries are delayed and patient care suffers. As a result, a situation where employees do not always formally speak up (w<1) outperforms unconditional speaking-up (w=1). However, although frequent speaking up delays inquiries, once the inquiries begin to resolve, a higher number of bad practices are corrected. In figure 3, for the first 10 000 rounds, 39% whistleblowing (circle line) outperforms 76% (diamond) and 100% (triangle) whistleblowing. However, after round 11 693, w=76% overtakes w=39%, demonstrating that the reduction in the number of bad practices is improved if whistleblowing rates are more frequent. At round 18 009, always speaking up (w=100%) passes w=39%, and at round 28 690, w=100% passes w=76%. The dotted lines in figure 3 depict model 3 over 50 000 rounds. Clearly, unconditional whistleblowing (w=1) outperforms all other strategies well before 10 000 rounds. Though it is difficult to see in the graph, by round 297, w=100% surpasses w=39%. Furthermore, w=100% outperforms w=76% at round 317.
Discussion
It is known that practitioners in institutions with highly effective formal review processing are more likely to speak up compared with those in less effective institutions. For example, a key principle of the VMMC system, described earlier, is that employees receive timely feedback on reported concerns, as well as examples of how internal speaking-up has led to practice improvements. As a result, other employees are encouraged to speak up, 76% of Norwegian health and education sector employees raise concerns when they observe wrongdoing in the workplace, a very high proportion compared with whistleblowing in Australia, the USA and UK.19 45 One reason for such a high proportion of speaking-up by employees is that 83% of Norwegian employees received timely and positive reactions when they raised concerns and 64% reported seeing improvements in their workplace after concerns were raised. In comparison, the reluctance of healthcare employees in the UK to speak up about concerns goes hand in hand with reports of staff concerns not being responded to by managers and fears about victimisation of whistleblowers. For example, a NHS Wales survey of clinical and non-clinical staff (n=10 350) shows that 54% did not report concerns due to a ‘belief that the issue won’t be taken seriously or nothing will get done’46 (p. 13). A similar trend linking organisational and managerial response to propensity for staff to report safety concerns is described by Howell et al,47 who found that hospital managers in England who fed back to staff about reported incidents and promoted change had significantly higher numbers of reports from employees.47 Hospital trusts that were deemed to have punished reporters had significantly lower reporting rates.
Model 3 demonstrates that speaking up at a rate of 39% in an institution that has inefficient and less timely responses to dealing with concerns, or speaking up at a rate of 76% in a more efficient/timely institution, can both be the best strategy for increasing the quality of patient care through the removal of bad practices. If the employees in inefficient institutions requested inquiries at 76% rather than 39%, then large-scale improvements to patient care would be significantly delayed. However, if the inefficient institution simultaneously increased their efficiency and their inquiry rate, then higher speaking-up rates would almost immediately feedback into improvements for the patients.
It is important to note that these results occur in the limit case where bad practice is never added to the institution over time—practices only ever improve. If, as in the real world, bad practices are occasionally added to the system, then this would accentuate our finding. The reason that the model’s review process eventually recovers from being inundated is that, after a time, there are not very many more requested reviews. If bad practices were continually added, then this would delay the existing reviews even more, increasing the delay in less efficient institutions. One could even imagine a world where reviews are resolved at a lower rate than bad practice is added to system, reducing the aggregate percentage of good practice. We did not add bad practices over time to this model to demonstrate that the best speaking-up strategy can be dependent on an institution’s review efficiency even in the limit case where no bad practices are added over time.
One might question the need to consider the early stages of institutional improvement, since, given enough time, it is eventually beneficial to always speak up (w=1). Why not accept that change comes at a cost, and while the institution may perform less well for a short period, in the end, transparency and whistleblowing lead to the best patient care? There is significant evidence that time may be a luxury that cannot be afforded. It is known that workers who experience delays in the process of handling and investigating concerns are often prone to absence from work due to physical and mental ill health.38 This all costs additional money that creates a feedback loop, negatively impacting patient care and staff morale.38 However, by decreasing the length of inquiries by half (from 100 to 50 rounds), it takes much less than half the time for high speaking-up rates to outperform lower rates. There is, at least in this simple model, an exponential benefit for decreasing the amount of time it takes to process inquiries.
In this model, there is always a period of time where employees not speaking up outperforms speaking-up; however, linear cuts in processing time lead to exponential cuts in the time where employees not raising concerns outperform speaking-up. As a consequence, while it might be feasible to accept the slow start to whistleblowing in an efficient institution, it might prove less feasible if inquiries take longer to process. This provides further evidence that the complex nature of institutions should be studied prior to recommending or implementing a strategy of carte blanche speaking-up.
Model 4: erroneous whistleblowing
In the previous models, the individual speaking-up always correctly diagnosed the valence of a practice. In reality, individuals are probably not perfect at uncovering poor practice. Occasionally, an employee may believe a good practice needs fixing or will not realise the faultiness of a poor practice.
Here we consider the effects of classification error in speaking-up (e), which is the probability an individual will misclassify a practice. If the individual believes a good practice is faulty, then, as previously, they will speak up with probability w. If the individual incorrectly believes, or is coerced into believing a bad practice is good, they will ignore it.
Results
Figure 4 illustrates the results when there is a 1% chance of misclassifying a practice (e=0.01). Comparing figure 4 with figure 3, it is clear that high speak-up rates take even longer to outperform lower rates. When inquiries initially require 100 rounds, a 76% whistleblowing rate does not outperform a 39% rate until round 17 945. This is in contrast to 11 693 rounds in figure 3 when practice is never misclassified, which is a 53% increase. An inquiry rate of 100% outperforms 76% at round 38 839. This is a 35% increase compared with figure 3, where it only took until round 28 690.

Patient care over 50 000 rounds when there is a chance e=0.01 that an individual misclassifies the valence of a practice. Solid lines: reviews initially take 100 rounds. Dotted lines: reviews take 50 rounds. Squares: no one ever blows the whistle, w=0. Circles, diamonds and triangles: w is 39%, 76% and 100%, respectively.
We tested a 1% level of error as the limit case, even small levels of errors create dramatic effects. If the chance for error is increased, the benefits of high levels of speaking-up decline further. At a 2% rate (e=0.02), a 76% whistleblowing rate does not outperform a 39% rate until round 25 514, a 118% increase compared with model 3. At 5%, it takes until round 63 971, which is a 447% increase.
In better functioning, efficient institutions, reporting error has less effect on the utility of whistleblowing. When the inquiry time is cut in half (dotted lines in figure 4), then high levels of speaking-up outperform low levels of speaking-up almost immediately. Despite misclassifying errors, high levels of speaking-up are quickly advantageous in more efficient institutions.
Discussion
We tested the consequences of small amounts of classification error on the value of whistleblowing. Including only a 1% chance to misclassify a practice led to a significant decline in the value of high levels of speaking-up. In this simple model, if an inefficient institution includes individuals with slightly imperfect classification ability, then shifting the whistleblowing rate from 39% to 76% could hinder patient care for an unacceptably long time. Of course, this is a simple model, and the exact interaction of error rates and review efficiency in the real world is unknown. However, if such small levels of error can generate such dramatic delays in the effectiveness of whistleblowing, then it may be unwise to advocate whistleblowing policy without holistically considering the underlying organisational topography and the introduction of practical steps to avoid or reduce misclassifying by employees (through training and education, eg, about what constitutes good and bad practices; how, when and where should concerns about poor practices be communicated; and the scope for informal and formal speaking-up approaches for various concerns).
Model 5: ineffective inquiries
Resolving concerns in a timely fashion is preferable when resources are scarce and employees are increasingly speaking-up. Time and resource pressures, allied to problematic workplace cultures may, however, undermine the accuracy of an inquiry. In all of our models up until this point, an inquiry has always shifted a bad practice into a good practice. In this model, with some probability a (accuracy), there is a chance the review erroneously deems bad practice to be acceptable. The bad practice is then placed back into the pool of practices until someone else speaks up and requests a new inquiry into the bad practice. Therefore, for each additional inquiry on the inquiry stack, there is a 0.001 chance the inquiry will be resolved incorrectly, thus accuracy is a = (0.001 * number of inquiries); we also restrict a so that it never rises above 20%.
Result
Figure 5 illustrates the results when e=0.01 and a=0.001. Comparing figure 5 with figure 4, the value of high speaking-up rates are further delayed. When inquiries initially require 100 rounds, a 76% speaking-up rate does not outperform a 39% rate until round 26 431. This is in contrast to the 17 945 rounds in figure 4 when inquiries always resolved correctly, a 47% increase in time. An inquiry rate of 100% outperforms 76% at round 48 099. This is a 24% increase compared with figure 4 where it only took until round 38 839.

Patient care over 50 000 rounds when there is a e=0.01 chance a worker misclassifies a practice, and a a=0.001 * N that inquiries will leave bad practice unchanged. Solid lines: reviews initially take 100 rounds. Dotted lines: reviews take 50 rounds. Squares: no one ever blows the whistle, w=0. Circles, diamonds and triangles: w is 39%, 76% and 100%, respectively.
As in model 4, the reduced effectiveness of whistleblowing more or less disappears if inquiries only require 50 rounds to complete (dotted lines). Even when misclassification errors (e) and inaccurate resolutions (a) are combined, efficient reviews generate an environment where increased rates of whistleblowing aids patient care.
Discussion
Here we consider the combined effect of inefficiency, misclassification errors (e) and inaccurate resolutions (a). If the accuracy of judgement is a function of the number of inquiries, then the benefits of high whistleblowing rates are delayed even further compared with model 4. However, for the most part, all of these concerns can be overcome if enough time and energy is placed into reducing the time required to resolve inquiries.
It is important to note that there is little empirical data internationally on the accuracy of reviews. However, several inquiries in many countries into serious cases of institutional shortcomings in healthcare practices have demonstrated that internal reviews of employee concerns have consistently failed to accurately resolve bad practices in a timely way, leading to the proliferation of suboptimal care to patients.23 It is also an open question how budget and resource constraints may affect the accuracy of reviews. However, as with most situations in life, it is not a huge leap to suggest that speed and pressed budgets bring costs in accuracy. As the number of inquiries increase, the speed required to resolve them efficiently may come at a cost.
We intentionally selected a small effect size (0.001) to compare the effects of inquiry errors in the limit case. While the effect size in the real world is unknown, this model demonstrates that even small correlations between the number of inquiries and the accuracy of reviews can significantly affect the utility of whistleblowing. This model lends further credence to the need for policy makers to consider the interaction between organisational topography and whistleblowing. Policy that demands speaking up without considering the organisation topography may be ineffective or, even worse, harmful.
Model 6: soft, informal speaking-up versus formal speaking-up channels
Given that we have shown that small organisational inefficiencies can dramatically impact the utility of whistleblowing practice, what is the best policy for organisations that are currently inefficient? A potential way forward is to permit the inclusion of softer mechanisms for internal adjustment of healthcare practices.2 There is evidence to suggest that in many institutions employees may speak up in softer, informal ways,40 48 such as private peer-to-peer communication.49 50 Here, we demonstrate that, when efficiency cannot be increased, less formal ways of speaking up can be advantageous.
Up until now, when a worker was presented with poor practice, they were only able to decide whether to speak up formally within their organisation. Here we introduce a softer mechanism for altering practice. Rather than formally speaking up, the employee may speak directly to a workplace colleague in an attempt to alter their behaviour, without formal internal reporting and investigation.
To model this, we add the propensity of an individual to employ softer, informal speaking-up channels, s. These informal channels may be within professional groups (eg, nurse-to-nurse) or between professional groups (nurse-to-doctor). As before, when an employee witnesses poor practice, they formally speak up with probability w. However, if the employee does not formally speak up, then they do so informally with probability s. As a result of being offered informal advice a colleague may improve their previously poor practice.
One of the concerns for permitting and promoting less formal speaking up is their lack of transparency. While internal investigations may take time, they are more transparent than permitting workers to share information and problem-solve without moderation. What happens if the advice given to the poor practising agent is not beneficial, or even worse, if it further impairs optimum practice?
To analyse the inherent risk of informal speaking up, we presume that when someone informs another of bad practice, their advice can either (1) improve, (2) worsen or (3) not affect the practice. Thus far, each good practice has increased patient care by 1, and each poor practice was represented as a 0. Now we add the ability to negatively impact patient care with a −1. If a practice is improved, then, as in the formal review, the poor practice (0 or −1) is switched to a good practice=1. If a poor practice is worsened, then the practice is switched from a 0 to a −1 (or if it is already a −1, it remains a −1). Consequently, the practice actually hinders patient care. Finally, informally speaking up can be ignored, and the practice retains its current value. We presume the chance of each output is equally probable (1/3 to improve, worsen and not affect). This is in contrast to whistleblowing which, in our model, will always result in a positive shift.
Results
Figure 6 compares model 2, where informally speaking up is not permitted (solid lines), with an institution where workers always speak up informally, s=1 (dotted lines). The chance to receive information is held static at i=1 (ie, full transparency), and the institution is accurate (a=0) and employees do not misclassify (e=0). Patient care is measured for different whistleblowing strategies. The y-axis is slightly altered compared with previous graphs. Since, in prior models, good practice=1 and bad practice=0, the fraction of good practices was the measure of patient care. Now, practices are in the set  Consequently, healthcare is measured by the average value of all practices.
Consequently, healthcare is measured by the average value of all practices.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of patient care with and without soft advice. Patient care over 50 000 rounds where reviews initially require 100 rounds. i=1, e=0, a=0. Solid lines: no soft advice, s=0 (model 2). Dotted lines: soft advice; s=1. Squares: no one ever blows the whistle, w=0. Circles, diamonds and triangles: w is 39%, 76%, and 100%, respectively.
According to figure 6, it is beneficial to promote an environment where staff speak up informally, even if this worsens the practice. If practitioners raise concerns with a 39% or 76% frequency, then informal speaking up always outperforms practitioners who do not. This is demonstrated by the fact that the dotted line is always higher than the solid line for both w=0.39 (circles) and w=0.76 (diamonds).
If workers always formally speak up (w=1), then informally speaking up to a colleague offers no benefit. This is as expected, since an employee only informally speaks-up if they do not formally speak-up, but since they always formally speak-up, the potential advantages of informal speaking-up are never witnessed. Finally, the dotted square lines illustrate that if informal speaking up is used without any formal speaking up (w=0), then practices improve, though not as much as a mixture of informal and formal speaking-up channels.
Discussion
Despite the trepidation of unmonitored and informal speaking up, in this simple model, it is almost always beneficial to permit informal channels for speaking up. However, it is important to note that in figure 6, there is an equal chance that informally speaking up will help, harm and not affect practice. If the likelihood of harmful advice is increased, then the benefits of informal speaking up may diminish or be eliminated (see online supplementary material C figure 7 and 8). This further establishes the need to consider the dynamics of the institution prior to instantiating whistleblowing policy. While it seems unlikely that professional advice would prove more likely to harm than help, such mechanisms play a significant force in selecting the best policy.
Supplementary file 3
Importantly, in figure 6, it is the mixture of formal and informal speaking-up that performs best. Whenever speaking up is not fully ubiquitous (w<1), then a combination of informal and formal speaking-up performs better than formal speaking-up in isolation. This is true over all rounds. Furthermore, this means that while formal speaking-up eventually surpasses informal speaking-up strategies, it requires more time. When the whistleblowing rate is 76% (dotted and diamond line), unconditional whistleblowing (w=1) only surpasses it when almost all practices are optimum. Thus, waiting for the benefits of formally speaking up may not be worth delaying the immediate improvement to healthcare given a mixture of softer/informal speaking-up and harder/formal speaking-up channels. If inefficiencies in processing cannot be overcome, informal speaking-up may augment formal speaking-up in generating improved patient care. This concurs with conclusions reached in a recently published large qualitative analysis of 165 employees in three NHS England organisations, which states that if organisations value less formal and softer insights as a means of sensing problems proactively, they may require approaches to accessing employee concerns that are less pervaded by formality.50
General discussion
The need for healthcare organisations to support and respond to employees who speak up about shortcomings in care has become increasingly prioritised in the UK38 and internationally.51 This has occurred as a result of evidence that suggests that organisations where employees freely speak up about concerns, and where those concerns are responded to in a supportive way, are associated with better patient outcomes52 and staff well-being.53 Organisations therefore reap significant benefits when staff are adequately listened and responded to, including: improved patient safety and patient experience, reduced costs and improved staff morale.54
In this work, we argue that subtle and small perturbations in a healthcare system may lead to significant alterations in the best policy for maximising the improvement of patient care through speaking up. By adding 10% interdependence between review processing time, we find that low speaking-up rates and a lack of transparency can, paradoxically, outperform transparency and high speaking-up rates (see model 2). Furthermore, even tiny amounts of employee error (model 4) or inaccuracy in resolving inquiries (model 5) significantly diminish the utility of speaking up. While the benefits of not speaking up do not hold in perpetuity (see models 3–5), for a given institution it may be long enough to prove salient, altering the best strategy for improving patient care. However, if inquiry time is reduced (see models 3–5), then this effect may prove small enough that the initial penalties for speaking up may be weathered and the future benefits of a transparent institution enjoyed.
We then analysed a method for increasing patient care quality when efficiency cannot be raised in isolation. We found that softer, informal mechanisms for correcting poor practices can help overcome some of the difficulties generated by institutional inefficiencies. While unmonitored advice seems risky, we showed that a mixture of informal and formal speaking-up channels leads to improved patient care. While the fidelity of formal internal institutional whistleblowing reporting and inquiries is valuable, it is cost prohibitive. Cheap, timely and informal but less transparent and possibly accurate channels for speaking-up, mixed with more accurate, formal but costly channels leads to excellent patient care.
Recently, a call was put forth to use the strengths of computational modelling to better understand the healthcare service.39 Given the speed at which modelling can diagnose potential problems with the instantiation of policy, we agree with this call and believe that modelling can act as a ‘first defence’ in trying to understand the repercussions of policy change. To our knowledge, the present work represents one of the first attempts to use computational models to better understand the effects of policy on speaking-up rates.
It is worth noting that while this work has focused on how different speaking-up rates compare with each other in a variety of environments, these models also demonstrate how much institutional nuances can alter the effectiveness of a given speaking-up rate. For instance, when the speaking-up rate is 100%, and reviews require 100 rounds, then it takes the following number of rounds to reach 95% good practice: model 1: 14 950, model 2 (10% increase): 24 280, model 4 (error rate): 29 710; model 5 (misclassification): 35 019. It is clear that the efficiency and effectiveness of an organisation can drastically alter the speed at which practice improves. For instance, if a very small amount of error and misclassification is added to the review process (model 5), this can delay the time required to reach 95% good practice by over 40% compared with the unrealistic perfect review process in model 2. Organisational efficiency and accuracy will likely play a key role in the success of speaking-up policy.
It is important, however, to discuss a major limitation in computational modelling—the simplicity of the model. No model can replicate the complexities of a working healthcare system. As the statistician George Box once said, ‘all models are wrong, but some are useful’.55 We have taken several assumptions from empirical data and shown that there is a system where concurrent review processing can impede the effectiveness of reviews so much that it is advantageous for the system to reduce the number of reviews. Does a given healthcare organisation operate in the space of this model, such that increasing reviews can impede good practice? We do not know. However, since such a space exists, we believe it is imperative to check whether existing healthcare organisations are vulnerable when enacting new policy.
Another potential limitation of this work is our use of the concurrent review process. Existing review processes are complex and often very specific to the organisation. Here, we sought to understand the consequences of trying to balance reviews concurrently. Future work could include a review process for a particular organisation that might blend the concurrent review process shown here, with both a queue-based system and a method for prioritising reviews. A model could easily be run to understand the repercussions of whistleblowing policy on the nuances of a specific review process.
It is also imperative to note that the models presented here only touch on a few mechanisms that could inhibit the utility of whistleblowing policy on patient care. We wished to demonstrate how small perturbations in institutional dynamics can lead to significant equilibrium shifts. By adding 10% delays to whistleblowing inquiries with small amounts of misclassification and inaccurate resolutions, we found that not speaking up and obfuscated information were actually beneficial to the improvement of patient care for long periods of time. We could have included even more roadblocks to resolving inquiries. For instance, given a static budget, whistleblowing reviews might actually hinder the care patients receive; if the institution is spending money on reviewing, it cannot spend money on additional patient needs. Furthermore, if a policy or guideline is created because of care failings in one institution, should other well-operating institutions be forced to comply with the new policy? The dexterity required to implement new policies may be non-trivial, potentially creating more problems than they solve. Also, this work did not consider organisational (as opposed to individual) learning. In the above models, informal and formal mechanisms for speaking up altered individual behaviour, but disseminating the need for behaviour change throughout the organisation adds another layer of complexity and viscosity. There are a number of ways in which the costs of whistleblowing may prove inhibitive, we explained three of these.
It is also known that not all organisations respond in the same way when their employees speak up about concerns. Similarly, within organisations, not all recipients of concerns are the same; some are more willing and/or able to take more effective ‘hearer’ action than others.56 We call for more research into ‘hearer courage’, to understand which managers have the courage to hear, under which circumstances, and with regard to which wrongs. Employees’ perceptions that concerns are largely ignored, or only partially acted on, has led to a lack of confidence with existing processes.2 38 40
Given that health systems internationally have experienced difficulty in responding to employees’ patient safety concerns, significantly more research and theory is needed to diagnose a holistic understanding of how the utility of whistleblowing relates to the complexities of healthcare institutions. In particular, a better understanding of the pre-existing context within which organisational initiatives and changes attempt to alter speaking-up cultures, practices and processes is needed. We recommend the use of implementation theories, such as normalisation process theory, which offers a robust conceptual framework to understand how complex interventions and their ensemble of related material and cognitive practices, gradually become normalised, or not, in specific social contexts.57 The present work calls into question the a priori belief that speaking up improves patient care and suggests that given resource constraints, whistleblowing policies should seek to understand the complex relationship between accuracy, efficiency, soft advice and the utility of speaking up. We hope continued research will aid in explaining how organisational complexities affect the utility of whistleblowing, leading to improved patient care. Furthermore, we join the recent call (see ref 39) in hoping that work such as this leads to further utilisation of the relatively untapped resource of modelling techniques into expediting and validating healthcare policy conversation.
Supplementary file 1
Supplementary file 2
References
Footnotes
Patient consent for publication Not required.
Contributors Both authors contributed to the project idea. Both authors contributed to the literature review and discussion. PR coded the simulations and wrote the result section. Both authors edited the result section. All authors read and approved the final version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The Matlab code, which was used to run the simulations, has been included in the supplementary material.