Article Text

Abstract
Objective To assess the efficacy and safety of intradialytic exercise for haemodialysis patients.
Design Systematic review and meta-analysis.
Data sources Databases, including PubMed, Embase, the Cochrane Library, China Biology Medicine and China National Knowledge Infrastructure, were screened from inception to March 2017.
Eligibility criteria Randomised controlled trials (RCTs) aimed at comparing the efficacy and safety of intradialytic exercise versus no exercise in adult patients on haemodialysis for at least 3 months. A minimum exercise programme period of 8 weeks.
Data extraction Study characteristics and study quality domains were reviewed. Studies were selected, and data extracted by two reviewers.
Data analysis The pooled risk ratios and mean differences (MDs) with 95% CIs for dichotomous data and continuous data were calculated, respectively.
Results A total of 27 RCTs involving 1215 subjects were analysed. Compared with no exercise, intradialytic exercise increased dialysis adequacy (Kt/V) (MD 0.07, 95% CI 0.01 to 0.12, p=0.02) and maximum volume of oxygen that the body can use during physical exertion peak oxygen consumption (MD 4.11, 95% CI 2.94 to 5.27, p<0.0001), alleviated depression standardised mean difference (−1.16, 95% CI −1.86 to –0.45, p=0.001) and improved physical component summary-short form-36 (SF-36) level (MD 7.72, 95% CI 1.93 to 13.51, p=0.009). Also, intradialytic exercise could significantly reduce systolic blood pressure (MD −4.87, 95% CI −9.20 to –0.55, p=0.03) as well as diastolic blood pressure (MD −4.11, 95% CI −6.50 to –1.72, p=0.0007). However, intradialytic exercise could not improve mental component summary-SF-36 level (MD 3.05, 95% CI −1.47 to 7.57, p=0.19). There was no difference in the incidence of adverse events between the intradialytic exercise and control groups.
Conclusions Intradialytic exercise resulted in benefits in terms of improving haemodialysis adequacy, exercise capacity, depression and quality of life for haemodialysis.
- haemodialysis
- intradialytic exercise
- systematic review
- meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This systematic review and meta-analysis provides evidence for the efficiency of intradialytic exercise in haemodialysis patients.
Adverse events were also evaluated to judge the safety of intradialytic exercise.
Due to the short-term follow-up in the evaluated studies, the survival rate was not studied.
Resistance exercise and a combination of aerobic and resistance exercise were not studied.
Introduction
Maintenance haemodialysis (MHD) is the major treatment option for patients with end-stage renal disease (ESRD). Due to a high prevalence of chronic kidney disease, the numbers of ESRD and MHD patients are growing rapidly.1 With progress in haemodialysis technology, the life expectancy of patients on MHD has dramatically increased. However, the overall mortality and quality of life in this population are far from satisfactory. Multiple reasons contribute to unfavourable outcomes for MHD patients, among which, sedentary behaviour is associated with increased risk of mortality among dialysis patients.2 Plagued by a variety of uncomfortable symptoms, such as fatigue, pain and depression, patients on MHD are usually less physically active. Thus, it is reasonable to encourage patients on MHD to participate in, or properly increase their, physical exercise.
Intradialytic exercise is a common recommendation given to encourage patients to be physically active.3 4 Previous studies have suggested that intradialytic exercise is effective in reducing fatigue severity, improving sleep quality,5 enhancing exercise tolerance,6 7 improving quality of life8 and even psychological status.9 Research also indicates that intradialytic exercise can increase the efficacy of dialysis,10 subsequently alleviating inflammation, improving nutrition and bone mineral density.11 Patients typically undergo two or three haemodialysis sessions a week, with each session lasting for approximately 4 hours. Since many patients maintain bed rest during haemodialysis sessions, intradialytic exercise can be a potentially useful approach to improve their health without consuming extra time during the interdialytic period. Although variety in exercise during haemodialysis sessions is limited, intradialytic exercise maximises the use of the MHD time period. Additionally, intradialytic exercise has been reported to increase patient compliance.12 However, conflicting data have been reported regarding the effects of intradialytic exercise. Furthermore, patients on MHD are usually at high risk of cardiovascular events and fractures,13 14 especially arrhythmia, acute coronary syndrome, sudden cardiac death, which render them extremely vulnerable. Thus, safety concerns may arise since unexpected injury may occur during exercise.
At present, whether or not physical exercise can ensure the safety of patients as well as improve the efficacy of haemodialysis is largely unknown. Dobsak et al 7 reported that intradialytic exercise could significantly improve Kt/V and exercise ability among dialysis patients, but not their quality of life. On the contrary, Hristea et al 8 found that intradialytic exercise did not influence patients’ Kt/V or exercise ability but significantly improved their quality of life. Regarding safety issue, previous meta-analyses15 16 showed that intradialytic exercise might not increase the risk of adverse events. However, it is noteworthy that among these meta-analyses, most of the included studies failed to address adverse events. Thus, their conclusions about the safety of intradialytic exercise need a second thought. This is further compounded by their contradictory findings regarding the efficacy of intradialytic exercise. Chung et al 15 reported that intradialytic exercise could improve haemoglobin levels but not 6 min walk distance (6MWD), while Sheng et al 16 reached quite the opposite conclusion. It seems that the risk and benefit of intradialytic exercise still remain uncertain.
In this study, we aimed to comprehensively evaluate the safety of intradialytic exercise, as well as its effects, in terms of MHD patient clinical outcomes by summarising and analysing the existing literature. Understanding the role of intradialytic exercise in MHD patients should facilitate better clinical decision-making.
Methods
Search strategy and study selection
We conducted a comprehensive medical literature search in the following electronic databases March 2017: PubMed, Embase, Cochrane Library, China Biology Medicine and China National Knowledge Infrastructure. There were no restrictions regarding language or date of publication. The search terms on PubMed included: intradialytic, haemodialysis, hemodialysis, hemofiltration, haemofiltration, dialysis, dialyses, aerobic exercise, aerobic training, resistance exercise, resistance training, strength training, physical training, physical fitness and exercise. These terms were searched both as Medical Subject Headings terms and free-text terms. The search terms were adapted for the other databases.
Two authors (JP and ZJ) screened the retrieved literature independently in two steps. First, the two authors independently screened the titles and the abstracts and excluded literature which were obviously irrelevant. Second, the full texts of potentially eligible studies were retrieved and assessed independently by the same two review authors. They included and excluded studies according to prespecified eligibility criteria: (1) Randomised controlled trials (RCTs); (2) The subjects were adult patients on MHD for at least 3 months; (3) Patients in an intervention group receiving intradialytic exercise (including resistance exercise or/and aerobic exercise). The exercise was undertaken at least twice a week, and the whole process lasted at least 8 weeks; (4) The patients in the control group received no intradialytic exercise; (5) The studies reported on the predefined outcomes we were interested in. Our primary outcomes of interest included dialysis adequacy (Kt/V), maximum volume of oxygen that the body can use during physical exertion oxygen consumption (VO2 peak), questionnaire on quality of life (short form-36, physical component summary (PCS) or mental component summary (MCS)), depression and adverse events; The secondary outcomes included a 6MWD, blood pressure at rest, haemoglobin (Hb), serum phosphorus, cholesterol and albumin levels after exercise. The studies were excluded if they had (1) patients on peritoneal dialysis or with limb disabilities; (2) implementation of physical exercise anytime other than the intradialytic duration; (3) full text was irretrievable.
Data extraction
The data extracted from the included studies were as follows: (1) Publication time, first author and country; (2) Characteristics of subjects (sample size, mean age and gender, etc) (3) Detailed information on intradialytic exercise (mode, intensity, time and frequency, etc); (4) Duration of follow-up and (5) Outcomes. Any disagreement between the review authors was resolved by the support of a third review author (SO).
Assessment of risk of bias
Assessment of risk of bias was performed independently by two review authors (JP and ZJ), with disagreements resolved by discussion. Risk of bias rating for each RCT was evaluated according to the quality domains in the Cochrane risk of bias tool and the scoring system developed by Jadad et al.17 Risk of bias for each domain was rated as high (seriously weakens confidence in the results), unclear or low (unlikely to seriously alter the results).
Data synthesis and statistical analysis
Review Manager V.5.3. (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012) was used to generate forest plots. Dichotomous data were summarised as risk ratio (RR). Continuous data were pooled as the mean difference (MD) if the outcome measuring methods and units were identical among studies; otherwise, the standardised MD (SMD), along with 95% CIs, was used. Heterogeneity among studies was evaluated by the χ2 test (assessing the p value) and calculating the I2 statistic. If the p value was less than 0.05 and I2 exceeded 50%, heterogeneity was considered substantial, and the origin of heterogeneity was analysed. For clinical heterogeneity, sensitivity analyses and subgroup analyses were performed. Alternatively, we only performed a systematic descriptive review. When heterogeneity was not substantial or obvious, the fixed effect model was used to combine the data. P<0.05 was considered statistically significant.
Patient and public involvement
There was no patient and public involvement as this was a database research study.
Results
Our initial search yielded a total of 1389 records, among which, 27 involving 1215 patients were relevant to our systematic review.6–12 18–37 The flow diagram of studies included is shown in figure 1. Of these 27 studies, three were three-arm study with comparison of no exercise, resistance exercise and aerobic exercise.

Flow diagram of studies considered for inclusion. CBM, China Biology Medicine; CNKI, China National Knowledge Infrastructure; RCT, randomised controlled trial.
Study characteristics and risk of bias
Characteristics of the included studies are shown in table 1.
Characteristics of the studies included
A total of 27 RCTs were collected and 1215 subjects were included, among which, 723 were male and 492 were female. The average age was 53. There were 16 studies that focused on aerobic exercise, 4 on resistance exercise and 7 on a combination of aerobic and resistance exercises. The detailed exercise protocols varied among studies. The follow-up duration ranged from 8 to 48 weeks. According to the modified Jadad scale, there were 13 high-quality articles (Jadad ≥4) and 14 low-quality articles (Jadad <4). The Jadad scores of studies included are listed in table 1.
Among the 27 RCTs included, 13 reported the detailed randomization methods. However, only eight trials described allocation concealment in detail. Drop-out and reasons for drop-out were described in most trials, with the exception of four. In terms of blindness, due to the nature of intervention, it was impossible to blind patients or caregivers, which might introduce selection bias, performance bias and detection bias to the results. Risk of bias ratings for each trial were assessed with the Cochrane risk of bias tool. The risk of bias summary is detailed in figure 2.

Risk of bias summary.
Evidence from randomised trials
Primary outcomes
Dialysis adequacy and VO2 peak
Nine RCTs7 8 10 11 20 21 32 34 36 involving 301 subjects reported changes in Kt/V, the measure of dialysis adequacy. Within this cohort, 153 patients participated in intradialytic exercise, while 148 patients in the control groups did not. No obvious heterogeneity was found (I2=16%, p=0.29). The analysis of data in the fixed effect model showed that intradialytic exercise could improve Kt/V (MD 0.07, 95% CI 0.01 to 0.12, p=0.02; figure 3A). The VO2 peak (metabolic equivalents (METs), equivalent to 3.5 mL/kg/min) was measured in nine RCTs.6 9 12 20 24 27 30 32 33 Among the 400 enrolled patients, 205 were assigned into the intradialytic exercise groups and 195 into the control groups. Heterogeneity was also not obvious (I2=43%, p=0.07). Compared with control subjects, the VO2 peak in patients performing intradialytic exercise increased significantly (MD 4.11, 95% CI 2.94 to 5.27, p<0.0001; figure 3B).

Forest plot: effect of intradialytic exercise on Kt/V and VO2 peak. VO2 peak, peak oxygen consumption.
Depression and quality of life
Four RCTs6 9 20 29 involving 195 patients reported on the assessment of depression levels at the baseline and endpoint. Within, 111 patients participated in intradialytic exercise, while 84 served as controls. Heterogeneity was found to be significant (I2=77%, p=0.005). The random-effects model was used to combine the data. The results showed that intradialytic exercise was able to lower the depression level (SMD −1.16, 95% CI −1.86 to –0.45; figure 4A). Two aspects of quality of life, PCS and MCS, were measured within the studies. A total of 10 trials7–9 19 22 23 26 29 31 34 that reported PCS changes were screened out. These studies involved 320 patients, 166 in the intradialytic exercise groups and 154 in the control groups. Heterogeneity was significant (I2=77%, p<0.0001). Improved PCS was observed in the intradialytic exercise group (MD 7.72, 95% CI 1.93 to 13.51, p=0.009; figure 4B). However, no significant improvement in MCS from intradialytic exercise could be discerned (MD 3.05, 95% CI −1.47 to 7.57, p=0.19; figure 4C) by analysing eight eligible RCTs.7–9 22 23 26 29 34 Additionally, significant heterogeneity was also found in this comparison test (I2=53%, p=0.04).

Forest plot: effect of intradialytic exercise on depression, PCS and MCS. MCS, mental component summary; PCS, physical component summary.
Adverse events
Only two studies28 30 reported adverse events related to intradialytic exercise. Thirteen RCTs claimed that no adverse events were observed, while 12 did not mention adverse events. Two cases of hypotension (one in the intradialytic exercise group and the other in the control group) were reported in one study. Exercise-related limb pain and minor injury were found in four cases. The prevalence of adverse events between the intradialytic exercise groups and control groups was not different: RR 4.5, 95% CI 0.55 to 36.89, p=0.16 (figure 5).

Forest plot of musculoskeletal complications.
Secondary outcomes
Twelve RCTs6 8 18 20 21 27 28 32–34 36 37 reported comparisons in Hb (g/L) levels between patients who did and did not undertake intradialytic exercise. No significant heterogeneity was found in the enrolled 459 patients (236 in the exercise groups and 223 in the control groups) (I2=0%, p=0.63). Intradialytic exercise was incapable of improving Hb levels within the fixed effect model (MD 0.01, 95% CI −0.13 to 0.16; figure 6A). In terms of albumin levels, no positive effect of intradialytic exercise on albumin levels was found (SMD 0.01, 95% CI −0.29 to 0.31, p=0.95; figure 6B) by analysis of the combined data from seven RCTs involving 175 patients.8 11 21 25 32 35 36 No significant heterogeneity was found (I2=0%, p=0.88).

Forest plot: effect of intradialytic exercise on Hb, Alb, cholesterol and phosphorus. Alb, albumin; Hb, haemoglobin.
Eight trials6 8 18 21 25 27 35 37 reported data on serum phosphorus and six11 20 25 26 32 36 reported on blood cholesterol levels. Heterogeneities were not significant in these two comparisons (I2=27%, p=0.21 and I2=0%, p=0.7, respectively). Data analyses showed that intradialytic exercise could neither lower cholesterol levels (SMD −0.13, 95% CI −0.39 to 0.13, p=0.33; figure 6C) nor decrease serum inorganic phosphorus levels (SMD −0.03, 95% CI −0.26 to 0.21; figure 6D).
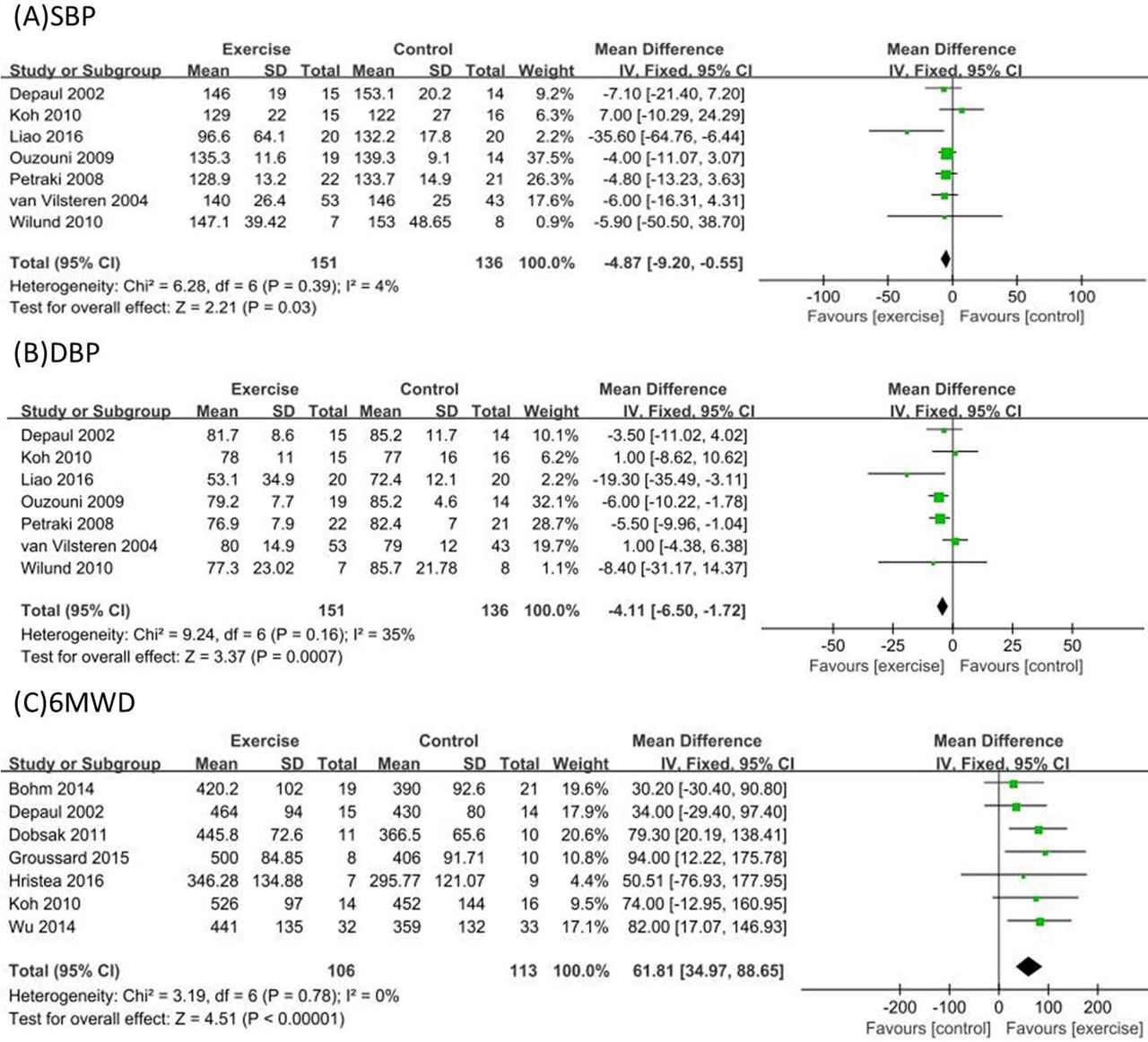
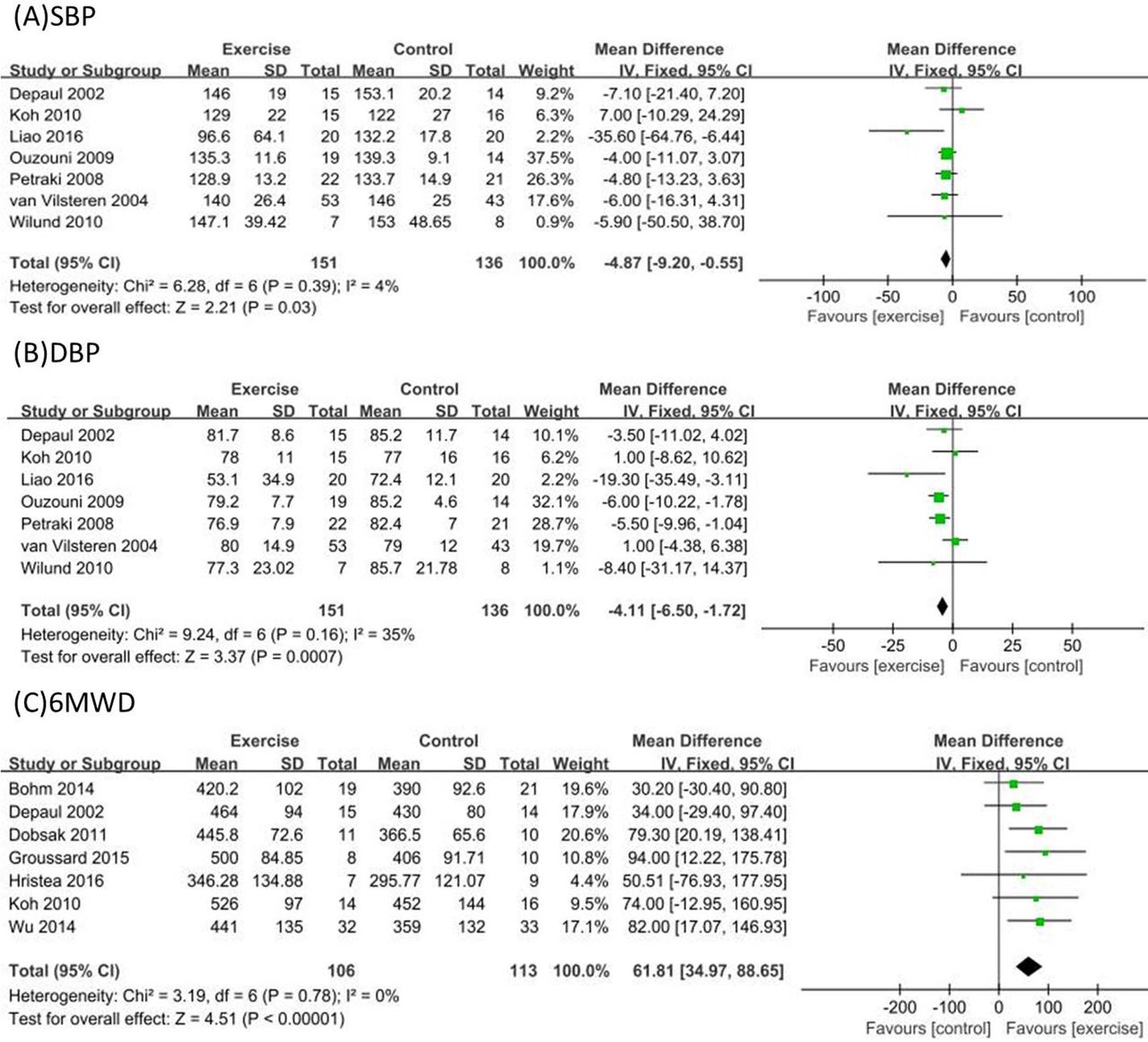
Seven trials9 11 20 23 25 28 33 compared blood pressure differences between patients who did and did not undertake intradialytic exercise. A combined analysis of 287 patients revealed that intradialytic exercise could significantly reduce systolic blood pressure (SBP) (MD −4.87 mm Hg, 95% CI −9.20 to –0.55, p=0.03) as well as diastolic blood pressure (DBP) (MD −4.11 mm Hg, 95% CI −6.50 to –1.72, p=0.0007). Heterogeneities were not significant in these two comparisons (I2=4%, p=0.39 and I2=35%, p=0.16, respectively; figure 7A,B). For assessment of physical performance, seven studies with 6MWD measurements6 7 23 28 30–32 were screened out. Due to the absence of significant heterogeneity (I2=0%, p=0.78), the fixed effect model was used for data analysis, which demonstrated that intradialytic exercise could improve physical performance (MD 61.81, 95% CI 34.97 to 88.65, p<0.0001; figure 7C).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot: effect of intradialytic exercise on SBP, DBP and 6MWD. DBP, diastolic blood pressure; SBP, systolic blood pressure; 6MWD, 6 min walk distance.
Discussion
This systematic review and meta-analysis provides positive evidence for the efficacy and safety of intradialytic exercise in MHD patients. The study included 27 RCTs involving 1215 subjects. Sixteen studies focused on aerobic exercise, four on resistance exercise and the remaining seven on a combination of aerobic and resistance exercises. The detailed exercise protocols varied among the studies.
Similar issues have been addressed by others before. Chung et al conducted a meta-analysis containing 17 RCTs with 651 patients.15 They found that intradialytic exercise could ameliorate depression, and improve quality of life, haemoglobin levels and VO2 peak among these patients; but failed to examine changes in Kt/V and blood pressure. Sheng et al 16 included 24 studies with 997 patients for meta-analysis and found that intradialytic exercise could improve Kt/V, VO2 peak, quality of life and blood pressure; but the results of physical performance (6MWD) and haemoglobin were contrary to Chung et al.
The results of this meta-analysis revealed that intradialytic exercise could improve Kt/V. This could be explained by the fact that exercise accelerated circulation and promoted the clearance of waste and excess water across the dialyser. Adequate dialysis is associated with reduced mortality. Held et al 38 found that mortality decreased by 7% with every 0.1 increase in Kt/V when Kt/V was below 1.3. Shinzato et al 39 also found that when Kt/V was lower than 1.8, the risk of all-cause death decreased with increases in Kt/V. A report by Charra et al 40 suggested that when Kt/V reached 1.67, the 5-year survival rate would be 87%, and the 20-year survival rate would be 43%. One haemodialysis study41 prospectively evaluated the impact of Kt/V on patient life expectancy. Although there was no difference in patient life expectancy between different Kt/V groups (1.25 vs 1.65), the beneficial effect of a higher dose of dialysis on survival was found in female patients in the subsequent subgroup analysis. Overall, higher Kt/V is indicative of a better prognosis. Thus, it is probable that intradialytic exercise benefits patients on MHD by improving Kt/V and increasing dialysis efficacy. However, the included RCTs did not conclude the effect of intradialytic exercise on survival rate.
Because cardiovascular complications and fatigue are common in patients with ESRD, patients on MHD usually have poor exercise capacity and are less physically active, which have been identified as independent risk factors of mortality.42 Indeed, better exercise capacity is related to lower risk of death.43 44 Our study found that intradialytic exercise increased the VO2 peak. Generally speaking, the longer the duration of exercise, the more prominent improvement is expected in VO2 peak. There are reports suggesting that for every one MET increase in VO2 peak, there will be 12% and 17% decrease in the mortality of male45 and female46 patients, respectively. Sietsema et al 47 followed up 175 patients undergoing MHD and found that VO2 peak higher than17.5 mL/kg/min was a significant predictor of survival. Consequently, we presume that intradialytic exercise may lower patient mortality through increasing VO2 peak. However, existing studies have not addressed this relationship yet. Notably, the VO2 peak measurement time points varied across the component studies, and these differences may result in clinical heterogeneity.
In terms of quality of life assessment, intradialytic exercise improved PCS levels, but not MCS levels. Depression is the most common mental disorder in the MHD population.48 Indeed, depression is more prevalent in the MHD population than the general population or even the chronic disease population,49 and unfortunately, depression increases the mortality of patients on MHD.50 51 We found that intradialytic exercise could improve depression severity. Unfortunately, there are few clinical trials (only four) focusing on the outcome of depression with a small sample size and diverse depression rating scales, such as Self-rating Depression Scale, Beck Depression Inventory, and the Hospital Anxiety and Depression Scale. This further increases the heterogeneity among studies. Confirmation of the association between intradialytic exercise and depression needs will require further investigation in high-quality randomised, controlled clinical trials.
Our study revealed a positive influence of intradialytic exercise on lowering blood pressure. Intradialytic exercise could reduce both SBP and DBP, without increasing the incidence of intradialytic hypotension. As a common complication, hypertension is closely related to increased cardiovascular events and mortality in MHD patients. A previous meta-analysis of five studies revealed that anti-hypertensive therapy might reduce all-cause mortality among the MHD population.52 Heerspink et al reported that the risk of cardiovascular disease reduced by 29%, cardiovascular mortality reduced by 29% and all-cause mortality reduced by 20% when blood pressure was reduced by 4.5/2.3 mm Hg.53
Adverse events were also evaluated to examine the safety of intradialytic exercise. The most common adverse events were hypotension and exercise-related injury. According to our results, only four patients suffered from limb pain and minor injury, and only one suffered from hypotension out of the total of 1215 cases analysed. It seemed that intradialytic exercise was unlikely to be associated with a high incidence of adverse events. Therefore, intradialytic exercise may be advantageous for patients undergoing MHD, with low associated risk. However, 12 of the trials reviewed did not report an incidence of adverse events, though under-reporting of exercise-related adverse events among MHD patients may be likely. Thus, to ensure patient safety, we recommend that implementation of intradialytic exercise be under the supervision of clinicians. In addition, our findings indicate that intradialytic exercise increases haemodialysis efficacy, alleviates depression and enhances exercise capacity among MHD patients. Furthermore, intradialytic exercise can lower blood pressure. However, we found no correlation between intradialytic exercise and albumin or Hb levels. Recently, a meta-analysis published by Young et al suggested that intradialytic exercise failed to improve VO2 and blood pressure; these findings were inconsistent with ours.54 This is possibly because our study enrolled studies involving aerobic exercise, resistance exercise or their combination; while the study by Young et al only included studies that were focused on aerobic exercise.
In this meta-analysis, we found that the method, the duration and the intensity of exercise differed between studies. Only a few studies examined the clinical influences of different exercise methods on the outcomes of patients. Afshar et al 36 found that compared with resistance training, aerobic exercise effectively decreased serum creatinine and high-sensitivity C reactive protein. Segura-Ortí et al 55 reported that resistance training did not differ from aerobic exercise in terms of their influences on physical performance. A study by Sheng et al 16 demonstrated that combining aerobic and resistance training could enhance the VO2 peak more efficiently than aerobic exercise alone, although significant VO2 peak elevation was only observed after the intradialytic exercise programme was implemented for more than 6 months. There is still a lack of evidence regarding the clinical impact of exercise intensity in terms of patient outcome. Due to the heterogeneity of exercise methods in the studies reviewed, we did not perform subgroup analyses. Further investigations are warranted to determine the optimal exercise method through which satisfactory outcomes can be achieved.
There are several limitations to this study. First, due to the short-term follow-up in the evaluated studies, the survival rate was not a typical endpoint for the included RCTs. Additionally, surrogate biomarkers can only reveal the benefit of intervention in a limited manner. Second, there was significant clinical heterogeneity in the exercise protocols (type, strength and duration of exercise), which might introduce bias to the results. Besides, the follow-up duration varied from 8 to 48 weeks. The variation in follow-up duration added to the interstudy clinical heterogeneity. Third, due to the heterogeneity of the exercise methods used in the included studies, we did not perform subgroup analyses. Thus, it is impossible for us to evaluate the effect of different types of exercise.
In conclusion, intradialytic exercise could improve Kt/V, exercise capacity, depression and quality of life as well as lower blood pressure among MHD patients. Intradialytic exercise might not increase the incidence of adverse events.
References
Footnotes
Patient consent for publication Not required.
JP and ZJ contributed equally.
Contributors SO and JP acted as guarantor for the validity of the study report. Study concept and design: JP and ZJ. Experiments were performed by: JP, ZJ, WW, LL and LZ. Analysis and interpretation of data: LL, YL and QL. Drafting of the manuscript: SO and JP. Critical revision of the manuscript for important intellectual content: SO.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.