Article Text

Abstract
Objectives Cancer survival and stage of disease at diagnosis and treatment vary widely across Europe. These differences may be partly due to variations in access to investigations and specialists. However, evidence to explain how different national health systems influence primary care practitioners’ (PCPs’) referral decisions is lacking.
This study analyses health system factors potentially influencing PCPs’ referral decision-making when consulting with patients who may have cancer, and how these vary between European countries.
Design Based on a content-validity consensus, a list of 45 items relating to a PCP’s decisions to refer patients with potential cancer symptoms for further investigation was reduced to 20 items. An online questionnaire with the 20 items was answered by PCPs on a five-point Likert scale, indicating how much each item affected their own decision-making in patients that could have cancer. An exploratory factor analysis identified the factors underlying PCPs’ referral decision-making.
Setting A primary care study; 25 participating centres in 20 European countries.
Participants 1830 PCPs completed the survey. The median response rate for participating centres was 20.7%.
Outcome measures The factors derived from items related to PCPs’ referral decision-making. Mean factor scores were produced for each country, allowing comparisons.
Results Factor analysis identified five underlying factors: PCPs’ ability to refer; degree of direct patient access to secondary care; PCPs’ perceptions of being under pressure; expectations of PCPs’ role; and extent to which PCPs believe that quality comes before cost in their health systems. These accounted for 47.4% of the observed variance between individual responses.
Conclusions Five healthcare system factors influencing PCPs’ referral decision-making in 20 European countries were identified. The factors varied considerably between European countries. Knowledge of these factors could assist development of health service policies to produce better cancer outcomes, and inform future research to compare national cancer diagnostic pathways and outcomes.
- delivery of health care
- primary health care
- general practitioners
- cancer
- decision making
- consultation and referral
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- delivery of health care
- primary health care
- general practitioners
- cancer
- decision making
- consultation and referral
Strengths and limitations of this study
The questionnaire was developed using content validity reduction and factor analysis of a consensus item pool, and therefore grounded in primary care practitioners' (PCPs’) clinical experience.
PCPs were recruited from 20 European countries, 4 countries from each of the Central, Eastern, Northern, Southern and Western European geographical areas.
Most samples were taken from each local lead’s own locality, and these may not have been representative of their nations as a whole.
The response rate was low but comparable to that of other equivalent surveys of primary care doctors.
Background
There is wide variation in cancer survival rates across Europe.1 Data from the fifth cycle of the European Cancer Registry-based Study on Survival and Care of Cancer Patients (EUROCARE-5) show that the 1-year relative survival rate for all cancer sites varies from 58.2% to 81.1% between countries1 (table 1). Although 1-year relative survival can be affected by differences in registration (eg, completeness and use of death certificates), and lead-time and overdiagnosis biases,2 3 it is generally taken to be an indicator of more advanced disease at diagnosis.4 5 Survival differences in the subsequent 4-year period (known as ‘5|1-year conditional survival’) are narrower, suggesting that earlier diagnosis could reduce the 1-year relative survival gap.6 This is supported by increasing evidence that longer time to diagnosis and treatment may adversely affect mortality.7–13 While recent overall cancer survival trends show improvements,14 there is little narrowing in the between-country survival differences.15
EUROCARE-5 1-year relative and 5|1-year conditional cancer survival rates for European countries,1 with ranks given
The challenge of where and how to achieve more timely diagnosis is considerable.16 A general practitioner (GP) will see only a small number of new cancers each year, for example, a GP in the United Kingdom (UK) will on average have a new cancer diagnosed in one of his or her patients each month.17 The majority of cancers are identified because the patient has been experiencing symptoms. However, most patients present with evolving and undifferentiated symptoms that are much more likely to be interpreted as something other than cancer.16
GP gatekeeping, in which patients’ access to specialists, hospital care and diagnostic tests needs to be authorised by GPs,18 is the cornerstone of many European medical systems.19 There is evidence that stronger gatekeeper systems are linked with lower 1-year relative cancer survival than systems without such gatekeeper functions.20 This may be because gatekeeping systems can impose cost and resource decisions which impede early referral for investigation.21 However, there are wide variations in the degree of gatekeeping between countries, with no simple binary model as to whether or not a country has a ‘GP-as-gatekeeper’ system, and a European study found no link between a higher probability of initial consultation with a GP and poorer cancer survival.22
The way in which different healthcare systems support primary care in cancer diagnosis by quick and easy access to investigations may also be a factor in timeliness of cancer diagnosis.23 It has been suggested that GPs need faster routes to diagnostic tests and/or specialist opinion for all patients with a suspicious symptom, above a certain threshold.21 In the UK, use of an urgent cancer referral pathway has been found to be associated with reduced mortality24 and a reduction in the proportion of cancers diagnosed through emergency presentations.25 An International Cancer Benchmarking Partnership (ICBP) study demonstrated a correlation between the readiness of primary care practitioners (PCPs) to investigate suspicious symptoms and cancer survival rates.26 No consistent associations were found between how likely practitioners were to investigate and PCP demographics, practice or health system variables. However, there was no exploration of how individual doctors felt that health system factors affected their decision-making.
The Örenäs Research Group is a European group of primary care researchers that studies the primary care factors that relate to cancer survival. It has identified a large variety of non-clinical factors that are likely to have a considerable impact on PCPs’ referral decision-making.27 These include levels of gatekeeping responsibility, funding systems, access to investigations and relationships with specialist colleagues. However, there has been little research done to explain how these vary between countries.16
This study investigated the health system factors potentially influencing European PCPs’ decision-making with regard to investigating patients who may have cancer, and how these vary between European countries.
Methods and design
Design
We performed an international online survey of PCPs in 20 European countries between November 2015 and December 2016. Some of the methodology described here reproduces information already reported in our published protocol paper.28
Development of the questionnaire
Following a literature review, 7 Örenäs Research Group investigators developed and agreed by consensus a list of 45 items, each relating to predefined aspects/concepts that may affect a PCP’s decision to refer patients with potential cancer symptoms for further investigation. A questionnaire based on these items was piloted by 16 members of the Örenäs Research Group to assess content validity. Six of the items were removed due to low content validity. An English-language questionnaire with the remaining 39 items was piloted by 49 PCPs in 16 Örenäs Research Group member countries (table 2). Nineteen items were found to show little or no variation between countries and were removed from the questionnaire, leaving 20 items.
Results of questionnaire pilot
Örenäs Research Group leads arranged for translations of the questionnaire into their local languages where these were not English, a total of 19 translations from the original English. Translation and validation were done in a standardised way29: native speakers of the local languages who were fluent in English and were medically qualified did the ‘forward’ translations. ‘Backward’ translations into English were then made by translators who were fluent in both English and their local language. The forward translations were then compared with the backward ones, to assess semantic and conceptual equivalence.30 Discrepancies between the forward and backward translations were resolved by discussion with the translators, following which the final translation was agreed on. Finally, in each country the corrected versions were piloted in a small sample of PCPs to evaluate the instructions, response format and the items for clarity and to ensure cultural adaptation.30
The questionnaire and distribution
The final questionnaire sought demographic information (table 3) and presented the 20 health system factor items (listed in table 4). Respondents were asked to rate how much they agreed with each item in relation to their referral decision-making for patients who could have cancer. A five-point Likert rating scale was provided for participants, with response options ranging from ‘strongly disagree’ to ‘strongly agree’. The questionnaires were put online using SurveyMonkey. Online methodology was used to aid the logistics of survey administration; online surveys have been successfully used in research involving cancer care professionals.31
Number of respondents per country and demographic distributions.
Mean national Likert-scale values for each of the 20 questions
Study population
The study was conducted in 25 Örenäs Research Group centres in 20 countries across Europe: Bulgaria, Croatia, Denmark, England, Finland, France, Germany, Greece, Israel, Italy, Netherlands, Norway, Poland, Portugal, Romania, Scotland, Slovenia, Spain, Sweden and Switzerland. Local study leads were asked to either gain ethical approval or obtain a statement that formal ethical approval was not needed in their jurisdiction (see online supplementary file).
Supplementary file 1
Subjects were eligible for the survey if they were doctors working mainly in primary care. These doctors, here referred to collectively as ‘PCPs’, included GPs and other doctors who had had specialist training but worked in the community and could be accessed directly by patients without referral.
Sample size
A total sample size of 1000 or more responses was calculated to be sufficient to obtain stable factor estimates within the exploratory factor analysis,32 based on each jurisdiction recruiting at least 50 respondents. This provided a 95% CI of at most ±14%.
Recruitment of participants
Each Örenäs Research Group local lead was asked to email an invitation to take part in the survey to the PCPs in their local health district, and to recruit at least 50 participants. In six countries (Denmark, Norway, Portugal, Romania, Slovenia, Sweden), the invitation was distributed to a national sample. Any local leads who had difficulty in achieving the required sample sizes were asked to increase the number of responses by using snowballing.33 Consent was implied by agreeing to take part in the survey. All data were collected anonymously.
Statistical analysis
The demographic characteristics of the respondents were explored using descriptive statistics. Likert scale responses were converted to numerical scores (‘strongly disagree’=1, ‘strongly agree’=5). An exploratory factor analysis was undertaken on these responses, to identify underlying factors and to test the predefined constructs.
We used a principal components method,34 with a direct oblimin rotation to allow for correlated factors. The number of components was defined by inspection of the scree plot and the Kaiser criterion (eigenvalue ≥1). Between-country variation in these factors was then examined and presented as means with 95% CIs. We made a sensitivity analysis with weighting of the responses to adjust for the differing numbers of respondents per country. Calculations were performed using IBM SPSS V.22.
Patient and public involvement
There was no patient or public involvement in this study.
Results
A total of 1830 PCPs completed the questionnaire. All participating centres received at least 50 responses, with a median of 72 respondents per centre. PCPs’ demographic distributions are shown in table 3. The median response rate per country was 20.8% (range 6.7%–57.8%).
The mean national Likert-scale values for each of the 20 questions are given in table 4.
The factor loadings for each of the 20 items are shown in table 5. The factor analysis identified five factors which accounted for 47.4% of the variance of individual responses. The factor means for each participating country and their 95% CIs are given in table 6.
Health system items and their factor analysis loadings The highest-scoring component for each item is italicised.
Factor means for each country with 95% CIs
Factor 1: primary care practitioners’ ability to refer
This factor contained six items. A higher score on this factor indicated lower barriers to specialist referral, more time during the consultation to consider whether the patient needs a referral and absence of criticism from colleagues over referrals that were perceived to be unnecessary. This factor explained 15.5% of the variance of individual responses. A comparison of national scores for factor 1 is shown in figure 1.

Comparison of national scores for factor 1: primary care practitioner’s ability to refer. A higher score indicated lower barriers to specialist referral.
Factor 2: degree of direct patient access to secondary care
This factor contained six items. A higher score for this factor was linked with items relating to direct patient access to secondary care: the absence of a GP gatekeeping role, with higher financial and geographical barriers to healthcare for some patients, and in some cases the presence of a quota for diagnostic tests. Higher scores for this factor were also linked with less likelihood of having a fast-track specialist appointment system for patients with suspected cancer. Factor 2 explained 10.8% of the variance of individual responses, and the comparison of national scores for this factor is shown in figure 2.
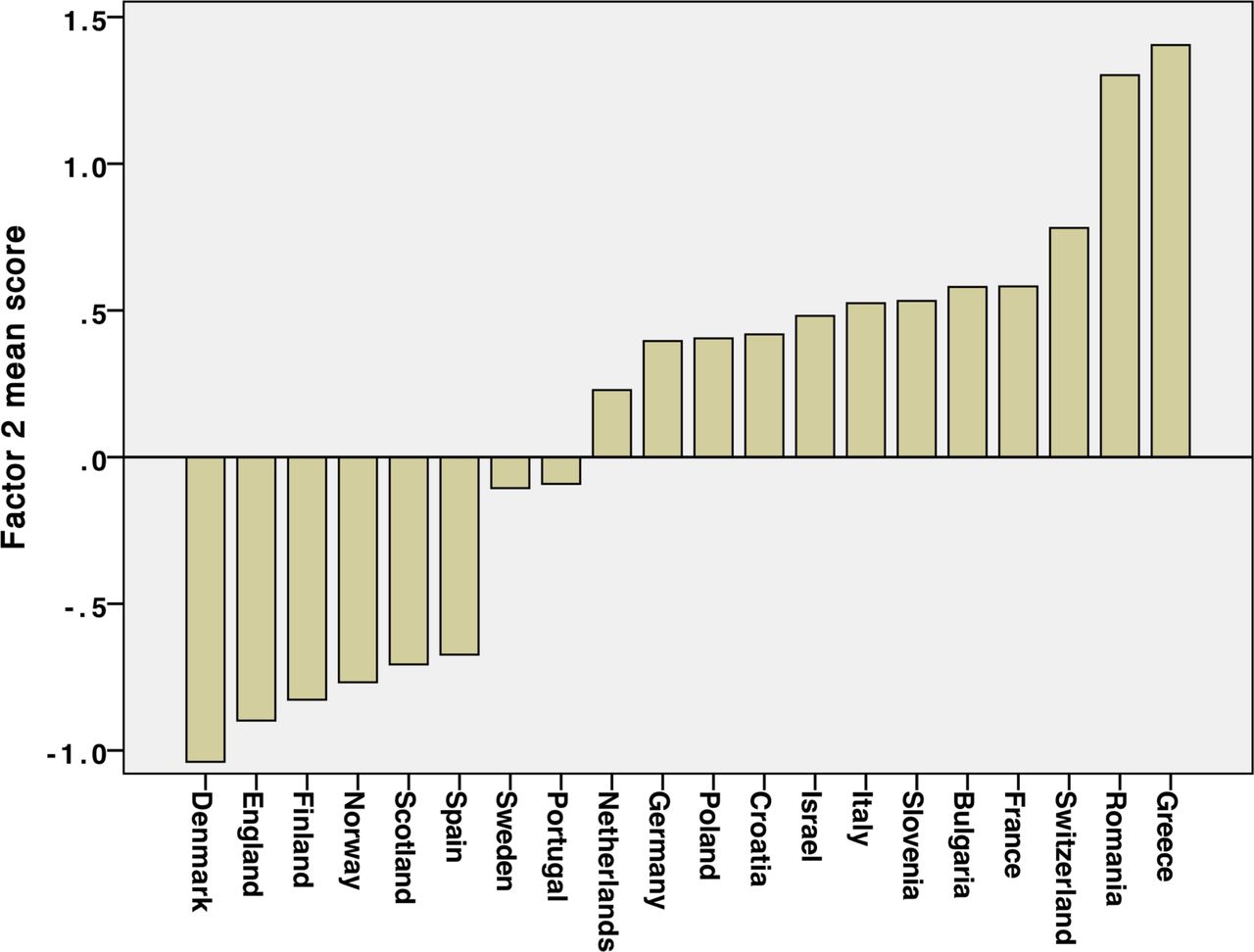
Comparison of national scores for factor 2: degree of direct patient access to secondary care. A higher score was linked with the absence of a general practitioner gate-keeping role, but higher financial and geographical barriers to healthcare for some patients.
Factor 3: primary care practitioners’ perceptions of being under pressure
This factor contained four items. A higher score was linked with perceptions of pressure on the PCP from a high workload, as well as demands from patients, the public and the health system. It explained 7.6% of the variance of individual responses. A comparison of national scores for factor 3 is shown in figure 3.

Comparison of national scores for factor 3: pressure on primary care practitioners from outside. A higher score was linked with perceptions of higher pressure on the primary care practitioner.
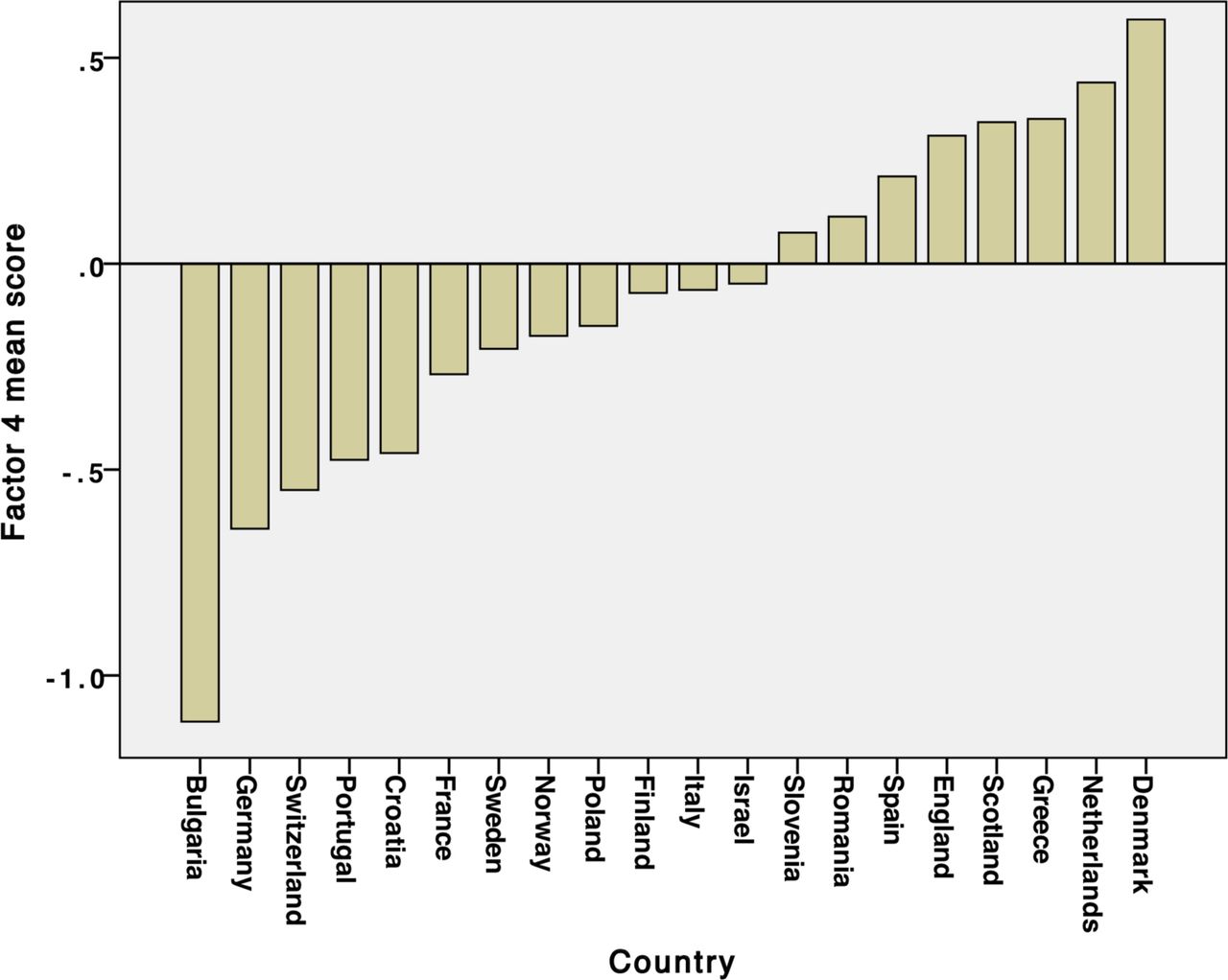
Factor 4: expectations of the primary care practitioners’ role
This factor contained two items. A higher score for this factor was associated with higher expectations of PCP-centred care, and the presence of guidelines to support PCP decision-making. It explained 6.7% of the variance of individual responses, and a comparison of national scores for this factor is shown in figure 4.

Comparison of national scores for factor 4: expectations of the primary care practitioner’s (PCPs') role. A higher score was associated with higher expectations of PCP-centred care, and the presence of guidelines to support PCP decision-making.
Factor 5: quality before cost
This factor contained two items. A higher score was linked with PCP perceptions that in their systems high quality care for patients was more important than costs, and that financial aspects had less effect on their referral decision-making. This factor explained 6.4% of the variance of individual responses. A comparison of national scores for factor 5 is shown in figure 5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of national scores for factor 5: quality before cost. A higher score was linked with primary care practitioner perceptions that in their systems high quality care for patients was more important than costs.
Sensitivity analysis
In a sensitivity analysis with weighting of the responses to adjust for the differing numbers of respondents per country, only one statement moved to a different factor: the statement "In my practice, patients often have to travel a long way to see a specialist" moved from factor 2 to factor 4.
Discussion
Principal findings
Based on a content validity process, a 45-item pool on referral decision-making for patients who could have cancer was reduced to a 20-item questionnaire. From the responses of 1830 PCPs, from 25 primary care centres in 20 European countries, 5 key factors were identified: PCPs’ ability to refer; degree of direct patient access to secondary care; PCP perceptions of being under pressure; expectations of the PCPs’ role; and the extent to which PCPs believe that, in their systems, quality comes before cost. The factors showed significant variation between the participant countries.
Interpretation of the results
Based on the content validity and the significant variation between countries, the survey can be regarded as relevant for studying aspects of PCPs’ perceptions of what affects their referral and investigation of patients with symptoms that could be due to cancer. Thus, the developed questionnaire could be used in further research to evaluate associations with cancer outcomes, and could also be used to evaluate changes in healthcare systems regarding referring patients who could have cancer.
Factor 1. PCPs’ ability to refer: the variation in PCPs’ ability to refer was linked to structural differences like barriers to specialist referrals (including waiting times), the degree of criticism of PCPs relating to their referrals, the quality of relationships between PCPs and specialists and the length of the PCPs’ consultations with patients. This was the most important factor, carrying most of the explained variation, and consequently it appears to be particularly important in explaining between-country differences in primary care cancer diagnosis.
Factor 2. Degree of direct patient access to secondary care: this important factor was related to the extent to which GPs were gatekeepers and to which public systems provided universal access to healthcare, whether self-referral to specialists was possible outside the public health system, patients’ ability to travel to and fund specialist consultations and whether fast-track referral systems were in place for patients with suspected cancer.
Factor 3. PCPs’ perceptions of being under pressure: variations in PCPs' perceptions of being under pressure were linked with PCP workloads, patient expectations and their level of trust in their doctors and the extent to which health systems expected PCPs to refer patients.
Factor 4. Expectations of the PCPs’ role: differing expectations of the PCPs’ role were related to whether there had been a shift of work and responsibility between secondary and primary care, and the extent to which patient care was from specialists rather than from PCPs.
Factor 5. Quality before cost: the variation in the extent to which PCPs perceived the balance between quality of care and cost was linked with how much PCPs themselves were directly affected by considerations of cost.
Strengths and weaknesses of the study
There were participating centres in four countries from each of the Central, Eastern, Northern, Southern and Western European geographical areas, providing variation in geography, health systems and levels of healthcare spending. It included the views of PCPs who are not usually involved in research. The questionnaire was carefully developed and piloted by GPs and other PCPs, and therefore grounded in their clinical experience. The sensitivity analysis suggested that the factor structure is robust and not driven by countries with larger numbers of respondents.
While low survey response rates are common in primary care35 and are known to vary between countries, the response rates in our study were comparable to those of a recent ICBP survey, in which response rates varied from 5.5% to 45.6%.26 As the survey was anonymous, we have no data on non-responders. It is possible that the PCPs with the most interest in this subject were the most likely to respond. However, while this selection bias may have affected the factor loadings, it is unlikely to have changed the factor structure itself.
While the demographic data that we collected included the gender of participants and the number of years that they had been in practice, we have found no equivalent data on national PCP populations that would allow us to assess how representative our samples were.
Most samples were taken from each local lead’s own locality, and these may not have been representative of their nations as a whole.36 While this makes it difficult to generalise the findings to each country, the variation between countries is relevant and valid. The recruitment method used in this study resulted in variable response rates, leading to a risk of non-response bias and loss of power.35 However, the goal of 50 survey participants per centre and >1000 respondents in total was achieved.
Participants’ responses may have been influenced by previous questions, and there may have been country-level differences in response styles, for instance, choosing or avoiding the ‘extreme’ options on the scale.37 As the translation also included a cultural adaptation we believe this bias was minimised, and the differences between countries cannot simply be explained by differences in response styles.
The five factors accounted for 47.4% of the variance in PCPs’ responses, and it is acceptable to consider a solution that accounts for 60% or less of the total variance as satisfactory.38 Two of the factors only included two items each, which makes them vulnerable to missing responses and stochastic variation.
Comparison with other studies
To our knowledge, this is the first study that has been designed to identify the factors underlying PCPs’ referral decision-making, and provide international comparisons of the extent to which PCPs themselves perceive these as important. An ICBP narrative review compared the characteristics of healthcare systems of six countries (Australia, Canada, Denmark, Norway, Sweden and the UK), aiming to identify characteristics that could possibly modify the diagnostic pathway.39 However, unlike our study, it only explored the systems of relatively wealthy countries, and it did not examine PCPs’ own perceptions of how their systems affected their decision-making. Our finding that PCPs in different European countries perceive different levels of access to investigations and specialist opinions may be relevant to the finding of varying referral delays in three European countries (Scotland, the Netherlands and Sweden).40
Possible implications for clinicians and policymakers
Five health system factors were able to explain nearly half of the variation in the PCPs’ responses to the items. This indicates that a relatively large part of the variation may be explained by differences between the health systems. Our study indicates the policy domains where countries might be able to modify their systems to better support their GPs and other PCPs in the timely referral and investigation of patients who could have cancer.
The most important of these factors were the ease of PCPs’ ability to refer, and the degree of direct patient access to secondary care. These factors are key in supporting earlier and expedited cancer diagnosis and may thus be linked with cancer outcomes. It therefore seems plausible that some countries could improve their cancer outcomes by providing better access to investigations and secondary care when cancer is suspected.
Unanswered questions and future research
The five factors and their related scores should be compared with national cancer outcomes. These outcomes could include mortality, stage distribution and patient evaluations. An additional area of study could be to relate the factors and scores to national health system costs.
Conclusions
This research has developed a 20-item questionnaire with good content and construct validity, and has identified five factors that PCPs perceive to affect their referral decision-making in patients that could have cancer. These appear to vary depending on the different European models of primary care. This understanding of the interaction between health system variables and PCP decision-making can help in an exploration of the differences in national cancer diagnostic pathways and cancer outcomes, and could help to inform health service policy and research towards better cancer outcomes.
Acknowledgments
The authors would like to thank all the PCPs who piloted the questionnaire and those who completed the survey. They would also like to thank the European GP Research Network for its support. They are grateful to Professor Barbara Silverman and Professor Lital Keinan for the data on cancer survival rates in Israel.
References
Footnotes
Contributors IA-A, JA, KB, MB, NB, EC, G-JD, ME, GF, SGB, MH, RH, EJ, TK, MM-C, PM, ALN, DP, MPS, JS-P, AS, ES, SS, GT, HT, PV and BW participated in the study design. All authors except GT were involved in the data collection. All authors contributed to the writing and to the review of the manuscript and approved the final version. MH had overall responsibility for the study design, recruitment of local leads, analysis of data and interpretation of results. GT advised on the study design and the statistical analysis.
Funding ALN is supported by the National Institute for Health Research (NIHR) Imperial Patient Safety Translation Research Centre, with infrastructure support provided by the NIHR Imperial Biomedical Research Centre (BRC).
Competing interests None declared.
Patient consent Not required.
Ethics approval University of Bath Research Ethics Approval Committee for Health.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The Örenäs survey data used in this study is available at https://doi.org/10.15125/BATH-00486.