Article Text

Abstract
Objective To better understand, based on patient partners’ experiences, benefits and risks in patient partner–researcher relationships in a health research setting.
Design Qualitative interviews with thematic analysis informed by a relational ethics lens.
Setting A multidisciplinary health research centre in Vancouver, Canada. This study was codeveloped by patient partners and researchers at the centre.
Participants 22 people living with arthritis, with experience as members of a patient advisory board at the research centre from 1 month to 10 years.
Results We identified three main themes: (1) Being Heard: Participants had experienced uncomfortable emotions (eg, feelings of insecurity) in their relationships with researchers. The discomfort, however, was minimised by the demonstration of mutual respect in their interactions. Specifically, participants valued environments without a hierarchy between patient partners and researchers, where contributions of each party were considered equally important, and where patients’ voices were heard; (2) Cobuilding social relations: Participants valued building social relations with researchers beyond their expected interactions as partners in research and (3) Adding another spinning plate to an already busy life: Participants valued relationships with researchers who had cocreated environments that minimised the risks of physical and emotional impacts (eg, fatigue, stress, guilt) on them while juggling multiple obligations, priorities and their health.
Conclusions Findings provide valuable insights to guide relationship building between patient partners and researchers. Informed by a relational ethics lens, these findings are a critical step in supporting an ethically sound practice of patient engagement in research that prioritises patients’ perspectives.
- qualitative research
- ethics (see medical ethics)
- patient engagement in research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study was initiated, codesigned and coconducted by researchers and patient partners.
Rich data were generated from a sample of participants with varying levels of experience in building relationships with researchers as patient partners in research.
Our findings may be limited to address issues of diversity in patient engagement in research. For example, the majority of participants were women, and thus, findings may not represent experiences of male patient partners in research.
Introduction
Building genuine, reciprocal relationships between patient partners and researchers is an important component in optimising patient engagement in research.1–4 As a practice, patient engagement in research encompasses complex and evolving processes through which patient partners are meaningfully and actively involved in governance, priority setting, conducting research and/or knowledge translation.5 The term ‘patient partner’ broadly describes individuals with at least one health condition, informal caregivers (eg, family members) or members of the public (who use health services, eg, annual physical examination; vaccination), who engage in research activities with researchers. Levels of engagement exist on spectrums, varying from patient partners being informed about decisions or patients providing feedback as advisers to collaboration or shared leadership with researchers.6–9 In recent decades, this engagement has been widely supported as a means to enhance the relevance of research, with the ultimate aim of supporting translation of research into improved health outcomes and services.5 6 10–12
Without building genuine, reciprocal relationships, engagement between patient partners and researchers is at risk of tokenism (ie, superficial efforts, in order to give a mere appearance of inclusion) and, ultimately, failure to realise potential.3 Genuine, reciprocal relationships are characterised by the presence of a sense of trust, full disclosure, mutual benefit and respect, and understanding of each other’s needs, capacities and goals.1 3 13 Several accounts indicate that patient partners experience benefits and risks in the process of relationship building with researchers.1 3 4 14–20 In a qualitative study of 64 patient partners, Cotterell et al found that interactions with professionals (including researchers) could be distressing for patient partners in instances when scientific knowledge that had negative implications for the prognosis of their disease was shared.15 Schipper et al also reported that while a patient partner experienced feelings of fear, tension and uncertainty in relationship building with researchers, the patient partner also valued having an increased sense of equality in her relationships with researchers.4 Little research, however, has systematically examined benefits and risks encountered in relationships between patient partners and researchers, from patients’ perspectives.
We apply a relational ethics lens in order to stress moral significance in the relationships that patient partners and researchers experience as they engage.21–25 From this particular relational ethics lens, an aspect of acting ethically demands attentiveness and responsiveness to benefits and risks that can be experienced in our relationships with each other. It requires careful consideration for the quality of our contact with each other, and asks for fitting responses to everyday ethical questions, such as ‘Is that the way I should treat someone else? Is that the way someone else should treat me?’ Relational ethics stems from a dissatisfaction with traditional bioethics principles (ie, autonomy, beneficence, maleficence, justice) that appear distanced or disinterested in the ordinary, everyday ethical issues encountered in healthcare practice.23 While drawing on these traditional principles, the relational ethics lens broadly expands in scope to direct attention to the contextual details of personal experience or situations within which these ethical principles are exercised in real life. It has been used previously to bring attention to ethically important moments experienced within relational contexts involving researchers and patients in healthcare and health research practices.22 23 It also highlights key ethical aspects in relationships (eg, respect, embodiment and interdependency), which are of particular relevance in the context of patient partner–researcher relationships.21–23 Respect can underscore issues of power and vulnerability. In the context of a patient partner–researcher relationship, respect may involve safeguarding confidential information revealed to each other during meetings.10 16 Embodiment can highlight the role that emotions play in the process of relationship building. For example, embodiment may highlight expectations among members of a research team that only patient partners should share their personal history and subjective feelings in the research process, while researchers are expected to remain objective.4 Interdependency can recognise that each individual is situated within a community, connected with other individuals and institutions that influence their choices. It may highlight, for example, patient partners’ concerns that having relationships with researchers who are also their clinicians may lead to other patients assuming they receive preferential care.16 Drawing on these aspects of the relational ethics lens, this study aimed to examine benefits and risks in patient partner–researcher relationships, based on patient partners’ experiences.
Methods
Patient and public involvement
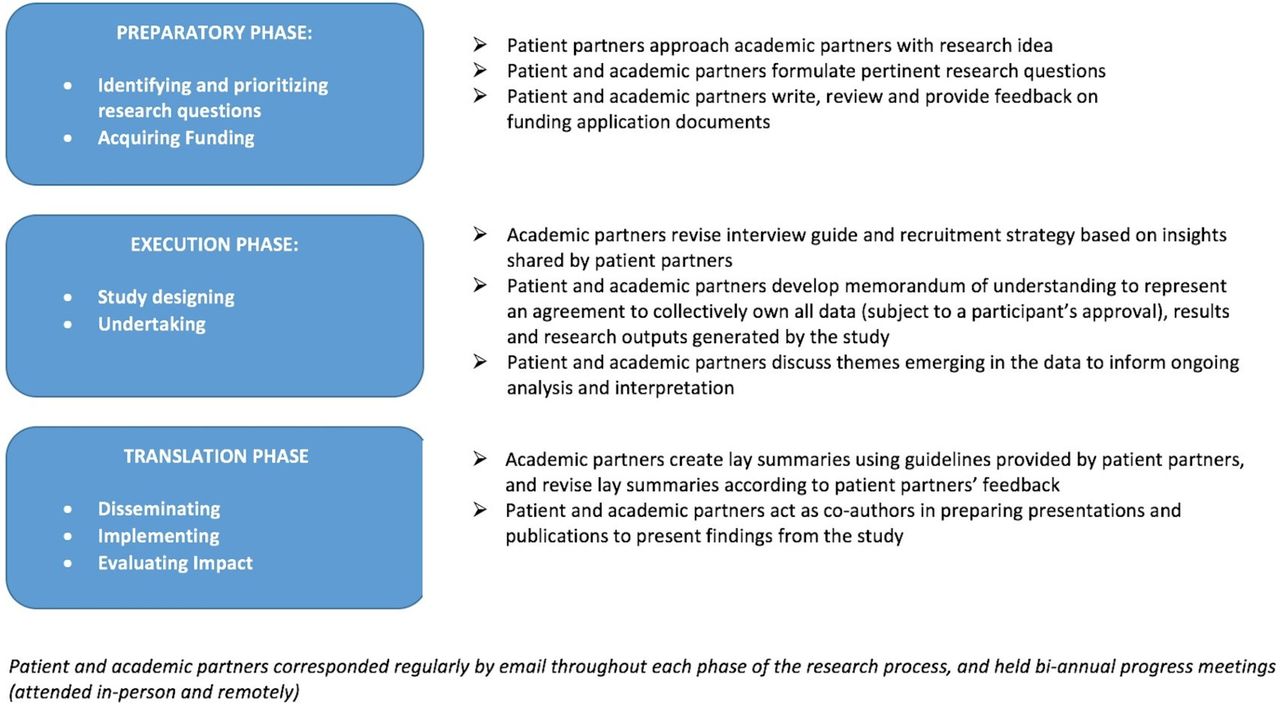
The study was initiated, codesigned and coconducted by patient partners (SK, LG, AMH, WL), who are members of Arthritis Research Canada’s Arthritis Patient Advisory Board, and researchers and trainees at the research centre (see figure 1). Founded by Arthritis Research Canada in 2001, the Arthritis Patient Advisory Board has over a decade long history of partnering with researchers at the research centre. The Advisory Board is a group of volunteers living with at least one form of arthritis, whose mandate is to engage with researchers at the research centre, and to serve as a bridge in disseminating research produced from the centre to the public. To date, the Board consists of 15 members and 23 past members (31 women; 7 men). The majority of members reside across the province of British Columbia, with the exception of one based in Ontario and five in Quebec. Members can be actively involved at any stage of research, including identifying research topics, preparing grant applications, shaping the research design, coauthoring scientific papers, writing plain language summaries and/or attending, and copresenting, at conferences. Two members currently serve as cochairs of the Board, with a paid staff member as a liaison between Board members and researchers at the centre.

{kind=link}
Outline of partnership between patient and academic partners in research process. Each phase of the research study was codesigned and coconducted by patient partners, researchers and trainees at a health research setting in Canada. Figure was created using a framework developed by Hamilton et al to advance the reporting of patient engagement in rheumatology research.40
Participants
We conducted semistructured, in-depth interviews with patients who had experience of building patient partner–researcher relationships. We recruited a convenience sample of past and present members of the Advisory Board that was sufficiently relevant and varied to generate rich data to address our objective. Indeed, participants had engaged to varying degrees with coauthors in previous research studies at Arthritis Research Canada. Participants were recruited via an email invitation and word of mouth. Coauthors SK, WL and AMH were themselves participants in the interviews.
Interviews
We developed a semistructured interview guide (see supplementary appendix A) to elicit participants’ perspectives regardless of their degree of experience with building relationships with researchers. Patient partners were consulted to inform the development of an interview guide that was relevant to the research topic, easy to understand and able to prompt spontaneous description of experiences and feelings from participants. The interview guide was organised into separate but overlapping sections, including: (1) experiences/benefits/downsides of being a patient participating in making decisions with researchers in research; (2) interactions with researchers in research-related activities. Open-ended questions were asked, and probes and prompts used for elaboration. Doctoral students with training in qualitative research (JL and BCT) each conducted half of the interviews. Interviews took place at a time and place convenient for each participant or by phone. Subject to a participant’s permission, JL and BCT also observed interviews conducted by each other to support their ongoing training in qualitative interviewing. Many participants were familiar with JL and BCT’s research interests prior to the interview, given previous interaction at Arthritis Research Canada. The interviews were not the interviewers’ first encounter with the subject area of patient engagement in research. JL had been engaging in research with patients as a research assistant at Arthritis Research Canada since 2010.
Supplementary file 1
The interviews (lasting approximately 30–90 min) were audiotaped and transcribed verbatim. We invited each participant to review and modify the transcript of their interview and provide permission for their transcript to be used for analysis. Only members of the research team who have been granted permission by a participant had access to their full de-identified transcript. We took this step to address any potential discomfort from our participants in sharing their interview data with anyone in the study team.
Data analysis
We applied an inductive, thematic approach to the data.26 No preselected codes were identified prior to analysis. We used constant comparative methods throughout our analysis to find similarities and differences within each transcript and across different transcripts, which helped analysts to continuously interrogate a fuller range of perspectives in the data in order to bring fresh insight.27 Three doctoral students (JL, BCT and GM) independently read and coded a selection of transcripts. They met to identify emerging issues for discussion and develop an initial coding scheme. Codes were then compared between the remaining transcripts, with similar and deviant cases being sought. This process was followed by clustering codes into thematic categories. Coding was carried out predominantly via paper-based methods, and NVivo V.10 was used for storage and management.
Thematic categories were verified, modified or refuted in discussions with co-authors and study participants until it was agreed that categories presented a sufficient range of varied and relevant perspectives to contribute new insight. Peer checking and member checking thus enhanced the rigour of our analysis.28 Thematic categories were then considered in light of aspects of the relational ethics lens, including respect, embodiment and interdependency.23 24 29
Results
Between August and November 2015, a total of 22 from an eligible 33 (67%) current and past members of the Advisory Board consented to participate in the study (table 1). Twenty-one (95%) were female, aged between 26 and 68 years (median=60 years). Thirteen (59%) participants had completed at least one university degree and 10 (45%) were in paid employment. Time spent as a member of the Advisory Board varied from 1 month to 10 years (median=3 years). We identified three themes from the analysis: (1) Being heard; (2) Cobuilding social relations; (3) Adding another spinning plate to an already busy life.
Participant characteristics
Theme 1: being heard
Participants had commonly perceived that researchers’ contributions in research held more weight than their own contributions. Many participants had perceived themselves as lacking experience, knowledge or credentials, which they expressed prompted them to feel inadequate or insecure when they were interacting with (or contemplating the possibility of interacting with) researchers.
I kind of feel like a fraud. I don’t feel like a real researcher. Most people who do research have their Master’s or their PhD and I am sitting here and I have no badge. You know, I have nothing except my life experience that qualifies me to do research (Hannah)
when I’m going to speak for myself… I felt ooh, I’m a consumeri , I don’t have the knowledge that these scientists, these doctors have, so right away, there’s a little bit of discomfort because do I look stupid, ill-informed, unstudied when compared to them (Phoebe Lewis)
I’m not ready or know enough yet… I hope to be able to go to the conferences and to talk to the researchers eventually, when I feel ready (Chloe)
Participants valued researchers who provided reassurances that they deemed patients’ contributions to be important. For many participants, these reassurances strengthened their sense of feeling genuinely respected in their relationships with researchers, which helped them feel at ease to contribute.
…researchers that I was involved with were very encouraging and very respectful. There’s a fear when you start contributing because you wonder if you’re going to be able to contribute anything useful… the researchers put you at ease immediately so that enables you to speak freely… they let us know how important it was for us to be involved (Lori)
…there’s a mutual respect… patients sometimes need encouragement and reinforcement that their views are not lesser… that’s really important because patients are going to be reticent to contribute if they feel it’s tokenism. If they feel it’s really valued then that’s going to encourage them to speak and contribute more freely without fear (Jessica)
Participants’ sense of feeling respected was also strengthened by researchers who were quick to defend patients who felt their contribution or emotional well-being was threatened by other stakeholders participating in the research process.
[In a project involving a multi-disciplinary team,] one of the graphic designers was very disrespectful to the patients. Immediately [researcher] got involved and the problem was settled. All of us felt very protected. You felt like you were part of the team, and that the team leaders would step in if anyone felt hurt or insulted (Lori)
…when the researchers appreciate the contribution that you bring to their project and go to bat for you, you know that you’re all part of the team. I was the only consumer on a panel of doctors and I raised an issue and one of the doctors dismissed it and [researcher] called him on it right at the table and said well I happen to agree with what Phoebe is talking about (Phoebe Lewis)
Many participants also expressed their sense of feeling respected by researchers who actively sought, listened to and acted on patients’ contributions. These active behaviours were viewed as demonstrations of genuine respect for patients’ contributions.
there have been some research projects where our feedback has made a difference in how the research was designed… that’s showing respect to the patient perspective… the researcher has treated me like a colleague in terms of sitting and talking and asking questions (Marie)
I’m sent the material to provide the feedback and inevitably, the changes are incorporated which is really important for a patient to see… it might be tweaked in some way but you know you’re being listened to, that you’re being valued, that it’s not tokenism (Jessica)
I don’t need any accolades or anything like that… If there’s an appreciation, you know, that your voice matters, that your input matters and yes we hear you, I think that’s really important (Laura)
I think when a researcher is asking questions to confirm their questions for their studies, they are asking us for our opinion… Sometimes I feel that when we explain where we’re coming from and what’s worked and what hasn’t worked and what the barriers are, the researcher listens and might change or modify what they’re going to be using as their topic… The researcher values our input. (Deka)
A few participants, however, expressed a need to reassess the weight of patients’ contributions in research projects. Olivia, for example, emphasised instances in which projects were shaped predominantly by patients’ contributions and the expertise of researchers had been discounted. In her experience, this had been to the detriment of the research quality. She highlighted that, if the value of patients’ contributions was not well balanced with that of researchers, there was a risk that the quality of research could be negatively affected. She expressed that questions remain about how to find the optimal balance in valuing the distinct contributions to research by patients and researchers (as different in kind, but not in degree of importance). Finding this balance was viewed to support building a relationship of reciprocity in which patients’ and researchers’ contributions are equally important for achieving quality in research.
I’ve seen patients shape some projects… what I saw these investigators had at the end was a much less generalizable project… I don’t think that you can discount years of research training for patient experience… we need to figure out the best way to give them both critical weight and maximize each one… The patient is just as important as the researcher, and the researcher is just as important as the patient (Olivia)
Theme 2: cobuilding social relations
Some participants (particularly past members of the Advisory Board) reflected that, in the early days of development of the Advisory Board, the paid support of a researcher to cochair the board had provided ‘the bridge’ needed to build social relations between patients and researchers. One participant viewed this facilitated process of building social relations with researchers as conducive to establishing patients’ sense of mutual respect.
…at the beginning, [researcher] was the co-chair… he was our relationship builder amongst the researchers… Things changed when budgets changed, so we ended up not having that kind of support. We changed to having two patient cochairs at that time… but by then we knew a fair number of the researchers (Julie)
[researcher] provided the bridge between [the Advisory Board] and the research scientists. He had the inside scoop… he was always connecting us with information and people… but as a group we also realized that this was an impossible structure to maintain because researchers are far too busy (Lori)
He was a very friendly, open fellow and he made sure that the ARC [Arthritis Research Canada] scientists knew about us and that we knew about them. So what he did basically was make us feel comfortable and very accepted by the researchers… It was sort of like a mutual respect thing that [researcher] made us realize (Phoebe Lewis)
Participants valued building social relations with researchers in which there was some informal acknowledgement of each other as people beyond their roles within a particular project. This acknowledgement was viewed as important by participants because it helped to mitigate the risk of feeling uncomfortable emotions (eg, feelings of inadequacy or insecurity) that could be provoked by their perceived power differentials.
Everybody was on a first-name basis and right away that power hierarchy is dismissed. So when you’re sitting across the table from a researcher and he’s just talking about his research as casually as if he was at a Sunday picnic, all of a sudden your comfort level as a consumer goes up… [researcher] would just sit down like the rest of us and eat and talk and sometimes share confidences… We felt quite comfortable passing them in the hall and saying hi. We knew a little bit about their families. They knew about ours (Phoebe Lewis)
…we’re meeting informally and that’s really important… those are the people that number one, are asking us to participate in what they’re doing and if you’re comfortable with somebody in a social event… I’ve already met you guys, I know what’s happening, not in your lives necessarily but yeah I know who got married… that’s a big deal (Victoria)
…we have so many opportunities for face-to-face and I’ve been to his lab a couple of times and I chatted to him at different events and so I’m comfortable to just zing it out there. I wasn’t afraid if he says ‘no’ or intimidated… (Julie)
Participants valued building social relations with researchers on an ongoing basis over time, with some identifying this as a defining part of genuine patient engagement in research. Genuine patient engagement in research (sustained over time) was also described as a reciprocal exchange or two-way dialogue that flowed with ease between patients and researchers.
Some of the researchers I’ve never actually met still even after being there for three years… maybe if the researchers consider ways to communicate to us more openly what they’re working on… there’s a few researchers that really stand out that are constantly in contact with us… that’s why we nominated [researcher] for the award because she is so great about being in touch with us on a constant basis… I find when we’re in close contact like that with a researcher we get to know them, they get to know us… we see her… she’s been present in various ways at a number of meetings over the past year’ (Norma)
I really like that the researchers talk to patients and tell them where they’re at with their studies whether it’s part way through or going to be published or it has been published… (Deka)
There’s an ongoing relationship that enables more in-depth partnership… true engagement is a continuing two-way dialogue, it’s not just project-specific (Jessica)
the one key thing is their camaraderie that happens between the researchers and [members of the Advisory Board]. That’s critical in continuing an exchange that has no barriers and is quite free flowing (Madeline)
I agreed to be on this research study as a patient member… they introduced me to the team but they didn’t introduce me to anybody, so everybody knew who I was and I was a patient but as for their roles and their names I had no clue… that was a less successful engagement (Hannah)
Theme 3: ‘adding another spinning plate to an already busy life’
Many participants described how they managed their relationships with researchers and their roles within research projects among existing priorities in their daily lives. Many highlighted, for example, how their relationships with researchers were impacted by their arthritis.
when you have a chronic and crippling disease… it’s sort of the guardian at the gate, it shapes and interferes with and constrains your relationships with the world… it’s a cage you live in… you have to live within that constraint in every single one of your relationships (Heather)
Several participants perceived themselves as having not contributed enough, with tasks related to their engagement in research that were ‘hanging over my head’. Others experienced stress, fatigue and guilt while adding their work as patient partners to their existing priorities. A few participants provided examples of how being patient partner resulting in negative impacts for other valued relationships in their lives.
[there is a] constant guilty, nagging feeling that I’m not doing enough… I have thought about [stepping down from being a patient partner] for that reason… basically I felt honestly um pressure, yeah, pressure, being involved… I have no personal time… my job has been very time consuming. So between all those things, um, it gives me very little time um for my husband [laughs] (Sarah)
it’s adding another spinning plate to an already busy life… it could be taking from time that you might otherwise have spent looking after yourself (Jessica)
Participants valued relationships with researchers who recognised they were managing their role as patient partners among multiple obligations, priorities and their own health. Acknowledging this required researchers to show consideration for what was going on in participants’ lives beyond the research setting. Participants valued this kind of consideration as a demonstration of respect and empathy. They often described showing consideration to involve researchers taking a flexible and accommodating approach in their interactions. Examples of this approach included working together to set deadlines, or providing food during a meeting.
…you’re already dealing with so much yourself, personally in your home life, your own health, your own work life… if you’re not able to contribute to the same degree because you’re in a flare, there’s a level of understanding and appreciation [from researchers] that you don’t have to feel guilty… there are a huge number of tasks from writing letters of support, to writing lay summaries… nobody is going to make you feel bad at all when you can’t do it (Mary)
…the research team send out a newsletter regularly to their study participants… they draft the newsletter and then I provide feedback and suggestions for edits that I feel may be helpful in improving the language and interpretation of the key messages to the patients… [I was] sent a draft of the newsletter [by a researcher]. Would you have some time to review it before I send? So I think that’s really nice… you’re not just sent something without a warning and then expected to be able to find time in their deadline to do it… I replied back that I have a number of commitments, was the deadline flexible… and right away the response was yes… again, the communication indicates that there’s respect (Jessica)
…researchers are so understanding… that these people live with certain restrictions on how much they can take on and for me I don’t even know if that’s illness related or if it’s just a human can only do so much… meetings were called… the researchers would have questions that they wanted to consult with you on… there was usually food. [Providing food] is actually really nice… when you have a chronic disease, especially one with this much pain, you have to really decide where you’re gonna expend your energy because you only have so much… so you should make it worth their while (Olivia)
It was also recounted by participants that showing consideration for what was going on in participants’ lives beyond the research setting involved researchers having concern for the health and emotional well-being of patient partners.
We were at a conference, and one of the [patient partners] became very ill and they had to call the ambulance. [Researcher], busy as she was, approached me and gave me her personal phone number in case this [patient] needed assistance. She told me to call her if we needed anything and she meant it! It was a tremendous show of concern and support’ (Lori)
[Researcher] knows that I had a hip problem… She says, ‘you know Laura you might want to, you know, try for a consult because there’s a long waitlist’… she gave me resources… she just came across as someone that was kind of like a caring individual, like personality-wise. (Laura)
The [researchers] understand you need to look after yourself and that’s what they want for you personally as well (Mary)
Discussion
Our study is one of the first to address ethical questions of how researchers and patient partners ought to treat each other on an everyday basis when engaging with each other in research. As one of the few empirical studies to examine components of patient engagement in research from patients’ perspectives, findings help to fill a wider gap of research evidence on patient views, experiences and preferences.2 This gap poses a barrier that hinders the development of best practice of engaging patient partners in research-related activities. A key strength is that findings are grounded in the perspectives of patients with varying levels of experience of building relationships with researchers in research-related activities, as well as a wide variation in age (table 1).
Drawing on key aspects of the relational ethics lens (ie, respect, embodiment, interdependency), our findings highlight benefits and risks encountered by patients in building relationships with researchers to optimise their engagement in the research process. Respect can be demonstrated by valuing patients’ and researchers’ distinct contributions as equally important in research. Based on participants’ experiences, embodiment highlights there is a risk of patient partners feeling negative emotions, such as insecurity, inadequacy, fear, guilt, stress, when interacting with researchers. Interdependency highlights how participants valued building social relations with researchers in which there was some informal acknowledgement of each other as individuals beyond the role of researcher or patient partner. The value of creating space for informal talks between patients and researchers has also been highlighted elsewhere in the literature.4 14 For example, Schipper et al report that informal talks offered an opportunity for patient partners and researchers to exchange experiences and foster mutual understanding.4 Rather than ‘warm, fuzzy’ extras, our findings add the insight that informal interactions are valued by patient partners as they help to mitigate the risk of experiencing negative physical and emotional impacts of adding engagement in research as ‘another spinning plate’ to other priorities in their daily lives.
Our findings are situated within broader theoretical debates about the status of medical and scientific knowledge, and the value of subjective, experiential knowledge.30 Indeed, there is growing acceptance of the value of subjective, experiential knowledge in health research as seen, for example, in the emergence of patient-reported outcome and patient-reported experience measures within the biomedical community.31 Crediting subjective, experiential knowledge can question the conventions of positivism, which credit ‘lay’ knowledge with less legitimacy than scientific knowledge traditionally contributed in research by researchers.30 Participants valued researchers who challenged this traditional positivist outlook by actively demonstrating that subjective, experiential knowledge contributed by patient partners could be equally important to achieving quality in research. Participants described ways in which researchers actively demonstrated that patient partners’ contributions were valued as equally important. These findings present ways in which researchers can meaningfully recognise the contributions of patient partners, which has been identified in the literature as an important part of facilitating the inclusion of patient partners in research.1 4 5 16 32–34
Importantly, our findings also caution there is a risk of researchers’ contributions being discounted when engaging with patient partners, to the detriment of research quality. As one participant stated: ‘I’ve seen patients shape some projects… what I saw these investigators had at the end was a much less generalizable project’. Indeed, in a qualitative study by Lindenmeyer et al, in-depth interviews with researchers revealed that one had faced criticism from a funding body for ‘giving too much power’ to patient partners.35 This prompts further questions. For instance, do researchers feel their contributions in research are at risk of being discounted when engaging with patient partners? Are there other risks being experienced by researchers when engaging with patient partners and, if so, how could they be mitigated? Schipper et al reported, for example, that a researcher felt insecure when feeling she had to empower the patient partners she was engaging with, but did not know how.4 Researchers’ experiences in their relationships with patient partners are currently understudied, and further research is warranted to identify potential gaps where support may be helpful from researchers’ perspectives.
Limitations
As in all qualitative research, we recognise that there are limitations to the transferability of these findings. For example, given that the vast majority of participants were women, it seems possible that findings are more transferable in contexts involving female rather than male patient partners. We note also that 59% of participants had at least one university degree (table 1), which is markedly higher than Canada’s general working-age population, with estimates of 24.7% having attained at least one university degree.36 Other published studies have highlighted that issues of diversity in patient engagement in research warrant further examination.37–39 We recognise there may be limitations in the degree to which our findings might be transferred in situations involving patient partners of different sociodemographic characteristics than in the context of our study.
Conclusion
Drawing on a relational ethics lens, our findings illuminate some important benefits and risks that patient partners can experience when fostering relationships with researchers, in order to optimise patient engagement in research. By gaining understanding of these benefits and risks, patient partners and researchers are better positioned to act ethically towards each other in ways that maximise benefits and minimise risks. Our findings are a critical step in supporting an ethically sound practice of patient engagement in research that prioritises patients’ perspectives.
Acknowledgments
Special thanks to all of the participants who shared their time and experiences for the purposes of this qualitative study.
References
Footnotes
↵ i The Arthritis Patient Advisory Board was formerly known as the Consumer Advisory Board. The name was changed in 2014 because it was felt by members that the term ‘consumer’ denoted an individual who purchased information or healthcare by choice. Members felt it was more accurate for them to identify with the term ‘arthritis patient’.
Contributors JL contributed to the study concept and design, generation, analysis and interpretation of data, drafting and critical revision of the manuscript. GM contributed to analysis and interpretation of data, as well as drafting and critical revision of the manuscript. SK, LG, AMH, WL, BCT and LCL contributed to the study concept and design, interpretation of data and critical revision of the manuscript. BCT also contributed to generating data and analysis. AFT contributed to interpretation of data and critically revised the manuscript.
Funding This work was supported by "PRECISION: Preventing Complications from Inflammatory Skin, Joint and Bowel Conditions" a Team Grant from the Canadian Institutes of Health Research, Canada (THC-316596) and the Vancouver Foundation (UNR15-0037).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The University of British Columbia’s Behavioural Research Ethics Board granted ethical approval for the study (#H15-00217).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.