Article Text

Abstract
Objective The purpose of the study was to investigate whether low education level was associated with patients’ health-related quality of life (HRQOL) after oesophageal cancer resection.
Setting A nationwide cohort study in Sweden.
Participants In total, 378 patients who underwent oesophageal cancer surgery in 2001–2005 were followed up 6 months and 3 years after surgery.
Outcome measures HRQOL was assessed by the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30 (QLQ-C30) and the oesophageal cancer-specific module. The association between level of education and HRQOL was calculated with linear regression models, providing mean score differences (MD) and 95% CIs. Data were analysed separately for women and men.
Results Education level was not associated with HRQOL recovery after oesophageal cancer surgery. However, when data were stratified by sex, lower education was associated with worse emotional function (MD −13; 95% CI −22 to −3), more symptoms of insomnia (MD 20; 95% CI 8 to 32) and reflux (MD: 15; 95% CI 3 to 26) for women, but not for men. Among women, low education was in general associated with worse functioning and more symptoms.
Conclusions Low education was not associated with worse HRQOL after oesophageal cancer surgery. However, when data were stratified for sex, low education level was associated with worse functioning and more symptoms in certain HRQOL domains for women, particularly in a short-term perspective. For men, no such association was found.
- hrqol
- long-term follow-up
- oesophageal neoplasm
- cancer survivorship
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
A population-based, nationwide design with high inclusion rate of all eligible patients in Sweden.
Robust exposure measure reducing the risk of misclassification.
Limited statistical power to detect weak or moderate differences, particularly in the stratified analysis.
Introduction
Surgical resection is an essential part of curatively intended treatment for oesophageal cancer.1 Due to advances in treatment, survival rates have increased during the last decade, which in turn has made health-related quality of life (HRQOL) an even more important and acknowledged outcome measure.2 Most patients reach preoperative HRQOL levels 1 year after surgery.3 However, a prospective population-based study showed that 50% of the included patients did not improve in global quality of life between 6 months and 5 years and 17% deteriorated further.4 Despite being cured, these patients seem to suffer from debilitating and persistent symptoms even up to 10 years after surgery.5 This accentuates the need to identify factors, not associated with the surgery itself, but with person-related issues that may promote or impede HRQOL recovery. Comorbidity may to some degree influence the recovery in HRQOL,6 but does not fully explain the long-term HRQOL deterioration. Thus, it still remains unclear what prevents full HRQOL recovery after oesophagectomy. Higher education has been shown to have a beneficial effect on survival for patients with cancer.7 8 For patients with oesophageal cancer, a nationwide study showed that higher level of education was associated with lower mortality rates.9 Since education seems to be an important factor for predicting outcome, we hypothesised that low education level is associated with, increased mortality, and reduced HRQOL after oesophageal cancer resection. Moreover, the association of healthcare and HRQOL seems to differ between men and women.10 11 Therefore, we also aimed to investigate whether education level influences HRQOL recovery differently for men and women.
Methods
Study design
A Swedish nationwide cohort study including patients curatively operated on for oesophageal cancer during a 5-year period (2001–2005). Patients were followed up until the end of 2008, that is, up to 3 years following surgery.
Data collection
A detailed description of this nationwide data collection has been published elsewhere.12 13 In brief, the study was based on a nationwide network of 174 Swedish hospital departments with contact clinicians involved in diagnostic procedures or treatment of patients with oesophageal cancer, in which 90% of eligible patients were included. Information regarding patient and tumour characteristics, treatment, and complications were prospectively collected, and based on a predefined study protocol to ensure completeness and uniformity. Comorbidity was predefined as diabetes, cardiac, respiratory, renal or other specified conditions.14 Information about comorbidity was collected from the Swedish Patient Register, which contains all in-hospital diagnoses in Sweden since 1987 and all outpatient specialist care since 2001. Patients’ self-reported HRQOL was collected by validated questionnaires at 6 months and 3 years after surgery for oesophageal cancer.
Education level
Information on education was obtained from the Longitudinal Integration Database for Health Insurance and Labour Market (LISA). LISA holds registration since 1990 and is updated yearly with information on the highest formal education level attained by each Swedish resident.15 The highest attained education level at the time of the oesophagectomy was classified into two categories: (1) Higher education, represented by 10 years or more of formal education, including postsecondary education and (2) Compulsory education, which corresponds to 9 years or fewer, including primary and lower secondary education, that is, up to the age of 16 years.
HRQOL assessment
HRQOL was assessed using two self-administered questionnaires, both developed and validated by the European Organisation for Research and Treatment of Cancer Quality of Life (EORTC).16 17 The EORTC Quality of Life Questionnaire-Core 30 (QLQ-C30) consists of 30 items that measure HRQOL aspects in patients with cancer in general.16 Questionnaire items are grouped into one global quality of life scale, five function scales (physical, role, emotional, cognitive and social), three symptom scales (fatigue, nausea/vomiting and pain) and six single items (dyspnoea, insomnia, appetite loss, constipation, diarrhoea and financial difficulties). An oesophageal cancer-specific module (OES18), the EORTC QLQ-OES18 was used to assess problems common among patients with oesophageal cancer.17 This 18-item questionnaire consists of four scales (dysphagia, reflux, eating difficulties and oesophageal pain) and six single items (trouble swallowing saliva, choking, dry mouth, coughing, speech difficulties and problems with taste). In both questionnaires, the four response alternatives were: ‘not at all’, ‘a little’, ‘quite a bit’ and ‘very much’. The only exception was the items in the global quality of life scale, which had a seven-graded rating, ranging from 1 (‘very poor’) to 7 (‘excellent’).
Clinically relevant mean HRQOL differences between groups were handled according to the classification of Osoba et al,18 where changes of ≥10 points were considered to be clinically relevant and noticeable for the patients.
Statistical analyses
Questionnaire responses were linearly transformed into scores between 0 and 100 according to the EORTC manual.19 Higher scores in the global quality of life scale and function scales are equivalent to better HRQOL, whereas for symptom scales and individual items, a higher score is interpreted as more symptoms. The association between level of education and HRQOL was calculated with linear regression models, providing mean scores, mean score differences (MD) and 95% CIs. High education was used as reference. The analyses were performed separately for 6 months and 3 years and further stratified for men and women. The multivariable regression model was adjusted for age (<60, 60–75 or <75 years), sex, number of comorbidities (0, ≥1 according to the Charlson Comorbidity Index20), tumour stage (0–I, II, III, IV) and tumour histology (squamous cell carcinoma or adenocarcinoma) tumour location (upper/middle, lower oesophagus or cardia), body mass index ≥25 kg/m2 and complications within 30 days of surgery (yes or no). A difference of ≥10 mean HRQOL scores between education groups was regarded as clinically relevant18 and statistical significance was tested (with two-tailed test and 5% level of significance where no adjustments for multiple testing were made) only when the MDs were clinically relevant. An experienced senior biostatistician (AJ) conducted all data management and statistical analysis according to a predefined study protocol (online supplementary file: study protocol). The statistical software SAS V.9.4 (SAS Institute) was used to all statistical analysis.
Supplementary file 1
Patient involvement
Patients and public were not involved in the design of the study. Findings from this study will be communicated to patients and healthcare professionals through conferences and patient meetings.
Results
Patients
During the study period, 614 patients underwent oesophageal cancer surgery. Of these patients, 490 survived for at least 6 months, and 401 patients (82%) completed the HRQOL questionnaires. Twenty-three patients were excluded due to missing data. Thus, 378 patients (75%) were included in the study. Among the included patients, 209 survived for 3 years, of whom 172 (82%) completed the 3-year follow-up questionnaires. Patient, tumour and therapy characteristics were similar between responders and non-responders (online supplementary file table 1A, B). Deaths did not differ by gender or by education level (data not shown).
For the 6-month survivors, 174 patients (46%) had compulsory education corresponding to 9 years or fewer and 204 patients (54%) had attained a higher education. Patient characteristics were similar between the groups except that patients with lower education were generally older at the time of surgery and had greater comorbidity (table 1).
Patient, tumour and therapy characteristics of 378 patients 6 months after oesophageal cancer surgery, categorised by education level
For the 3-year survivors, 78 patients (45%) had a compulsory education only. Patient and tumour characteristics were comparable for the two groups except for that patients with lower education had more comorbidities (table 2).
Patient and tumour characteristics and health-related quality of life 3 years after oesophageal cancer surgery (n=172), categorised by educational level
Low education level and HRQOL
Education level did not influence HRQOL recovery at 6 months or 3 years after surgery. Global quality of life, functions, general and oesophageal cancer-specific symptoms were similar between patients with low and high education level with no clinically relevant differences in mean HRQOL scores (table 3).
Mean score differences with 95% CIs in HRQOL between patients with high education level (≥10 years) versus low education level (≤9 years) 6 months and 3 years after oesophageal cancer surgery
Education level and short-term HRQOL in women and men
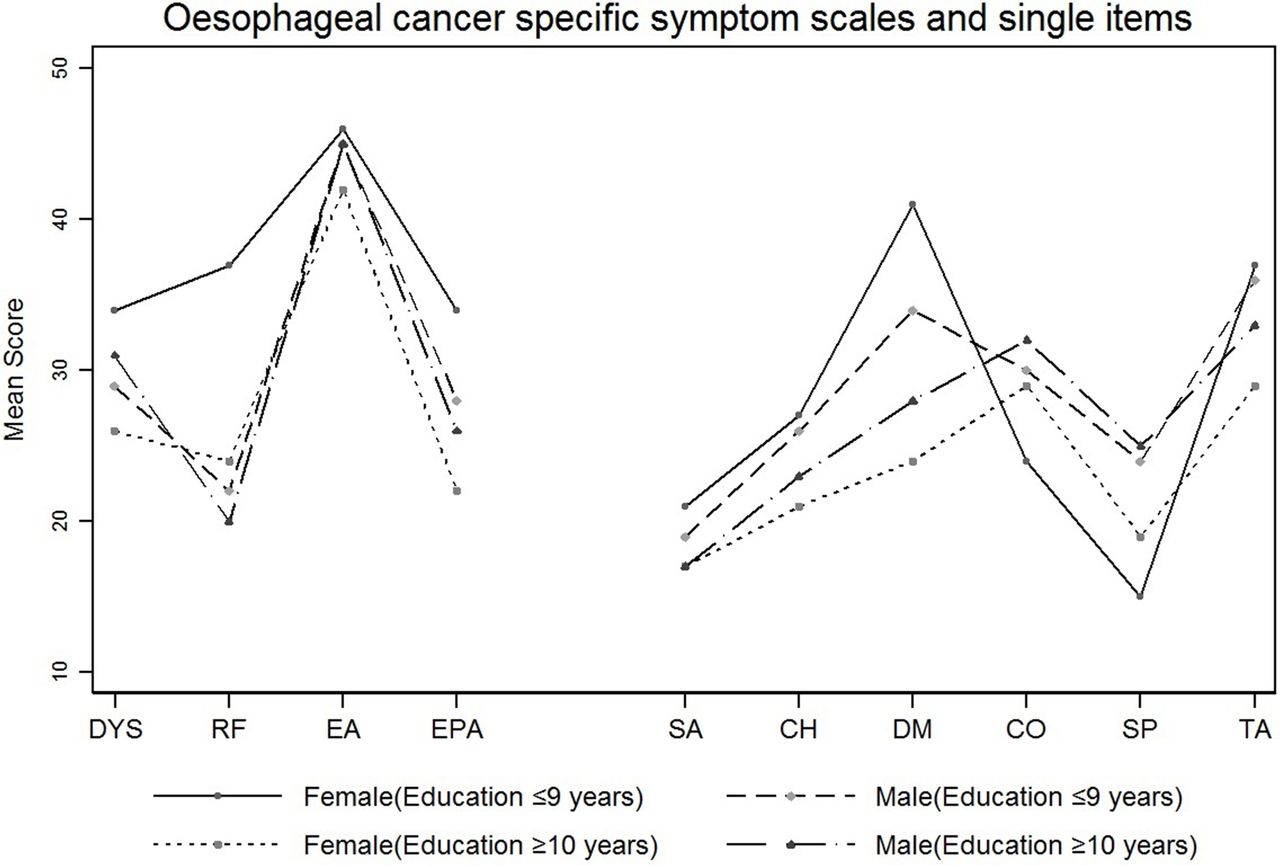
For patients with low education level, women reported clinically relevant and statistically significantly worse emotional function (MD −13; 95% CI −22 to −3), more symptoms of insomnia (MD 20; 95% CI 8 to 32) and reflux (MD 15; 95% CI 3 to 26) compared with men. Among women, low education was associated with clinically relevant and statistically significantly worse emotional function (MD −22; 95% CI −34 to −11), cognitive function (MD −20; 95% CI −30 to −10) and social function (MD −14; 95% CI −28 to −1) as well as more symptoms of fatigue (MD 14; 95% CI 1 to 26), pain (MD 21; 95% CI 7 to 34), insomnia (MD 22; 95% CI 8 to 36), oesophageal pain (MD 12; 95% CI 1 to 24) and dry mouth (MD 17; 95% CI 2 to 32). Among men, low education level was not associated with reduced HRQOL (table 4, figures 1 and 2).
Mean differences with 95% CIs in HRQOL between men and women with high education level (≥10 years) versus low education level (≤9 years) 6 months after oesophageal cancer surgery
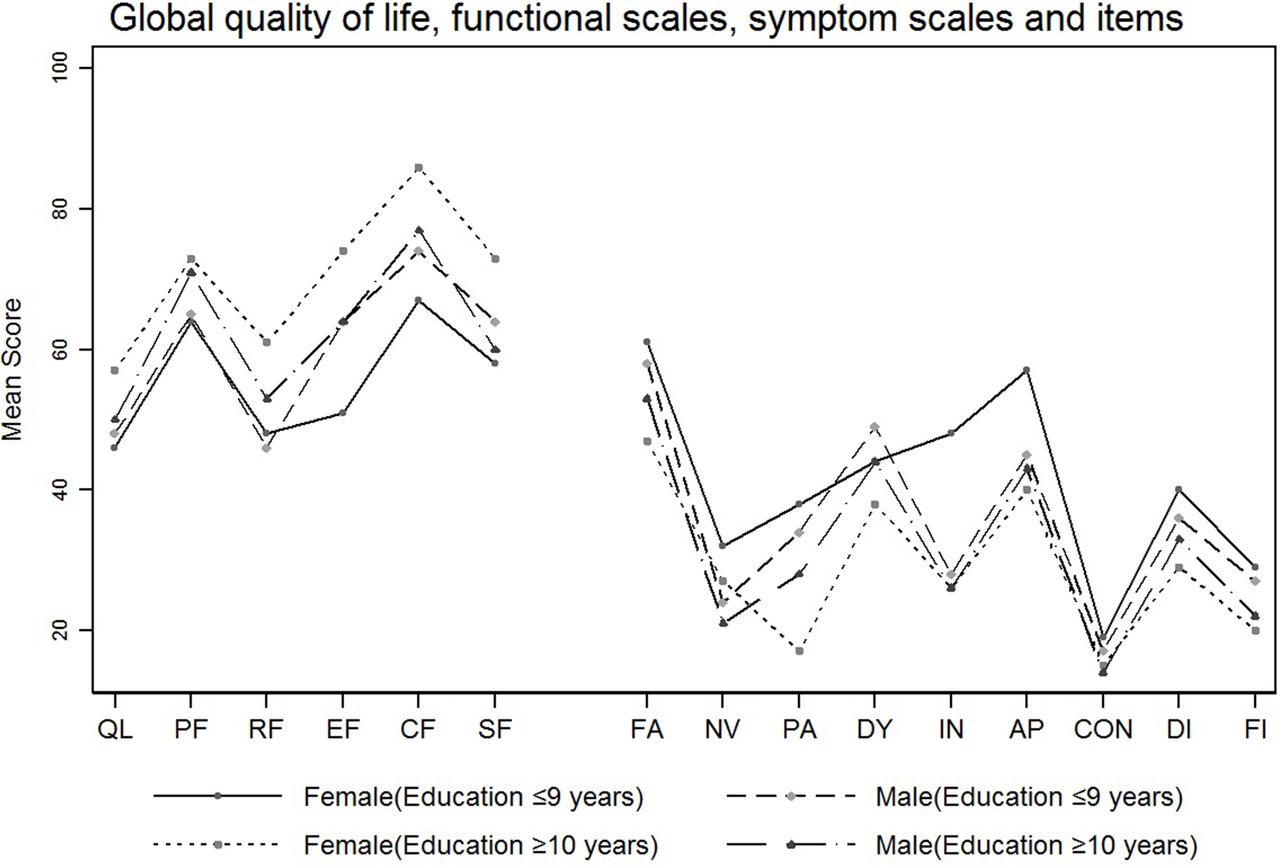
Global quality of life (QL), functional scales, symptom scales and items in men and women with high and low level of education 6 months after oesophageal cancer surgery. In QL and functional scales, high scores indicate better HRQOL. High scores in symptom scales and items correspond to more symptoms. AP, appetite loss; CF, emotional function; CF, cognitive function; CON, constipation; DI, diarrhoea; DY, dyspnoea; EF, emotional function; FA, fatigue; FI, financial difficulties; HRQOL, health-related quality of life; IN, insomnia; NV, nausea/vomiting; PA, pain; PF, physical function; RF, role function; SF, social function.
{kind=link}
{kind=link}
Oesophageal cancer-specific symptom scales and items in men and women with high and low education level 6 months after oesophageal cancer surgery. Higher scores correspond to more symptoms. CH, choking; CO, coughing; DM, dry mouth; DYS, dysphagia; EA, eating difficulties; EPA, oesophageal pain; RF, reflux; SA, trouble swallowing saliva; SP, speech problems; TA, problems with taste.
Education level and long-term HRQOL in women and men
Low education level was associated with several clinically relevantly poorer functions and symptoms for women compared with men but only problems with taste was also statistically significant (MD 22; 95% CI 4 to 40; p 0.02). For women, low education was associated with clinically and statistically significantly worse role function (MD −25; 95% CI −46 to −3), emotional function (MD −15; 95% CI −30 to 0), social function (MD −22; 95% CI −39 to −4) and more financial difficulties (MD 17; 95% CI 1 to 32) as compared with those with higher level of education. Among men, only appetite loss was found to be clinically significantly worse (MD −12; 95% CI −23 to −1) in those with a low level of education (table 5).
Mean score differences with 95% CIs in HRQOL between men and women with high education level (≥10 years) versus low education level (≤9 years) 3 years after oesophageal cancer surgery
Discussion
In this nationwide study on patients with oesophageal cancer treated with surgery, low education was not associated with worse HRQOL in the short or the long term for the total group. However, in women, low education was associated with worse functioning and more symptoms in certain domains.
The nationwide data collection contributes to strengthening the validity of the results. The exposure measure, education level, was used as a proxy for socioeconomic position. Education level is relevant to people regardless of age or working circumstances, a relatively robust measure and easy to assess.21 Information about education level was collected from a database that contains valid and updated information on education for all Swedish citizens, which reduces the risk of misclassification. However, other variables such as income, occupational or marital status may also be of importance for HRQOL recovery but were not included in this study.
A limitation of the study is the lack of preoperative HRQOL data. Still, using preoperative baseline data to measure recovery in HRQOL entails inherent flaws since at such a time, patients’ HRQOL is typically highly influenced by the disease itself and psychological factors.
The participation rate was 75% which could potentially have induced selection bias in the study. However, the non-responders did not differ in characteristics from the participants, and therefore, it is not likely that non-participation would be due to education level. The study was not powered to detect weak or moderate differences in the subgroup analyses. There is a known male predominance in oesophageal cancer,22 and when stratifying data by gender, the group of remaining women was relatively small. To increase the statistical power, especially for the 3-year data and for subgroup analyses, a binary classification of the variable for education level was used. Using a more refined categorisation would have enabled an interpretation about the social gradient which the present results do not allow. To reduce the risk of multiple testing and chance findings, we only tested for statistical significance when a clinical relevant difference was reached. The choice of cut-off for such clinical significance was based on previous research.18 Available research on clinical significance levels is based on the core QLQ-C30 questionnaire23 and since the current study also included a disease-specific module the same cut-off was used for all scales and items.18 In this study, patients had survived oesophageal cancer surgery for 3 years that may have lowered their standards of expectations of HRQOL. This response shift may have influenced the results,24 but is not likely to have induced differences between groups. The data collection of the study ended in 2008; even though this is not the most recent, there is no reason to believe that education level has less influence on HRQOL today compared with some years ago. However, the treatment of patients with oesophageal cancer has developed during the last decade, for example, today perioperative oncological therapy is often included in the treatment. This may influence the generalisability of the results.
Previous studies have shown an inverse relationship between education level and HRQOL for patients with different diagnoses.25–28 In this study, no such association was found until data were stratified by sex. The male predominance in patients with oesophageal cancer may have contributed to mask any gender-specific finding. HRQOL may be perceived differently by men and women10 11 and it seems likely that experiences of being diagnosed with cancer and undergoing an extensive surgical procedure follow the same pattern. Studies on psychological aspects have reported that women are more likely to experience physical and emotional symptoms associated with stress and are also more likely to report lower HRQOL life than men.29–31 Also, inequalities in socioeconomic status seem to be more important for women than for men,29 32 a result that was confirmed by our study. Being in the highest income category and working full time are important predictors for women’s good health.33–36 One possible explanation may be that a higher education level is related to a stronger awareness of the disease and better coping ability with the challenges of a cancer diagnosis. In a study of women with breast cancer, higher education was associated with better coping behaviour.37 This information is valuable when designing follow-up strategies after oesophageal cancer surgery. Women with low education level are a vulnerable group of patients who may need intensified support along the pathway of cancer survivorship to obtain an optimal recovery in HRQOL.
Conclusion
In this nationwide study, low education was not associated with worse HRQOL after oesophageal cancer surgery. However, when data were stratified for sex, low education level was associated with worse functioning and more symptoms in certain HRQOL domains for women. Based on the results of this study, future cancer survivorship research would benefit from including a gender perspective on HRQOL.
Supplementary file 2
Supplementary file 3
Acknowledgments
We would like to acknowledge all the patients who graciously participated in the study.
References
Footnotes
Contributors ARS, AJ, KM and PL contributed with input in designing the study. Data collection and assembly of data were performed by PL. Data analysis was conducted by AJ. All authors (ARS, AJ, KM and PL) contributed in interpreting the results, manuscript writing and approval of the final version of the manuscript.
Funding This work was supported by the Swedish Cancer Society (Grant number: 140323) and the Cancer Research Foundations of Radiumhemmet (Grant number: 141223).
Disclaimer The funding sources had no role in the design and conduct of the data collection, management, analysis and interpretation of the data or preparation review or approval of the manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study is approved by the Regional Ethical Review Board, Stockholm, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data underlying the findings are presented in the manuscript. The original database is not accessible through public repository, but available from the Swedish Esophageal and Cardia Cancer Registry at Karolinska Institutet, whose authors may be contacted at pernilla.lagergren@ki.se.