Article Text

Abstract
Objectives To determine the proportion of contacts to general practitioner (GP) with recent onset gynaecological cancer alarm symptoms (pelvic pain, postmenopausal bleeding, bleeding during intercourse or pain during intercourse) and to analyse the associations between lifestyle factors, socioeconomic status and GP contact for these symptoms.
Design Cross-sectional survey combined with data from national registers.
Setting The general Danish population.
Participants A total of 25 866 non-pregnant women ≥20 years completed the survey. Women reporting at least one of four gynaecological alarm symptoms within the preceding 6 months form the study base (n=2957).
Results The proportion of women reporting GP contact ranged from 21.1% (pain during intercourse) to 32.6% (postmenopausal bleeding). Women aged 60+ years had higher odds of reporting GP contact for at least one of the four gynaecological cancer alarm symptoms compared with those aged 20–39 years (OR 2.56, 95% CI 1.69 to 3.89), and immigrants had higher odds of reporting GP contact for at least one of the symptoms (OR 1.56, 95% CI 1.13 to 2.15) compared with ethnic Danish individuals. Among those reporting postmenopausal bleeding and/or bleeding during intercourse, women in the age group 60+ years had higher odds of reporting GP contact compared with those aged 20–39 years (OR 2.79, 95% CI 1.33 to 5.87). A high educational level (>12 years) was positively associated with reporting GP contact for postmenopausal bleeding and/or bleeding during intercourse compared with a low educational level (<10 years) (OR 2.23, 95% CI 1.19 to 4.19). No associations were found with lifestyle factors.
Conclusions Few women contacted their GP with recent onset gynaecological cancer alarm symptoms. Higher age, being immigrant and higher educational level increased the odds of GP contact. Future studies should explore the reasons for these findings as this may aid in prompting early diagnosis and thereby improve the prognosis of gynaecological cancer.
- gynaecological cancer
- symptoms
- lifestyle
- socioeconomic status
- healthcare seeking
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The population is large, which enables investigation of small subgroups.
Socioeconomic data are obtained from national registers of high quality.
Telephone interviews enabled additional responses from individuals who are usually rarely represented in surveys.
General practitioner (GP) contacts are seen in relation to experienced symptoms, thus reflecting true actions rather than hypothetical situations.
Data regarding GP contacts are self-reported and thus may be prone to bias.
Introduction
Several studies have shown that late-stage cancer diagnosis is associated with reduced survival.1–3 This is also the case for gynaecological cancer, and timely diagnosis and treatment are thus considered essential for prognosis.
For most patients, the diagnostic process is still initiated based on a symptom presentation, although some patients are diagnosed through screening programmes.4 The time period from the first symptom to diagnosis consists of several intervals, and each of these intervals contributes to the overall time spent in the diagnostic process.5 To reduce both the patient interval and the diagnostic interval,5 several countries have implemented referral guidelines and organisational changes.6 7 Most of these guidelines suggest that individuals presenting with symptoms indicative of cancer (alarm symptoms) should be urgently referred to specialised investigative trajectories. Some of the symptoms mentioned in guidelines are commonly occurring and often caused by benign conditions,8 which poses a clinical challenge due to the rather modest positive predictive values for cancer. On the other hand, most of the cancers must be detected among symptomatic individuals,4 which justifies the approach with fast-track investigations. Some of the symptoms prompt investigation as single symptoms, eg, postmenopausal bleeding, whereas others, eg, pain during intercourse, are rather considered as alarm symptoms in combination with other symptoms.
A prerequisite for the general practitioner (GP) to refer to specialised investigations is, however, that individuals contact the GP when experiencing symptoms. Evidently, not all symptom experiences lead to healthcare seeking,9–11 and several parameters might affect the decision to contact a GP with symptoms, such as socioeconomic status (SES),12 experience with illness13 and lifestyle factors (eg, smoking status, alcohol intake and body mass index (BMI).14–16 Specifically, studies show that sociodemographic factors are associated with prolonged time to diagnosis for a number of other cancers, while an unhealthy lifestyle is associated with longer intervals prior to diagnosis17–19 including gynaecological cancers.20 An enhanced understanding of the healthcare-seeking behaviour with gynaecological cancer alarm symptoms in different groups in the general population might improve policy interventions targeting early diagnosis of gynaecological cancer.
Therefore, the aims of this study were (1) to determine the proportion of women in the general population reporting recent onset of gynaecological cancer alarm symptoms with subsequent GP contact and (2) to analyse the associations between lifestyle factors, SES and contact to GP with gynaecological cancer alarm symptoms.
Methods
The study was conducted as a nationwide combined questionnaire-based and register-based study. It is a part of a larger study, the Danish Symptom Cohort (DaSC), that investigates the prevalence of symptom experiences and healthcare-seeking behaviour in the general population.21 In Denmark, 98% of citizens are listed with a GP. The GPs have a gatekeeping role in the healthcare system and with the exception of very few situations, patients do not have direct access to secondary care nor to specialist care in primary care. The Danish healthcare system is tax funded and provides free medical care for all in both primary care and hospital setting.22
Study subjects
For the survey (DaSC), a random sample of 100 000 adults aged 20 years or older was drawn from the Danish Civil Registration System (CRS), in which all Danish citizens are registered with a unique identification number. This identification number enables accurate linkage between national registers. The sampling procedure did not include individuals who had indicated in the CRS that they did not want to participate in research-related inquiries. Of the 100 000 invited individuals, 51 090 (51.1%) were women, and only data for the women are included in this paper.
The questionnaire
The questionnaire was designed using the internet-based platform SurveyXact, and the invited individuals received a unique 12-digit login by postal letter.23 This login had to be entered on a secure webpage in order to access the questionnaire. In order to prevent exclusion of people with no internet access, the participants were offered to complete the survey by telephone interview. Questionnaire data were collected from June to December 2012.
The development of the questionnaire followed standardised and widely recognised procedures and was pilot tested in its entirety for content validity, relevance, acceptability and feasibility. The final version of the questionnaire was field tested on 500 individuals, randomly sampled from the CRS prior to the survey. The data quality, response rate, floor and ceiling effects, score ranges of single items and scores were assessed. Additional details about the design of the study and the data collection process are described elsewhere.21
A comprehensive questionnaire concerning the experience of 44 predefined specific and non-specific cancer alarm symptoms, as well as general and frequent symptoms, was developed. The alarm symptoms were selected based on a review of literature including national and international cancer referral guidelines.24–28 This study focuses on four symptoms (pelvic pain, postmenopausal bleeding, pain during intercourse and bleeding after intercourse), as these are mentioned in cancer referral guidelines regarding gynaecological cancer.25 26 The respondents were asked whether they had experienced one or more of the symptoms within the preceding 4 weeks, when they had experienced the first onset of the symptom(s), and whether they had contacted a GP about the symptom(s). The wording of the question regarding symptoms was: ‘Have you experienced any of the following bodily sensations, symptoms or discomforts within the past 4 weeks? (Yes/no)’. A follow-up question for reported symptoms was phrased: ‘When did you experience these for the first time? (Less than a month ago/1–3 months ago/3–6 months ago/More than 6 months ago)’. The question regarding contacting a GP was: ‘Have you contacted your GP concerning the symptom(s) you have experienced within the preceding 4 weeks, through appointment, by telephone or email? (Yes/no)’. The questionnaire also included items about self-reported lifestyle factors, such as smoking habits and alcohol consumption. Respondents also reported their height and weight.
Patient and public involvement
Individuals from the general population only participated in the pilot testing and field testing of the questionnaire, and were otherwise not involved in the design of the study, research questions or other aspects of the survey, including recruitment and conduct of the study. The results of the study will be disseminated to the public by summaries in popular scientific magazines.
Register data
Information about SES and demographics was obtained from Statistics Denmark for each individual using the unique personal identification number in the CRS. Statistics Denmark is a governmental institution responsible for collecting and handling data from a number of social and administrative registers.29 Information about educational level, household income, labour market affiliation, cohabitation status and ethnicity was obtained via data linkage to this database for each respondent for the year 2011, the year before the survey.
Statistical analysis
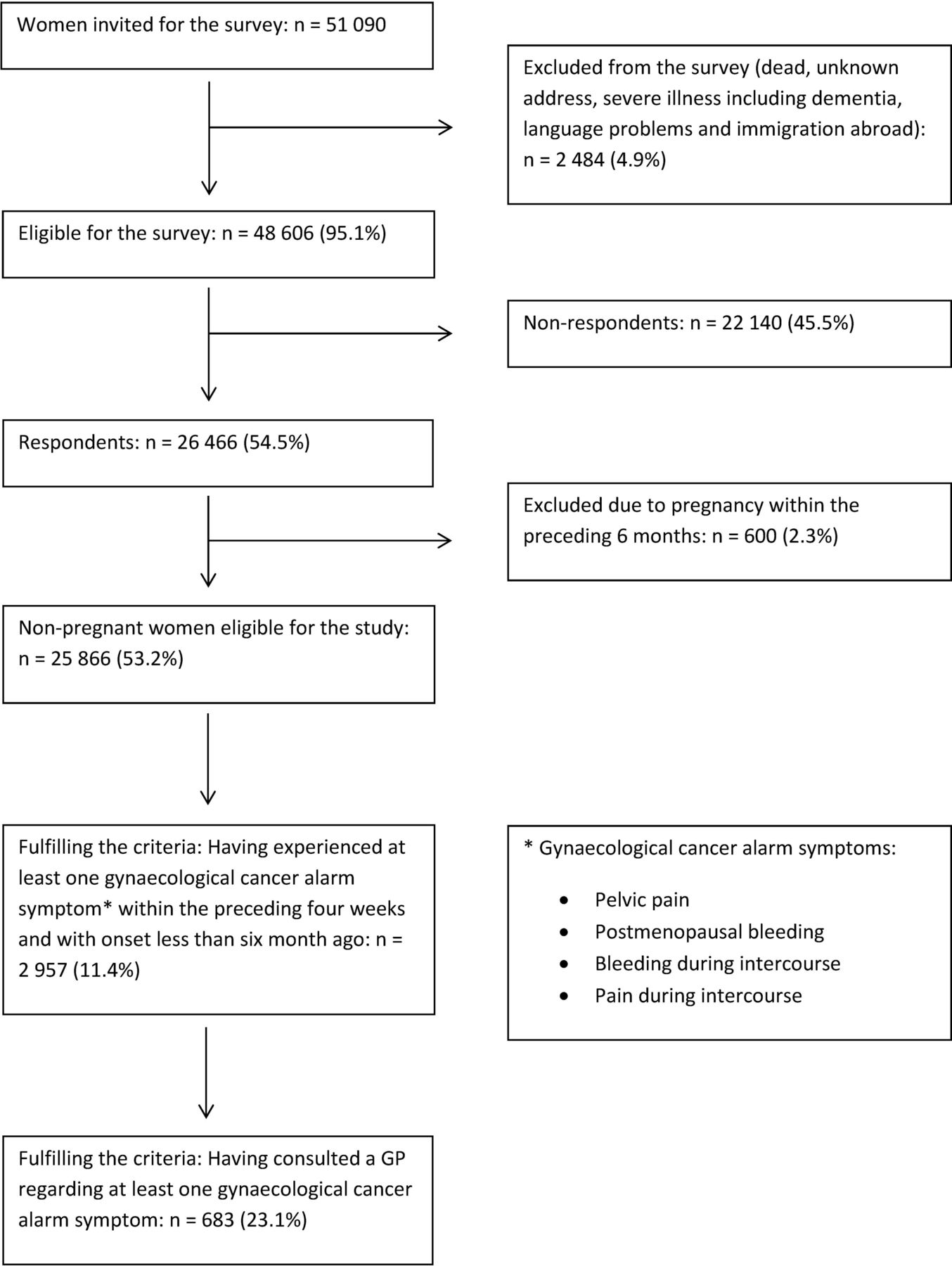
In order to explore how recently onset symptoms were managed, symptoms with onset more than 6 months ago were excluded. As pregnant women may display a different healthcare-seeking behaviour compared with non-pregnant women, individuals who stated that they were pregnant within the preceding 6 months were excluded from the analyses (figure 1).
{kind=link}
Study population. GP, general practitioner.
The proportions of women with recent onset of gynaecological symptoms and contact with a GP are presented as percentages for each symptom. CIs were calculated using binomial distribution. Logistic regression models were used to calculate unadjusted and adjusted ORs for associations between GP contact with at least one of the four cancer alarm symptoms and each of the covariates. A subanalysis was performed for those reporting postmenopausal bleeding and/or bleeding during intercourse, as these symptoms from a clinical perspective are considered as especially alarming thus prompting fast investigation. The variables considered for analyses were age group, smoking status, alcohol consumption, BMI, educational level, income, labour market affiliation, cohabitation status and ethnicity. All these were categorical, and if they showed a significant association with GP contact in the crude logistic analyses, they were included in the subsequent logistic regression models.
Age was categorised as follows: 20–39, 40–59 or 60+ years old. The BMI was calculated for each respondent who was then categorised as underweight (BMI <18.5), normal weight (18.5≤BMI<25), overweight (25≤BMI<30) or obese (BMI ≥30) according to WHO guidelines.30 Smoking status was categorised as never smokers, former smokers or current smokers. Alcohol consumption was categorised according to average intake (measured in units): 0, 1–7 units/week or >8 units/week. Education was categorised according to the highest attained educational level: low (<10 years, ie, primary and lower secondary school); middle (10–12 years, ie, vocational education and upper secondary school) or high (>12 years, ie, short-term, medium-term or long-term higher education).31 Equivalence-weighted disposable income was categorised as low income (first quartile), middle income (second and third quartiles) or high income (fourth quartile). The equivalent disposable income comprises all income (wages, salaries, benefits and pensions) after taxation for the entire household and is adjusted for number of persons in the household.32 Labour market affiliation was categorised as currently working, pensioner or out of the workforce. Cohabitation status was categorised as cohabiting/married or single. Ethnicity was categorised as people of Danish origin, immigrants (individuals not born in Denmark by parents who holding Danish citizenships) or descendants of immigrants (individuals born in Denmark by parents who are neither born in Denmark nor holding Danish citizenships).
All statistical tests used a significance level of p<0.05. Data analyses were conducted using STATA statistical software V.13.1 (StataCorp).
Results
A total of 26 466 women completed the questionnaire, yielding a response rate of 54.5% for the women. The median age of the participants was 51 years (IQR 39–63) compared with 53 years (IQR 37–71) for non-participants. A total of 600 (2.3%) stated that they had been pregnant within the preceding 6 months and were thus excluded from the analyses. A total of 2957 (11.4%) of the remaining 25 866 women reported at least one gynaecological cancer alarm symptom with onset within the preceding 6 months, figure 1.
The descriptive data for the study population are shown in table 1. The proportion of respondents reporting GP contact ranged from 21.1% for pain during intercourse to 32.6% for postmenopausal bleeding, table 2.
Descriptive data for the study population
Gynaecological cancer alarm symptoms within the preceding 6 months and self-reported contact to general practitioner (GP)
Among individuals reporting at least one of the four cancer alarm symptoms, no significant association with GP contact was found for BMI, smoking status, alcohol consumption, household income, educational level or marital status. Thus, the variables included in the adjusted logistic model were age group, labour market affiliation and ethnicity. In the full model, we observed that women in the age group 60+ years had higher odds of reporting GP contact compared with the youngest age group (OR 2.56, 95% CI 1.69 to 3.89). Likewise, immigrants had higher odds of reporting GP contact (OR 1.56, 95% CI 1.13 to 2.15) compared with ethnic Danish individuals, table 3.
Crude ORs and adjusted ORs for associations between lifestyle factors, socioeconomic status and contact to GP with at least one of the four cancer alarm symptoms (symptom experiences <6 months)
In the subgroup analyses among women reporting postmenopausal bleeding and/or bleeding during intercourse, we found no associations with GP contact for smoking status, BMI, alcohol consumption, labour market affiliation, household income, ethnicity or marital status. Women aged 60+ had higher odds of reporting GP contact compared with women in the age group 20–39 (OR 2.79, 95% CI 1.33 to 5.87). Furthermore, those with a high educational level (>12 years) had higher odds of reporting GP contact compared with those with a low educational level (<10 years) (OR 2.23, 95% CI 1.19 to 4.19), table 4.
Crude ORs and adjusted ORs for associations between lifestyle factors, socioeconomic status and contact to GP with postmenopausal bleeding and/or bleeding during intercourse (symptom experiences <6 months)
Discussion
Main findings
In this nationwide study comprising 26 466 women from the general Danish population, 23.1% of those reporting four specific gynaecological alarm symptoms with onset less than 6 months prior had contacted a GP with at least one of the symptoms. The proportion of GP contacts ranged from 21.1% (pain during intercourse) to 32.6% (postmenopausal bleeding).
Women in the oldest age group and immigrants had significantly higher odds of having contacted the GP when reporting at least one of the four symptoms. No associations were found with smoking status, BMI, alcohol consumption, labour market affiliation, household income, marital status or educational level. In the subgroup analysis of women reporting postmenopausal bleeding and/or bleeding during intercourse, higher age and a high educational level were associated with having contacted the GP. In this subgroup, no associations were found with labour market affiliation, household income, ethnicity, marital status or any lifestyle factors.
Study strengths and limitations
Strengths of this study include the large study sample (51 090 women) and the relatively high response rate (54.5% among women). An overall responder analysis of the entire study cohort including both genders showed that respondents were more often cohabiting, had higher educational level, had higher income, were of Danish origin and more were affiliated with the workforce.11
In Denmark, detailed socioeconomic and demographic data on an individual level are available, based on administrative data and defined in Statistics Denmark.31 32 The quality of these data is in general high and there is a low risk of misclassification.29
Some of the symptoms mentioned in guidelines are frequently occurring in the general population, and mostly caused by benign conditions, for example, normal menstrual cycle.8 As both the symptoms33 and gynaecological cancers are age dependent,34 exploring the healthcare seeking for each symptom in different age groups would be of great value. However, some of the symptoms were somewhat rare and analysing these separately with regard to the explanatory variables would be in violation with Danish legislation and data protection regulations. In a previous study based on the same population cohort, increasing age was found to be significantly associated with healthcare seeking regardless of symptom type, supporting that our finding regarding age may be due to other factors than the individual symptoms alone.35
This study is based on self-reported symptoms within a time frame of 4 weeks with onset less than 6 months prior to questionnaire distribution and GP contacts regarding these symptoms. Even though the time spans are relatively short, some memory decay cannot be ruled out, which may result in under-reporting of both symptoms and GP contacts. On the other hand, some individuals may have felt that the alarm symptoms should have led to GP contact, which may have resulted in desirability bias. The time for GP contact was not specified as the intention was to obtain information on all GP contacts.
Furthermore, it is important to keep in mind that the lifestyle factors (alcohol consumption, smoking status and BMI) are self-reported and may be under-reported, thus prone to information bias. However, it has been demonstrated that self-reported anthropometric data are reliable—especially among young people.36 37
Comparison with existing literature
It has been demonstrated that women lack knowledge about symptoms of gynaecological cancer and that they often attribute the symptoms to benign conditions,38 increasing age and simply being a woman.39 In hypothetical situations of experiencing gynaecological cancer alarm symptoms, many women hesitate to seek medical attention.40 Our study confirms that this is also the case when actually experiencing gynaecological alarm symptoms in real life.
Few studies have investigated the associations between healthcare seeking and lifestyle and sociodemography of individuals reporting gynaecological alarm symptoms. In a survey by Brain et al, higher educational level was significantly associated with delay for women in the hypothetical situation of experiencing gynaecological alarm symptoms.40 The different results in our study may be due to the fact that Brain et al explore a hypothetical situation with rather vague symptoms, compared with our study with truly experienced symptoms that are more specific of nature. In a study by Elliott et al 41, higher educational level was associated with higher degree of consulting the GP with both low-impact and high-impact symptoms, the tendency being more profound for high-impact symptoms. This supports our findings indicating that higher educational level is indeed positively associated with healthcare-seeking behaviour with gynaecological alarm symptoms of certain impact, as we only found the association for bleeding during intercourse and postmenopausal bleeding.
Another study based on the DaSC-survey has demonstrated that healthcare seeking with respiratory symptoms is significantly lower among smokers.42 This may be caused by the well-known association between smoking and respiratory symptoms, which may induce normalisation of, for example, coughing among smokers. Likewise, smokers may experience other barriers towards healthcare seeking such as fear of being blamed for their health conditions being caused by lifestyle. In our study, we did not find such an association, which may indicate that the association between lifestyle and healthcare seeking is specific for the symptoms in question and not generalisable to overall healthcare seeking.
Interpretation of findings
We evaluated whether social inequity existed with regard to GP contact with gynaecological alarm symptoms, and whether lifestyle influenced the healthcare-seeking process. In the Danish healthcare system, GPs act as gatekeepers and healthcare coordinators for their patients. A prerequisite for further investigations is, however, that patients seek healthcare when experiencing symptoms. We have demonstrated that healthcare seeking with gynaecological cancer alarm symptoms is positively associated with age, ethnicity and educational level. As the risk of cancer increases with age for both endometrial and ovarian cancer, higher proportions of healthcare seeking in the older age groups may be beneficial for detecting these cancers. On the other hand, cervical cancer is also frequently occurring among younger women, and means to promote more appropriate healthcare seeking in the younger age groups must be explored, especially taking into consideration that adherence to cervical screening is lower among younger women.43 This study found that higher educational level was positively associated with increased healthcare seeking, while no significant associations were found for lifestyle factors. This might indicate that educational level is a proxy for health literacy, and that the latter is the determining factor for healthcare-related actions rather than lifestyle. In a previous study, we found that higher educational level was positively associated with specialist investigation of gynaecological symptoms.44 When taking the results of the present study into account, the social inequality in healthcare utilisation may be even more profound than previously expected. As we found no associations with lifestyle factors, a central point of interest for researchers, clinicians and policy-makers should be the influence of sociodemographic factors on timely diagnosis of symptomatic individuals. At the same time, it must be kept in mind that most of the symptoms are attributable to benign and often normal conditions which poses a challenge for both clinicians, the healthcare system and the symptomatic women who may be exposed to extensive investigations with the risk of iatrogenic harm and psychological distress.
Conclusion
Less than one-third of women contact their GP with newly onset gynaecological cancer alarm symptoms. Higher age, being immigrant and a higher educational level increased the odds of GP contact. Especially the effect of educational level may contribute to social inequality in healthcare utilisation. Future studies should explore the reasons for these findings, and in the meanwhile, clinicians should be aware of patients at risk of not seeking help with symptoms, for example, younger women or women with lower education.
Acknowledgments
The Danish Symptom Cohort is conducted in collaboration between University of Southern Denmark and Aarhus University, and the project is imbedded in the research portfolio at the Research Centre for Cancer Diagnosis in Primary Care (CaP). The questionnaire, on which the study is based, was developed in collaboration with Rikke Pilsgaard Svendsen, Anette Fischer Pedersen, Rikke Sand Andersen and Peter Vedsted. The authors thank Maria Munch Storsveen for statistical aid and Merete Moll Lund for proofreading the manuscript.
References
Footnotes
Contributors KB, SE, SR and DEJ participated in the design of the study, development of the questionnaire, the logistics concerning the survey and the drafting of the manuscript. KB moreover did the main work in forming the manuscript and carried out the statistical analyses. JS participated in the design of the study, development of the questionnaire and drafting of the manuscript. RdC participated in the statistical considerations concerning the survey and analyses. PFH participated in the interpretation of the findings and drafting of the manuscript. All authors read and approved the final manuscript.
Funding The study is financially supported by the Region of Southern Denmark, the Novo Nordisk Foundation and the Danish Cancer Society.
Competing interests None declared.
Patient consent Not required.
Ethics approval The project was approved by the Danish Data Protection Agency (journal no. 2011-41-6651).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The datasets generated and analysed during the current study are not publicly available due to the data protection regulations of the Danish Data Protection, Statistics Denmark and the Danish Health and Medicines Authority. Access to data is strictly limited to the researchers who have obtained permission for data processing. This permission was granted to the Research Unit of General Practice, Department of Public Health, University of Southern Denmark.