Article Text

Abstract
Introduction Treatment-resistant schizophrenia (TRS) is a severe form of schizophrenia. In the European Union, approximately 40% of people with schizophrenia have TRS. Factors such as the persistence of positive symptoms or higher risk of comorbidities leave clinicians with a complex scenario when treating these patients. Intervention strategies based on mHealth have demonstrated their ability to support and promote self-management-based strategies. Mobile therapeutic attention for treatment-resistant schizophrenia (m-RESIST), an innovative mHealth solution based on novel technology and offering high modular and flexible functioning, has been developed specifically for patients with TRS and their caregivers. As intervention in TRS is a challenge, it is necessary to perform a feasibility study before the cost-effectiveness testing stage.
Methods and analysis This manuscript describes the protocol for a prospective multicentre feasibility study in 45 patients with TRS and their caregivers who will be attended in the public health system of three localities: Hospital Santa Creu Sant Pau (Spain), Semmelweis University (Hungary) and Gertner Institute & Sheba Medical Center (Israel). The primary aim is to investigate the feasibility and acceptability of the m-RESIST solution, configured by three mHealth tools: an app, wearable and a web-based platform. The solution collects data about acceptability, usability and satisfaction, together with preliminary data on perceived quality of life, symptoms and economic variables. The secondary aim is to collect preliminary data on perceived quality of life, symptoms and economic variables.
Ethics and dissemination This study protocol, funded by the Horizon 2020 Programme of the European Union, has the approval of the ethics committees of the participating institutions. Participants will be fully informed of the purpose and procedures of the study, and signed inform consents will be obtained. The results will be published in peer-reviewed journals and presented in scientific conferences to ensure widespread dissemination.
Trial registration number NCT03064776; Pre-results.
- treatment-resistant schizophrenia
- mhealth
- psychosis
- mobile device based intervention
- feasibility
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
To the authors’ knowledge, mobile therapeutic attention for treatment-resistant schizophrenia (m-RESIST) is the first mHealth platform specifically addressed to treatment-resistant schizophrenia.
The m-RESIST solution includes a sophisticated tool to detect early warning signs for preventing symptoms before they occur.
This study promotes the involvement of the caregivers in the therapeutic process and a closer monitoring and communication with clinicians.
The outcomes of this study will help in future performance of a cost-effectiveness randomised controlled trial.
The study focuses on feasibility and acceptability, so any differences found in outcomes should be treated with caution due to the design (small sample size, absence of control group, and the short length of intervention and follow-up period).
Introduction
Background
In the European Union, between 0.2% and 2.6% of the population suffer from psychotic disorders.1 The largest group is patients with schizophrenia, and around 20%–30% are patients whose condition does not respond satisfactorily to adequate treatment and clearly have harder-to-treat psychotic symptoms, despite adherence to current optimised treatment.2 These patients are referred to as patients with treatment-resistant schizophrenia (TRS).3 4 TRS is a complex phenomenon influenced by a great variety of schizophrenia subtypes, psychiatric comorbidity and coexisting medical illnesses. Such patients pose a challenge to psychiatric and primary care clinicians, generating a financial burden on society due to frequent emergency visits, hospitalisations and chronic use of polypharmacy.5 Moreover, there is also a huge impact in human terms with regard to patients and caregivers, involving several dimensions such as quality of life, treatment side effects, caregiver burden, social impairment and high mortality.6
Standard intervention in patients with TRS is challenging due to the persistence of positive symptoms, extensive periods of hospitalisation and elevated risk of somatic and psychiatric comorbidities. Improvement obtained by current drug therapy, such as clozapine alone or in combination with another antipsychotic/mood stabiliser, is frequently not effective enough to achieve remission in patients with TRS.7 Therefore, the development of innovative evidence-based interventions adjunctive to pharmacological and psychosocial treatment is needed.
Previous studies have shown feasibility, acceptability and also preliminary efficacy of mobile interventions (mHealth) for schizophrenia.8–14 Over 80% of participants indicated that they would recommend the interventions and that they were easy to use and useful, reporting also high levels of satisfaction. Intervention strategies based on mHealth have demonstrated their ability to support and promote self-management-based strategies in psychotic disorders.
Mobile interventions may be effective in preventing relapses, increasing treatment adherence and relieving some of the symptoms, though the effects on social functioning remain unclear.11 13 15 16 Smartphone ownership among people with schizophrenia is relatively high and increasing.17 Moreover, patients also seem to be willing and able to use smartphones to monitor their symptoms, engage in therapeutic interventions and increase physical exercise.9 Alvarez-Jimenez et al performed a meta-analysis of 12 studies, where evidence on acceptability, feasibility, safety and benefits of online and mobile-based interventions for psychosis were analysed.18 Results showed that 74%–86% of patients used web-based interventions efficiently, 75%–92% perceived them as positive and useful, and 70%–86% of patients completed or engaged with the interventions during follow-up. On the other hand, 26% of patients experienced difficulties in using web-based psychoeducation and cognitive behavioural therapy (CBT), the main causes being lack of motivation, poor engagement and poor understanding.18 It should be noted that the lack of published mHealth studies focusing on patients with TRS makes it more difficult to design novel interventions. Therefore, future mHealth studies in TRS should pay attention to some essential aspects: the recruitment process, the design and delivery of patient-centred and easy-to-use mHealth programmes, and strategies to maximise retention rates. Performing a feasibility study would be helpful to explore the acceptability and adequacy of intervention components, evaluate recruitment and assessment procedures, and to ensure if changes will be necessary during a subsequent cost-effectiveness randomised controlled trial (RCT).
This study protocol (version 1; dated 5 July 2016) is part of a European research project, cofunded by the Horizon 2020 Framework Programme of the European Union (grant agreement n° 643552). This project aims to develop and test the use of m-RESIST, a mobile system based on information and communications technology (ICT), addressed to empower patients suffering from TRS and to involve their caregivers. This platform offers a holistic approach to integrate psychiatric and psychological assistance, offering a better monitoring of patients through a personalised and optimised therapeutic process, promoting acceptance and self-management of the condition, and potentiating a proactive role of patients and caregivers in the therapeutic process.
As stated by Aranda-Jan et al,19 the main considerations for an effective mHealth project are an appropriate project design (adapted to the local context), the availability of technology and resources, the involvement of stakeholders and the implementation process in healthcare systems. According to these conditions, a qualitative study about the receptivity of patients with TRS, caregivers and clinicians towards possible m-RESIST components was performed during the first stage of the m-RESIST solution development. The hypothetic positive acceptability of the solution in terms of usefulness, increase of patient’s empowerment and social contact promotion was shown.10
The current study protocol corresponds to the second stage of the project, aimed at ensuring that the designed solution satisfies the needs of end-users. To explore this, a feasibility study will be performed in an environment as close as possible to real-life settings, where the m-RESIST prototype will be tested in the target group (patients, caregivers and clinicians).
Aims and hypothesis
The objectives of this study are:
To investigate rates of willingness to enrol, attrition (non-usage and dropout attrition) and compliance with the study.
To investigate the acceptability of the m-RESIST solution in patients with TRS, caregivers and clinicians.
To examine participants’ satisfaction and the usability of the m-RESIST solution.
To explore the suitability and availability of proposed clinical, functional and economic outcomes measures.
The hypotheses are:
The m-RESIST solution will have acceptable rates of willingness to enrol (≥70%), non-usage and dropout attrition (both <15%) in patients with TRS.
The m-RESIST solution will be highly accepted by patients with TRS and reflected in high scores in acceptability, usability and satisfaction reported by more than 80% of the patients.
The proposed clinical, functional and economic outcomes measures will be suitable and available for TRS.
Methods and analysis
The following methods adhere to the Standard Protocol Items Recommendations for Interventional Trials (SPIRIT) guidelines for the reporting of study protocols.20
Study design and setting
This is a prospective multicentre feasibility study, without a control group, following an iterative process in patients with TRS and their caregivers. Participants will be recruited from three sites: Gertner Institute & Sheba Medical Centre, Psychiatric Division (Tel Aviv, Israel); Semmelweis University, Department of Psychiatry and Psychotherapy (Budapest, Hungary), and Hospital de la Santa Creu i Sant Pau-D of Psychiatry (Barcelona, Spain). These sites provide full-spectrum mental health services to adult people from their catchment area and have wide experience in participating in large-scale clinical trials in patients with schizophrenia.
Participants
A total of 45 patients with TRS (15 per centre), with their caregivers, will be selected for invitation to participate by researchers. The eligibility for participation will be based on the inclusion and exclusion criteria in table 1.
Inclusion and exclusion criteria for the study
Due to the voluntary nature of participation in clinical trials, participants may leave the study without having to specify their reasons. The investigators could also dismiss a participant from the study whenever they consider it appropriate.
Reasons for withdrawal include events such as inpatient psychiatric hospitalisation. A participant will be withdrawn from the study participation if she/he:
Refuses to cooperate.
Wishes to drop out (in this instance a specific reason must be recorded by the investigator).
Experiences adverse events sufficiently severe that, in the opinion of the investigator, it would be harmful to continue in the study.
Has a general medical condition that, in the opinion of the investigator, would make it harmful to continue in the study.
Does not complete the study as outlined in the study protocol.
Intervention
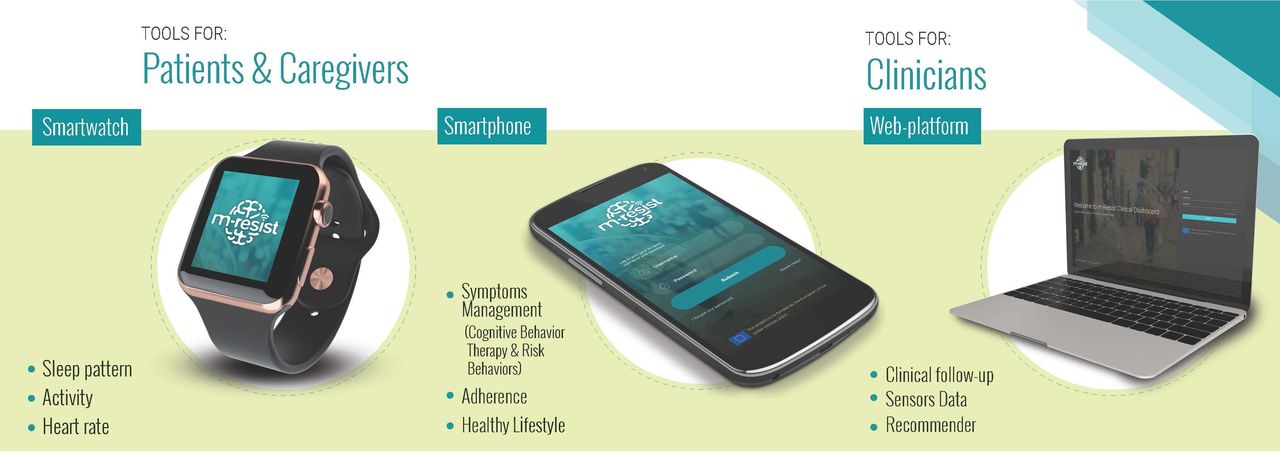
In the current study, the intervention will involve patients and their caregivers, and the main actors involved in the deployment of the m-RESIST solution will be a psychiatrist, a psychologist and a case manager. The key aim of the intervention delivered by the m-RESIST solution is to engage patients with TRS, together with their caregivers, in an active participation in therapeutic processes, and empower them to enable the self-management of their condition. To achieve this objective, the intervention is supported by three mHealth tools: a wearable (smartwatch), a mobile app and a web-based platform (see figure 1). Patient compliance will be measured by the number of days that the m-RESIST was used during the 3 months of intervention. Data for usage will be captured automatically by the m-RESIST software.
{kind=link}
mHealth tools of the m-RESIST solution. m-RESIST, mobile therapeutic attention for treatment-resistant schizophrenia.
The functionality of the smartphone is based on the m-RESIST app. Through this app, patients will have access to educational content about TRS condition and related issues; track their early warning signs (EWSs), symptoms and biological variables; ask for help by questionnaires or the ‘alarm bottom’; receive and practice helpful CBT-based coping strategies and exchange messages with their caregiver or healthcare provider.
The wearable is a smartwatch that will collect data from patients and send it wirelessly to the smartphone. Sensor data will be recorded through automatic passive upload. The variables collected will be level of activity, heart rate, sleeping pattern and steps counter.
The web-based platform is the tool that the healthcare providers (case manager, psychiatrist and psychologist) will use to collect assessment data, to monitor patients’ state and review data collected by sensors, to communicate by texting with patients, caregivers and other professionals, and to consult recommendations (based on guidelines and experts’ opinion).
The m-RESIST intervention has been designed in order to meet the following assumptions:
It focuses on key problems: before starting the m-RESIST intervention, the patient’s early EWSs and current problems will be assessed. There will be two outputs. First, the patient’s relapse signature configured by the three main EWSs presented by the patient before a worsening occurs. Each EWS will be linked with a predefined (based on CBT) or tailored (based on patient’s experience) coping strategy. These strategies will be triggered as a recommendation through the app when patients express distress or the system detects risk of worsening. The second output will be the treatment plan which will identify the three main problems and corresponding goals in the patient’s life, and link these goals with a specific module of intervention. This process will be agreed between patient, caregiver and clinician.
It is modular and tailored to the patient’s condition: two categories of interventions have been designed, basal and risk intervention (see definition and characteristics in table 2). They are related with the list of problems mentioned previously, in order to set the most appropriate intervention depending on the patient’s situation.
m-RESIST modules of intervention
It is capable of detecting worsening: the m-RESIST intervention is capable of changing the system’s triggers to patients when worsening is detected by means of the baseline sensor and clinical profiles. During a 15-day period, the patients will use the smartwatch and the smartphone to capture continuously multidimensional sensor data. The baseline sensor profile will be based on the analyses of these data. Furthermore, a complete assessment of clinical variables (eg, symptoms, risk behaviours, functionality and adherence) will also be performed in this period. The baseline clinical profile will be based on the analysis of these data. A set of predefined algorithms will detect significant changes in predefined thresholds, and trigger specific questionnaires, recommendations and notifications. Whenever a moderate or high risk of an oncoming episode of worsening is detected, the clinical team will be alerted, and the patient will be offered tailored recommendations or emergency assistance.
Concomitant therapy: Apart from the intervention associated with the m-RESIST solution, patients will keep receiving their treatment-as-usual (including outpatient case management, linkage to services and medication monitoring). If it is necessary to make changes in the psychiatric treatment, they will be recorded in the patient profile created in the platform.
Outcomes
The evaluation framework to understand the factors affecting the user experience and acceptance of the m-RESIST solution among various stakeholders, as well as the main determinants affecting user experience at a feasibility level, will follow the living lab approach.24 It is defined as ‘a user-centric research methodology for sensing, prototyping, validating and refining complex solutions in multiple and evolving real-world contexts’. Living lab research goes beyond mere usability studies and acceptance studies, as it also takes the impact of the context of use into account. A multimethodological approach, with both qualitative and quantitative methodologies, is chosen so as to be able to capture different aspects of the implemented solution.
The protocol diagram based on SPIRIT guideline20 provides an overview of the measures used in the trial and their time points (see table 3). In addition to outcomes described in table 3 and below, sociodemographic and clinical characteristics (eg, years of evolution, past and current treatment, comorbidities) will be collected by using a semistructured interview.
Schedule of study protocol periods and assessments
The primary and secondary outcomes (see table 4) of the study protocol are the following:
Baseline assessment and outcome measures
Primary outcomes
The primary outcomes include feasibility and acceptability of using the m-RESIST solution. Qualitative and quantitative feedback will be collected to identify the main determinants of experience and acceptance of the m-RESIST solution.
Feasibility will be examined by analysing willingness to enrol, attrition and compliance. The measures and operational criteria are as follows:
Willingness to enrol: the proportion of patients approached about the study that proceed to the consent stage. Operational criteria definition: ≥70% of patients approached will agree to enrol.
Attrition25 26: two measures will be collected, dropout and non-usage attrition.
Dropout attrition: proportion of participants who fail to complete the study protocol and thus do not complete the study assessments. Operational criteria definition: <15% of participants will be lost to follow-up or withdraw from the study.
Non-usage attrition: proportion of participants who do not drop out (eg, who are still completing the follow-up), but who stop using the m-RESIST tools (smartwatch, app). Operational criteria definition: <15% of participants will stop using devices
Compliance: extent to which participants experience the content of the m-RESIST intervention, measured by number of logins, time spent online, number of questionnaires completed, number of messages sent and answered and number of successful appointments.
Acceptability of the m-RESIST solution will be assessed in terms of acceptability, usability and satisfaction in patients with TRS, caregivers and clinicians. Critical measures are the following:
Acceptability: a modified version of the Technology Acceptance Model (TAM) scale,27 adapted to patients with TRS by the research team, will be used. The following variables will be evaluated: perceived usefulness, perceived ease of use, intention, compatibility, subjective norm, facilitators and habit. Each variable is composed of a series of Likert-type items (seven levels, from ‘totally disagree’ to ‘totally agree’). Data will be collected at the end of the intervention (V7).
Usability: two instruments will be used, User Experience Questionnaire and Interval Question. The User Experience Questionnaire will be delivered by online data collection (Qualtrics software) and is composed of a combination of survey questions (4-point Likert-type scale) and open questions. The survey will explore perceived ease of use, perceived usefulness, attitude and perceived quality of content. The open questions will explore lasting impressions and recommendations. The participants will be asked to complete the questionnaire on three occasions during the 3-month intervention: at the start (V0), in the middle (V3) and at the end of the intervention (V7).
The Interval Question, aimed at better capturing a more constant experience of the participants, will ask always the same question: What is it like to use the m-RESIST solution? It will be sent to participants via m-RESIST message system once a week, but on different days and at different times.
Satisfaction: this variable will be assessed using the Client Satisfaction Questionnaire-8.28 This instrument will be completed at the end of the intervention (V7).
Secondary outcomes
A complete clinical and economic evaluation would be premature in this feasibility study, due to the small sample. However, it will be useful to collect necessary parameters for planning a full prospective RCT to test the cost-effectiveness of m-RESIST solution.
Completion rates and missing data will be explored. Operational criteria definition for missing data: <10% of each set of secondary outcomes is missed during study data collection.
The measures for clinical, functional, quality of life and economic outcomes are the following:
Clinical outcomes
Severity of symptoms will be assessed using the instruments Positive and Negative Syndrome Scale (PANSS),29 Calgary Depression Scale (CDS)30 and Clinical Global Impression-Schizophrenia (CGI-SCH).31 PANSS and CDS will be completed on two occasions, at the start (V0) and at the end (V7) of the intervention. CGI-SCH will be rated in all protocol visits (V0–V7).
Insight will be assessed using the instrument Scale Unawareness Mental Disorders.32 This scale will be administered on two occasions, at V0 and at V7.
Adherence will be assessed using the Adherence to Refills and Medications Scale.33 This instrument will be administered on two occasions, at V0 and at V7.
Functional and perceived quality of life outcomes
Functionality will be assessed using the instruments Global Assessment of Functioning (GAF)34 and Social Functioning Scale (SFS).35 GAF and SFS will be administered on two occasions, at V0 and at V7.
Perceived quality of life will be assessed using the EuroQol 5 dimensions 5 levels questionnaire.36 This instrument will be administered on two occasions, at V0 and at V7.
Economic and organisational outcomes
Questionnaires with open ad-hoc questions and semistructured interviews will be used to assess the use of resources (eg, unit cost of personnel of remote or face-to-face visits, number of emergency admissions and length of stay) and the impact of m-RESIST in organisation (questions regarding effects on the structure, work process and the culture of the organisation). This information will be gathered at V0 and V7.
Safety measures
Finally, safety measures will also be collected throughout the study. The presence of serious and non-serious adverse events, defined as any clinical change or illness reported during the study, will be monitored in every clinical visit. The adverse events observed when carrying out the study, either by the clinician or by the patient himself/herself and regardless of the causality relationship ascribed, will be recorded in the clinical records and at the patient’s dashboard.
Participant timeline
The study will consist of four periods: recruitment, preintervention, intervention and follow-up.
Recruitment period, aimed at contacting and checking the eligibility of candidates. The outputs of an in-depth report about healthcare routes and clinical pathways in the three participant regions, made within the context of the m-RESIST project, have helped to identify the strengths and weakness of the recruitment capabilities. In order to reach the total sample of participants, two recruitment strategies will be used. Leaflets to promote the study will be distributed to healthcare providers, informing them about the study and inviting them to contact the research staff if potential participants are identified. In addition, research staff at the recruitment sites will approach eligible patients directly to suggest participating in the study. Informed consent signature for patients with TRS and caregiver will be obtained if inclusion and exclusion criteria are met, and both patient and caregiver agree to participate in the study.
Preintervention period (V0), aimed at training the participants in using the smartwatch and the app, and collecting clinical and sensor baseline information. At the beginning of the preintervention period, patients will be given the study smartwatch and smartphone, with m-RESIST app preinstalled. Caregivers will be given permission to install the app in their own smartphone. Both will be trained by the research staff in how to use the functions of the smartwatch and the different features of the app. Research staff will also provide patients and caregivers with training material (user guide and online video tutorial). Patients will be asked to wear the smartwatch for a period of at least 15 days, in order to collect enough sensor data to establish the baseline sensor profile. Furthermore, patients and caregivers will also be encouraged to use and familiarise themselves with the app by consulting the educational content and using the messaging system. Patients will also attend a clinical assessment, where secondary outcomes will be collected (see table 3). At the end of the preintervention period, the key elements (relapse signature and treatment plan) to deliver a tailored intervention will be explored.
Intervention period (V1–V7) aimed at testing the features and action flows that configure the m-RESIST interventions, and at assessing the experience of participants. At the beginning of the intervention, the treatment plan will be defined and the corresponding basal intervention will be activated. Participants will use the solution over 3 months, and appointments with clinicians will be scheduled every 15 days. This period will comprise four online visits and three onsite visits. In each visit, the treatment plan will be reviewed, the CGI scale and measure of patients’ perceived health status will be assessed and changes in the current antipsychotic treatment and potential adverse events will be explored. At the end of this period, a final visit will be held, made up of the full global assessment, to get post-test measures of the variables assessed in the preintervention period (see table 3).
Follow-up period, aimed at evaluating the primary and secondary outcomes of the study.
Sample size
This protocol study is a non-randomised feasibility study where the primary outcomes are not measures of intervention effects, but factors that could affect the successful execution of RCT. The proposed sample size of 45 patients, with their corresponding caregivers, is consistent with the recommendations for feasibility studies.37 38
Data analysis
Descriptive statistics (means and SDs or percentages) will be used to summarise baseline sociodemographic and clinical characteristics of participants.
Analysis of primary outcomes
Descriptive statistics will be used to ascertain feasibility. Willingness to enrol and attrition components will be summarised for participants, overall and in relation to selected baseline characteristics. Differences between followed up patients and those who were lost to follow-up will be examined in terms of baseline characteristics, by a paired sample t-test (normal distribution) or Wilcoxon signed-rank test (non-normal distribution).
Quantitative and qualitative data for acceptability and usability will be examined:
Quantitative data: each variable measured in acceptability and usability configured a Likert scale. The composite score (mean) of each variable will be calculated and treated as an interval/ratio scale. Pearson correlations between the constructs will be calculated to explore the following hypotheses: perceived usefulness and perceived ease of use is positively and significantly correlated to attitude; perceived ease of use is positively and significantly correlated to perceived usefulness; perceived quality of content will influence perceived usefulness and ease of use. Repeated measures of the User Experience Questionnaire will be tested by repeated measures analysis of variance method.
Qualitative data: for the analysis of self-reported data collected from User Experience Questionnaire and from Interval Question, qualitative thematic/content analysis will be conducted as proposed by Mayring.39 This method is a technique of summarisation, whereby themes are created in an inductive procedure by reducing, paraphrasing and generalising relevant text passages. Patterns in the text will be found and coded in order to search for themes in the data. The data will be subjected to thematic content analysis with the help of Atlas-ti software.
Finally, descriptive statistics will be used to assess satisfaction with m-RESIST intervention.
Analysis of secondary outcomes
Descriptive statics will be used to explore the availability and utility of data relating to proposed clinical, functional and economic outcomes measures, and a range of summary measures will be presented in the final statistical outputs.
Statistical analysis
Analyses will be conducted using STATA V.13. Descriptive statistics will be used to summarise clinical and demographic characteristics of patients. Feasibility of trial procedures will be examined using proportions and 95% CIs for assessments of feasibility and acceptability in terms of recruitment, consent, dropout, follow-up and integrity of double blinding. The variance observed in this sample will be used for sample size calculation for the future RCT, as recommended by Lancaster and colleagues.40
Quality control
The researcher will ensure the accuracy and integrity of the data and reports required. The data included in the m-RESIST derived from source documents will be consistent with such documents; otherwise, the discrepancies will be justified. The researcher will keep the study documents for at least 5 years after the study is completed.
Data monitoring will be done by the ethics committee of each site. Clinicians will have all the study-related files available, allowing direct access to data or source documents to perform monitoring, audit, review by the ethics committee or any inspection by the competent authorities. All data collected will only be accessible to m-RESIST partners.
Ethics and dissemination
Before entering the study, all participants will be legally competent and will provide written informed consent to the clinical team. All the data collected will be treated confidentially and analysed anonymously. Any protocol amendments will be made through the ethics committee of each site. The results of this study will be published in international peer-reviewed journals. A wide dissemination of the project results is planned to take place at European and international level. Patients, caregivers, health professionals, institutions and stakeholders will be targeted as the main recipients of the m-RESIST outcomes.
Study status
At the time of writing, the m-RESIST solution was still being tested by technological and clinical partners belonging to the project’s consortium, and potential participants were being assessed.
Discussion
This article summarises the protocol of a multicentre feasibility study aimed at assessing rates of attrition and acceptability of the m-RESIST solution. This information will provide important parameters to consider running a cost-effective RCT, and to identify potential constraints and possible solutions.
TRS is a complex phenomenon usually excluded from RCT. Our research group, made up of experienced clinicians and researchers in TRS patient follow-up, is interested in understanding the factors that lead to resistance or response in this patient population, and in developing new approaches to treatment.
The m-RESIST project targets the ‘high end’ (in terms of severity) of psychiatric morbidity–TRS, which is characterised by a chronic and continuous prolonged course, low level of adherence, insight and judgement, and is particularly challenging also due to impairments in interpersonal communication. These challenges reduce the possibility of the patients’ taking full responsibility for their treatment and self-care, and communicating their needs and changes in clinical state. The TRS multidimensional presentation, diverse course and multidimensional functioning impairment require treating patients with TRS by a multidimensional approach, including multidisciplinary teamwork and different interventions.
Current trends in treating schizophrenia result from general social trends and recent developments in medical care, including implementation of evidence-based medicine tools and novel technological developments in the field of healthcare, specifically regarding data collection using various sensors, data processing and communication. Healthcare systems are also moving towards personalised medicine, combining a large body of personal and disease-related information. The aforementioned view of heterogeneous complicated needs of patients with TRS, their caregivers and treating clinicians emphasises the need for a comprehensive system that will allow and encourage different modes of communication between potential users involved in the clinical complexity of the disease.
The m-RESIST solution is an initiative targeted to create a hybrid system aimed at optimisation of chronic care by integrating technological solutions, and assisting clinicians in their decision-making process. The developed solution also enhances the involvement of patients in their own treatment process, encouraging active participation in therapeutic processes, self-managing of their condition, thus reinforcing a sense of empowerment and improving quality of life.
The novel principles include new technology, high modularity and flexibility, and personalised response to heterogenic needs. In order to overcome the disadvantages of the current healthcare system, the m-RESIST solution intends to provide continuity of care, immediate attention for prevention of worsening and hospitalisations, automated and personalised interventions and recommendations, as well as easy and efficient communication between the solution users.
The main limitations of the study are those characteristic of feasibility studies, the lack of randomisation and a control group. It may have a high dropout rate, so predictors of discontinuation should be assessed comparing characteristics of compliant patients with those who were lost to follow-up. Furthermore, studies in mHealth require a minimum range of skills to use the tools. In this regard, patients with TRS can present limitations in using the devices due to some degree of cognitive impairment, and caregivers might have a poor knowledge of the internet, computer and other devices due to their age range.
However, and despite the aforementioned limitations, the findings and outputs from the proposed study will take us closer to designing a future cost-effectiveness trial in treatment-resistant patients.
References
Footnotes
AA-S and KR contributed equally.
Contributors AA-S and KR wrote the first draft of this study protocol. EMG and IC conceived the idea of the study and participated in the design of the solution. EJ, MI and AS served as advisors in this project and provided their expertise in studies in schizophrenia. VAV and JCM provided their expertise in quality and health assessments. AC, ZU and KF collaborated in the development of the intervention. SVdG, MS and TC collaborated in the definition and creation of the technological solution. EH-R and SM-G collaborated to the writing of the manuscript. JB and MH served as coordinators of the study. All authors contributed to the revising of the manuscript and writing of the final version of the manuscript, and gave their approval for the submission.
Funding This work has been supported by the Horizon 2020 Framework Programme of the European Union (grant number 643552) and partly funded by FEDER funds of the EU and CERCA Programme/Generalitat de Catalunya. Trial Sponsor: Institut de Recerca de l’Hospital de la Santa Creu i Sant Pau–IIB Sant Pau, Spain.
Competing interests None declared.
Ethics approval The study protocol has been approved by the local research ethics committee of each site: Gertner Institute (Tel-Aviv, Israel), Semmelweis University (Budapest, Hungary) and Hospital de la Santa Creu i Sant Pau (Barcelona, Spain).
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Francisco Alcalde, Enrico d’Amico, Caritat Almazán, István Bitter, Walter Baccinelli, Chiara Bonizzi, María Bugheroni, Xavier Constant, Marisol Escobar, Kata Fazekas, Emmanuel Gimenez, Charlotte Jewel, Teija Juola, Timo Jämsä, Rachelle Kaye, Alejandro Keymer-Gausset, Panagiotis Kokkinakis, Hannu J Koponen, Gregoris Mentzas, Jouko Miettunen, Jani Moilanen, Susana Ochoa, Ilias Papas, Fotis Paraskevopoulos, Elisabeth Reixach, Alexandra Roldán, Elena Rubio-Abadal, Garifalia Sebú, Jussi Seppälä, Valentina Simonetti, Vittorio Tauro, Anna Triantafillou, Judith Usall, David Vermeir, Ilaria de Vita.