Article Text

Abstract
Introduction Accessibility to healthcare services is a major concern facing migrant agricultural workers (MAWs) in the USA. We aimed to test the feasibility of implementing cardiovascular risk screening at farm sites.
Methods This was a pilot prospective cohort study providing on-site monthly screenings of cardiovascular risk factors. We estimated the prevalence of cardiovascular risk factors and evaluated the success of this approach via modified validated satisfaction surveys.
Results We enrolled 38 MAWs and diagnosed 18 cases of pre-diabetes, diabetes, hypertension and hyperlipidaemia in 15 subjects (39.4%). Mean scores of workers’ satisfaction were high (≥4) on a 5-point scale except ‘Time spent with provider’. Over 80% of workers were likely to use this model if it was permanently available on the farm. Only 8.7% of workers were able to follow up after referral to a clinic.
Conclusions Cardiovascular risk factors are highly prevalent in MAWs. On-the-farm screening is a feasible and satisfactory model of healthcare delivery; however, other barriers continue to hinder MAWs from receiving follow-up care.
Trial registration number NCT02418637. Results.
- migrant worker
- accessibility of health services
- cardiovascular disease
- diabetes mellitus
- feasibility study
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- migrant worker
- accessibility of health services
- cardiovascular disease
- diabetes mellitus
- feasibility study
Strengths and limitations of this study
Prospective outreach study design with an underserved population.
This study introduces a novel approach of healthcare delivery in the farming industry.
Pilot study with a small sample size.
Potential selection bias.
Introduction
The production of agricultural products in the USA has been dependent on hand labour provided by migrant agricultural workers (MAWs). Since the early 1900s, MAWs have become a distinctive entity of the work force in the USA. The Department of Labour defines a migrant farmworker as “a seasonal farmworker who had to travel to do the farm work so that he/she was unable to return to his/her permanent residence within the same date”.1 Estimates of the numbers of MAWs in the USA vary enormously. The National Agricultural Workers Survey in 2010 estimated over 3 million migrant and seasonal farmworkers in the USA,2 3 with 75% of them born in Mexico and around 42% entered the USA within the 5 years prior to survey.4 MAWs are predominantly men with only one in five workers is a woman and 1 in 20 is under the age of 18.5
Cardiovascular risk factors, including obesity, type 2 diabetes and hypercholesterolaemia, are more prevalent in the MAWs and Hispanics than the general US population. While US Hispanics have similar or lower rates, MAWs were found to have higher prevalence of hypertension than non-Hispanic whites. Moreover, control of these chronic health conditions is poorer in the Hispanic population in general, causing greater disease complications.6–11 More importantly, MAWs perceive their health status as significantly poor9 and healthcare delivery to MAWs remains suboptimal, particularly for primary healthcare and preventive services.5 12 13 Some of the barriers for accessing healthcare services are similar to those experienced by other immigrant Hispanic communities in the USA, including cultural and linguistic differences, low educational attainment, and financial and medical insurance challenges. Other barriers unique to MAWs are frequent mobility, residence on or close to farms with inadequate transportation, irregular employment and working long hours (25% reported working 50 hours or more/week).5 14
Legislation in the 1960s provided funding for a national system to facilitate healthcare delivery for MAWs in devoted clinics that usually offer income-based sliding scale fees and bilingual staff. Mobile clinics have been another solution to improve accessibility.15 Some programmes attempt more organised campaigns offering advanced screening (eg, mammography, bone density and respiratory diseases). Nevertheless, the lack of reliable transportation and inability of workers to leave job duties remain as significant barriers.16–19
Considering all these challenges, different healthcare delivery models are needed. Health screening at the worksite is one possibility to reduce some of these barriers and has been evaluated and proven to be associated with high degree of acceptability and adherence for up to 2 years.20 21 However, such reports targeted urban workers, not MAWs. To our knowledge, there has been no research evaluating cardiovascular risk factor screening in MAWs at their worksite (on the farm). Therefore, we have conducted this pilot prospective study to evaluate the feasibility and acceptability of performing biometric and cardiovascular screening on the farm.
Methods
Study design and sample selection
We designed a 6-month prospective cohort study with monthly visits to farm sites for testing blood pressure, glucose, lipid panel and weight. Surveys of feasibility and satisfaction were delivered at the end of the study period. We collaborated with the University of Minnesota Extension Program in Southeast Minnesota to reach out to farms listed in their database. We sent an email message to eight farms in the region outlining the research question, setting, population and timeline. Two dairy farms expressed interest in participation, one in Lewiston MN (total 11 workers) and the other in Canon Falls MN (total 15 workers). A third farm in St. Charles MN (20 workers) expressed interest after referral from one of the participating farms. After initial introductory visits to the farms, farms owners agreed to participate and introduced the project to their workers. Participation was voluntary and all participating workers signed a consent form.
Patient and public involvement
There was no patients’ or public involvement in this pilot study.
Inclusion and exclusion criteria
We included male and female adult (18 years and older) migrant workers who were directly involved in agricultural work at farm sites. We excluded workers who were not directly involved in agricultural work (eg, accountants, administrative, etc).
Data collection
Demographics
On the initial visit, all participants filled out a basic demographic questionnaire that also included information about their cardiovascular medical history (hypertension, diabetes and hyperlipidaemia), smoking status, level of education and family size as well as years of working on their current farm and in farming in general.
Cardiovascular risk factors
A bilingual staff was available at all times. Using Clinical Laboratory Improvement Amendments–waived testing, the study principal investigator measured participants’ blood pressure, glucose, cholesterol and HgA1C. Blood pressure was measured monthly using OMRON (OMRON Healthcare, Lake Forest, Illinois, USA). Blood glucose and cholesterol were also assessed monthly using CardioChek (PTS Diagnostics, Indianapolis, Indiana, USA) with PTS Panels test strips. Glycated haemoglobin was tested every 3 months using A1CNow (PTS Diagnostics). Weight was measured monthly using EatSmart scale (Health Tools LLC). Testing took place at a room designated by the farm owner (break room or meeting room) ensuring privacy and access to all participants. Testing took 15–20 min for each subject and was coordinated between farm owners and workers at each farm to avoid work interruption. A picture of the screening station is illustrated in figure 1.

Screening station.
Blood pressure was measured in the sitting position, in the right arm (when possible), after a 5 min rest. Abnormal blood pressure was considered with systolic pressure ≥140 mm Hg or diastolic pressure ≥90 mm Hg on two consecutive monthly visits. Random blood glucose and cholesterol were measured with fingertip samples. Abnormal glucose and total cholesterol were considered with values ≥200 mg/dL for both. Haemoglobin A1C was reported as normal if ≤5.7%, pre-diabetes if 5.8%–6.4% and diagnostic of diabetes if ≥6.5%. Body Mass Index (BMI) was calculated by dividing a participant’s weight (kg) by their squared height (m). Subjects with BMI 18.5–24.9 kg/m2 were considered normal weight, 25.0–29.9 kg/m2 overweight and ≥30.0 obese.
Follow-up
Participants with known or new diagnoses of hypertension, diabetes or hyperlipidaemia were referred for follow-up. Those who indicated having a personal physician were advised to follow up with their physician to discuss any new findings. Others with no primary care physician were referred to the Migrant Health Clinic in Rochester MN, which usually provides services to MAWs (and local underserved Hispanic population in general), and appointments were facilitated by study staff. We provided educational materials regarding basic lifestyle modifications to patients with newly diagnosed and borderline conditions (eg, DASH diet for hypertensive patients, normal body weight measures and dietary/exercise recommendations for overweight and obese patients).
Feasibility and satisfaction
After completing the study, each participant was asked to fill out the modified validated patient satisfaction questionnaire (PSQ-18) that evaluates seven different dimensions of satisfaction with medical care: general satisfaction, technical quality, interpersonal manner, communication, financial aspects, time spent with provider, and accessibility and convenience. PSQ-18 is a widely used validated method for measuring recipient’s satisfaction with medical service. In 18 questions and less than 5 min to complete, these seven areas of satisfaction are assessed with 5-point Likert scale and each area is scored by the average of its multiple questions (with 4–5 reflecting high, 3 moderate and 1–2 low satisfaction)22 (online supplementary tables Ia and Ib).
Supplementary file 1
Participants were also asked to complete a short survey we developed asking them about the testing site as well as any concerns of employment insecurity as a result of the screening and if they would adhere to and/or recommend this model to other workers (online supplementary table II). Farm owners were also asked to reflect on their experience, difficulties in accommodating screenings and thoughts about the model’s impact on workers’ health and business improvement. Feasibility was evaluated by assessing participants’ satisfaction, adherence and the likelihood of workers and farm owners to adopt the new model of healthcare delivery.
Statistical analysis
Data were entered in Microsoft Excel and analysed using SPSS (released 2009; PASW Statistics for Windows V.18.0). Categorical variables were presented as frequency and percentage. Continuous variables were presented as means±SD or median (range). Data were stratified based on gender, level of education and family size. We used a non-parametric Mann-Whitney U test to identify the difference between two groups with a two tailed p value of <0.05 indicating statistical significance.
Results
Baseline characteristics of the participants
A total of 38 workers consented to participate in the study of which 30 (79%) completed the 6-month follow-up. The remaining eight (21%) were all lost to follow-up due to turnover of migrant workers on the three farms. The majority were men (32) and median age was 30 years. Twenty-six workers (69%) reported ending their education in middle or high school, while the rest were elementary school educated and only one worker graduated high school. Only three workers (10%) identified themselves as English proficient. In terms of baseline health, 29 workers (71%) were either overweight or obese and seventeen (45%) were active smokers. Table 1A summarises participants’ baseline characteristics.
Baseline characteristics of participants
Cardiovascular risk factors in MAWs
Over a 6-month period, screening detected 14 cases (36.8%) of pre-diabetes, 2 cases (5.3%) of diabetes, 1 case of hypertension (2.6%) and 6 cases of hyperlipidaemia (15.8%). Prevalence and incidence of these risk factors are outlined in table 1B. Of note, the one case of hypertension was symptomatic (worker reported feeling fatigued and short of breath at times). He was referred to the Migrant Health Clinic in Rochester, MN, but unfortunately he failed to show up for the appointment and was lost to follow-up in the study. All newly diagnosed cases were counselled and provided with educational materials about their conditions. They were all referred to the Migrant Health Clinic; however, only two patients (8.7%) were able to follow up in clinic and two others with their primary care physician. The rest either did not have the time or the clinic was too far for them to follow up.
Prevalence and newly diagnosed cases of cardiovascular risk factors
Satisfaction and feasibility of MAWs with screening service
Different areas of participants’ satisfaction are presented in table 2. Subjects reported high satisfaction with scores above 4 on six of the seven tested areas including general satisfaction, technical quality, interpersonal manner, communication, financial aspects and accessibility and convenience all presented as mean±SD. Time spent with the screening provider averaged a score of 3.86±1.6, consistent with moderate satisfaction.
Domains of satisfaction
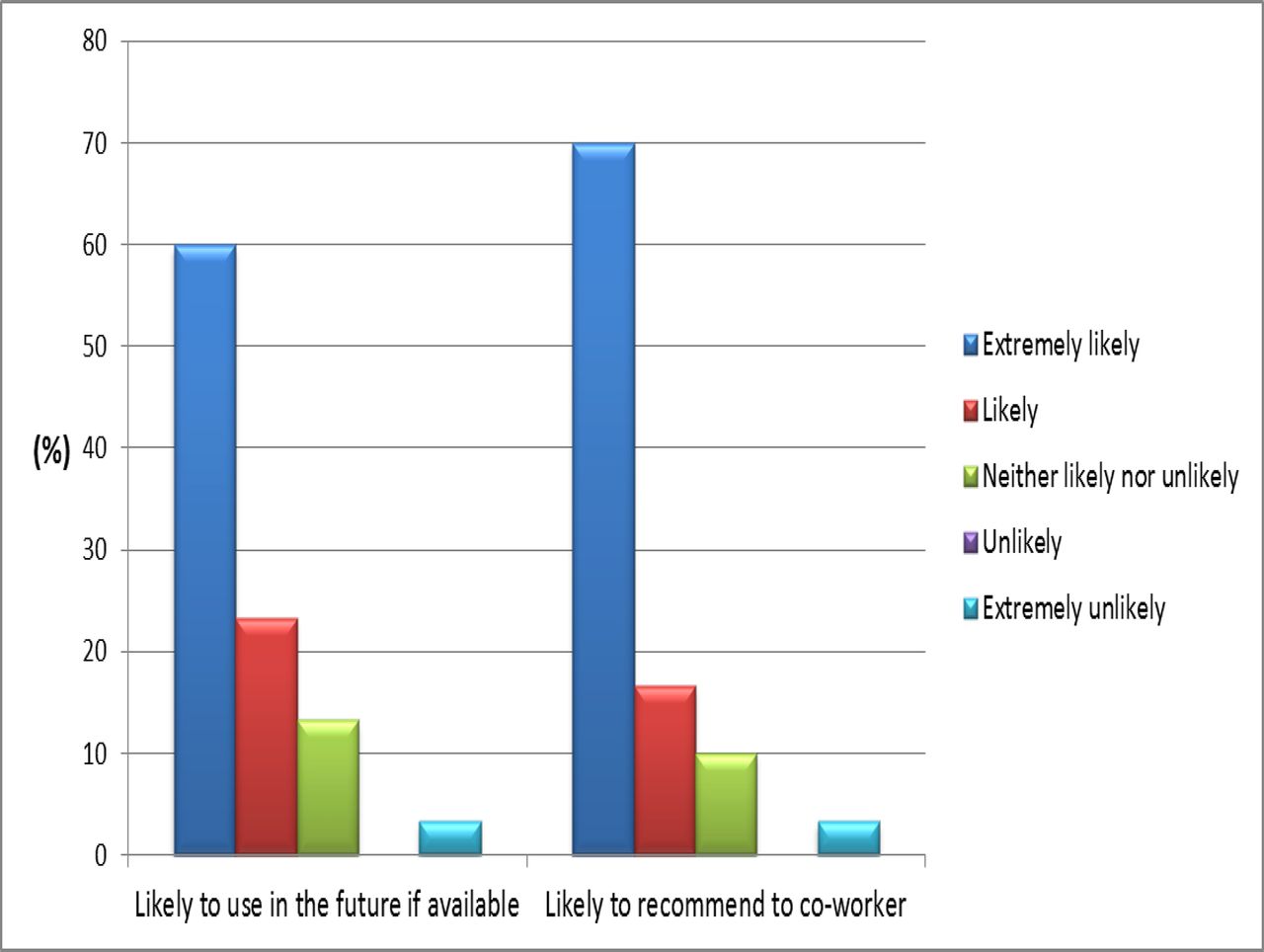
The vast majority (93.3%) of participants agreed that the screening site was convenient and 66.6% reported the screening did not interfere with their work schedule. As depicted in figures 2 and 3, 80% did not believe the intervention would put them at risk for employment discrimination. Over 80% were likely to use this model if further implemented in the future and would recommend it to a coworker.

Final survey; different areas of agreement.
{kind=link}
{kind=link}
{kind=link}
Final survey; likelihood of using or recommending this model.
Stratified analysis was done to explore the relationship between different areas of satisfaction and different baseline criteria. No statistically significant differences in areas of satisfaction or feasibility were noted when different comparisons were made including cardiovascular burden (with risk factor vs without risk factor), family size (no family vs family) or educational status (less than middle school vs middle school and higher). Online supplementary tables IIIa, IIIb and IIIc describe the stratified analysis.
Satisfaction and feasibility of farm owners with screening service
With a short survey at the end of the study, owners of the three participating sites expressed great satisfaction with the screening process. In fact, all three found it easy to accommodate time and space for workers to be screened. They agreed that the screening may improve their workers’ health and improve their farm business. Finally, they strongly stated that they would recommend this model to other farm owners; however, only two were extremely likely to adopt a permanent similar screening model. Farm owners reported that they do not provide medical insurance. One farm owner provides workers with extra cash on their paychecks designated as medical expense money. However, she did not require workers to spend that money in any particular way. The other two farm owners did not offer any type of monetary assistance towards medical expenses.
Discussion and conclusions
This pilot prospective study demonstrated that cardiovascular risk factors are highly prevalent in MAWs. Screening on a farm worksite appears to be a feasible and satisfactory model of service in this population.
Although this population sample was relatively healthy with only two self-reported cases of hypertension initially, the majority were at higher risks of cardiovascular disease for being either smokers or overweight. Nevertheless, multiple undiagnosed and new cases of pre-diabetes, diabetes, hypertension and hyperlipidaemia were uncovered over the study period. Fifteen participants were identified with one or more CV risk factors but, as noted above, very few (2) were seen for follow-up at the Migrant Health Clinic and two others reported following up with a primary care provider. Other subjects (7) reported lack of time and long distance (4) of approximately 20 miles from our Migrant Health Clinic as main reasons for not scheduling a follow-up visit. Two participants with CV risk factors left their jobs before the study ended. Other possible reasons include access to insurance, residence status, and language and cultural barriers, which indeed match findings from previous research (5); however, the Migrant Health Clinic in Rochester MN has full-time bilingual/Hispanic staff, does not require proof of residence and charges sliding scale fees based on income. Thus, we believe distance and nature of their work (as noted above, some work >50 hours/week) continue to represent the major barriers for follow-up on screening-detected diagnosis.
The literature overwhelmingly shows overall poor health, prevalent risk factors and great barriers to healthcare in farm workers. Discussions with farm owners confirmed that they do not offer workers medical insurance. Hence, new and innovative methods are needed to deliver care to this population. Screening on a farm worksite may be one of the approaches that can reduce barriers such as distance and work schedules and improve access. The intervention offered preventive measures that were free of charge and was facilitated by employers’ buy-in. Accommodation of time and space, and the availability of a bilingual healthcare provider also ensured maximum participation of mostly non-English-speaking individuals. The challenge remains with the need for better solutions for follow-up. This proposed model of care focuses only on screening, diagnosis and education on the farm site. This pilot work provides a rationale for evaluating the delivery of additional services to MAWs at their work site, such as treatment and continuity of care. Such approach has been proven effective in other settings. Alderman for example20 23 24 tested the detection and treatment of hypertension at the worksite and reported improved adherence and better control of blood pressure, as well as less disability and hospitalisation days. However, Alderman’s work took place in an urban setting and validation in farm setting may demonstrate the need to modify his approach to fit the unique needs, values and preferences of this unique population.
Limitations
The major limitations to this pilot study is the small sample size of MAWs and the attrition rate (21%), although this attrition rate was expected due to the mobility and job instability among MAWs. Another possible limitation is the lack of crops and seasonal farms recruitment (sample included three dairy farms). Selection bias could have affected the results since participating farm owners (previously engaged in research projects with University of MN) may not represent other farm owners who may be less acceptant of health screening of their workers. We did not inquire whether MAWs were legal immigrants or H2-A visa holders. If any were illegal, they may have not had the ability to seek further follow-up.
References
Footnotes
Contributors All authors have substantially contributed to this pilot study. Study design: TR, JR, MHM. Data collection: TR, JR. Data analysis and interpretation: TR, KM. Manuscript writing: TR, KM, MHM. All listed authors have reviewed, revised and approved the final manuscript and agreed on accountability for all aspects of the submitted manuscript.
Funding This project was funded by University of Minnesota Upper Midwest Agricultural Safety and Health Center through sub-award (no. P004365208).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The project was approved by the Institutional Research Board at Mayo Clinic in Rochester MN (Protocol 15- 000647) and is registered in ClinicalTrials.gov (ID NCT02418637).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All available data can be obtained by contacting the corresponding author.