Article Text

Abstract
Introduction There is only limited and conflicting evidence on the effectiveness of Pay-for-Performance (P4P) programmes, although they might have the potential to improve guideline adherence and quality of care. We therefore aim to test a P4P intervention in Swiss primary care practices focusing on quality indicators (QI) achievement in the treatment of patients with diabetes.
Methods and analysis This is a cluster-randomised, two-armed intervention study with the primary care practice as unit of randomisation. The control group will receive bimonthly feedback reports containing last data of blood pressure and glycated haemoglobin (HbA1c) measurements. The intervention group will additionally be informed about a financial incentive for each percentage point improved in QI achievement. Primary outcomes are differences in process (measurement of HbA1c) and clinical QI (blood pressure control) between the two groups. Furthermore, we investigate the effect on non-incentivised QIs and on sustainability of the financial incentives. Swiss primary care practices participating in the FIRE (Family Medicine ICPC Research using Electronic Medical Record) research network are eligible for participation. The FIRE database consists of anonymised structured medical routine data from Swiss primary care practices. According to power calculations, 70 of the general practitioners contributing to the database will be randomised in either of the groups.
Ethics and dissemination According to the Local Ethics Committee of the Canton of Zurich, the project does not fall under the scope of the law on human research and therefore no ethical consent is necessary. Results will be published in a peer-reviewed journal.
Trial registration number ISRCTN13305645; Pre-results.
- pay for performance
- financial incentive
- reimbursement
- diabetes
- general practice
- primary care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This randomised controlled trial (RCT) will allow to directly observe the impact of a financial incentive on evidence-based quality indicators (QIs) in patients with diabetes, comparing both process and clinical QIs.
The secondary outcomes of this study are not directly targeted by financial incentives, in order to assess the indirect impact of the Pay-for-Performance programme on cardiovascular risk in patients with diabetes.
We chose the study population of diabetic patients, since diabetes is highly prevalent and is associated with high morbidity, mortality and costs.
The database of the Swiss FIRE (Family Medicine ICPC Research using Electronic Medical Records) project is the first and, to date, only database of clinical routine data in Swiss primary care.
Introduction
Evidence regarding Pay-for-Performance (P4P) programmes is inconclusive. However, P4P interventions might be an interesting approach to improve adherence to guidelines and quality of care in primary care. Effectiveness of P4P programmes highly depends on different factors: study type (randomised controlled trial (RCT), before after design and interrupted time series), investigated quality indicator (QI) (process versus clinical variables), type of healthcare system (gate keeping versus non-gate keeping), study participants (large-scale community clinics versus single-handed primary care practices), patient selection (socioeconomic status, multimorbidity and insurance type) and the method and level of payment.1–3
In a gate keeping healthcare system such as the National Health System (NHS) of the UK, the Quality and Outcomes Framework (QOF) introduced financial incentives for evidence-based QI in primary care. Subsequently, achievements with regard to all QIs increased.4 Since the QOF was a nationwide pretrial/post-trial without control group, it remains controversial to which extent the P4P programme or the increasing guideline adherence over time was responsible for this improvement. Evidence from P4P programmes in a different healthcare setting such as the USA has shown to be conflicting.2 5–7 RCTs from countries outside of Europe and the USA have shown positive effects of certain P4P interventions.8–11 A systematic review12 concludes that financial incentives targeting indicators that can be directly altered by providers (eg, the number of measurements) have shown greater effects than financial incentives targeting indicators that can only be indirectly influenced (eg, blood pressure values).
In Switzerland, no data on the P4P approach exists and the role of QIs, especially in primary care, has been marginal. The main reason might be that—in contrast to the UK for example—documentation in primary care is still mainly paper based instead of based on electronic medical records (EMR).13 General practitioners (GPs) do not receive external (financial) support for EMR implementation; they bear the running electronic system costs themselves. There is evidence for technical assistance and financial incentives alongside EMR implementation being able to improve quality of care,14 15 at least modestly concerning improvements in cardiovascular care processes and outcomes.16 Also, combining a feedback mechanism alongside with EMR implementation and therefore providing users with near-term benefits from maintaining good data as well as financial incentives have shown to be promising approaches in promotion of EMR implementation in primary care.17–22
The Institute of Primary Care of the University and University Hospital of Zurich founded the research network FIRE (Family medicine ICPC Research using EMRs)23 with currently 290 GPs voluntarily documenting their consultations in an EMR using the International Classification of Primary Care (ICPC-2) coding system.24 The anonymised structured medical routine data are uploaded to a server of the Institute and available for analysis. A previous study has shown that the FIRE database offers a valuable base for the calculation of QI according to the QOF in patients with diabetes.25
With the current study, we aim to test a P4P approach in Swiss primary care using clinical routine data in a cluster RCT. Our hypothesis is that a financial incentives increases GPs achievements of QIs in patients with diabetes more effectively than evidence-based educational feedback reports. Since the impact of clinical parameters on prognosis of diseases is higher than the simple fact whether or not for example, blood pressure was measured, we will include two different approaches; one incentivising a clinical parameter (blood pressure control) and in the other incentivising a process parameter (the measurement of glycated haemoglobin (HbA1c)).
Methods and analysis
Outcome-Parameter
Over the entire study period, we aim to investigate the following effects of implementing P4P in Swiss primary care practices:
Effect of P4P on QI achievement in comparison to feedback reporting (by randomisation into an intervention and control group, where both groups receive feedback reporting, but only the intervention group receives a financial incentive).
Difference of P4P on process (measurement of HbA1c) versus clinical QIs (blood pressure control).
P4P effect on non-incentivised QIs (lipid status measurements and levels).
Sustainability of P4P (extended observation period 24 months after study start and 12 months beyond incentives, respectively).
The QIs thresholds in our project are based on the experience of the Swiss QOF25 and the latest version of the QOF of the British NHS.26 For the threshold of the clinical QI blood pressure control, we refer to the latest recommendation of the European Society of Cardiology for the management of arterial hypertension in patients with diabetes.27 Indicator achievement will be expressed as percentage of patients meeting the indicator (numerator) in reference to all eligible patients (denominator). The primary and secondary outcomes are summarised in table 1.
Outcome parameters
Study design
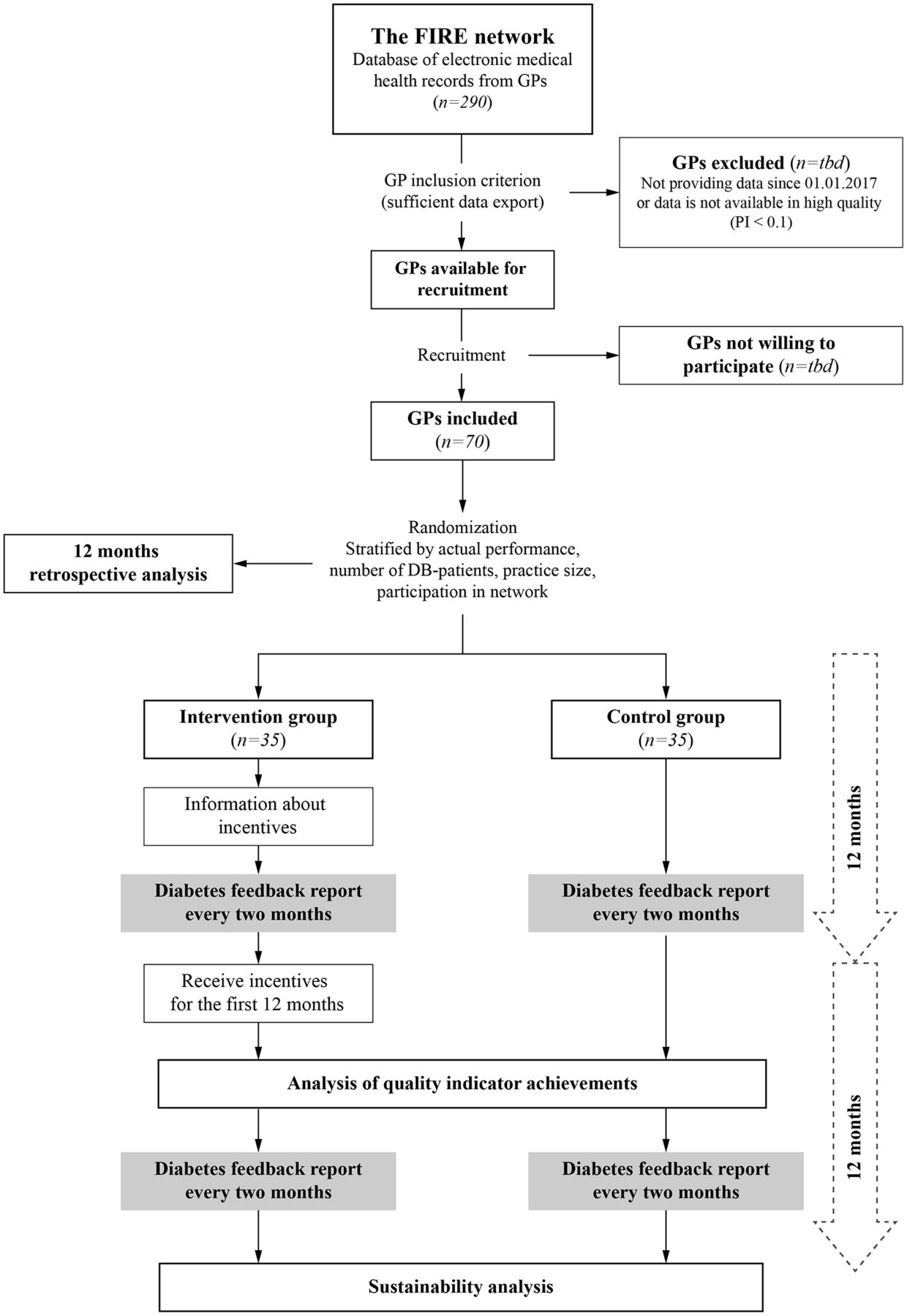
The study is a cluster-randomised, two-armed intervention study based on the FIRE database, with the practice as the unit of randomisation. The practice at the level of randomisation was chosen to avoid contamination of intervention. The study flow chart is presented in figure 1.

{kind=link}
Flow chart of the study. DB-patients, patients with diabetes; FIRE, Family Medicine ICPC Research using Electronic Medical Record; GP, general physician; PI, process indicator.
Data collection
The FIRE database of the Institute of Primary Care, University of Zurich will provide the database for this study. Up to December 2017, 290 GPs from 14 German-speaking cantons of Switzerland participated in the FIRE project. In December 2017, the database contained data of 3 372 343 encounters of 345 811 patients.
It consists of following data components:
Administrative data (year of birth, gender, dates of each consultation and unique anonymised patient identification number).
Vital signs: systolic and blood pressure, pulse, height, weight and waist circumference.
ICPC-2: between one to seven codes for reason for encounter and diagnoses per contact date as assessed by the GP.
Laboratory values: haemoglobin, leucocytes, C reactive protein, erythrocyte sedimentation rate, creatinine, total cholesterol, high-density lipoprotein cholesterol and low-density lipoprotein cholesterol, triglycerides, glutamat-oxalacetat-transaminase (aspartate aminotransferase), glutamat-pyruvat-transaminase (alanine aminotransferase), gamma-glutamyl transferase, fasting glucose, HbA1c, prostate-specific antigen and so on; all values including their reference range and date of analysis.
Medication data: Anatomical Therapeutic Chemical Classification, medication doses, in-take time (morning, noon, evening and night-time), cessation date and comments.
Structural data on participating GP practices (physicians’ age and training, practice type (single-handed, double or group practice), location and laboratory connection), which are collected at individual project entry.
Sample size
For the process QI (HbA1c) we assume an improvement from currently 70% adherence to 85% with a power of 90%. For the clinical QI (proportion of patients with controlled blood pressure defined as <140/85 mm Hg) we assume a lower increase and calculated with an improvement from currently 45% to 56%.25 We account for a cluster effect of 0.04. For the process QI (HbA1c), we will need 70 clusters and 6 observations per cluster (total of 418 patients). For the clinical QI (blood pressure) we will need 70 clusters and an average of 26 observations per cluster (total of 1804 patients). We will therefore include 70 GPs in in our study.
Recruitment of GPs and randomisation
GPs are eligible if the data set is complete for all 12 months in 2017 and a minimum threshold of 0.1 is achieved for the process indicators of HbA1c and blood pressure, to rule out technical problems.
The level of randomisation will be on the practice level. The participating practices will be divided into an intervention and control group. Current performance status (clinical QI blood pressure), number of GPs per practice, details of network participation of the practice and number of patients with diabetes will be used to stratify randomisation. In contrast to the UK,4 we do not expect relevant social differences in the Swiss study population28; we therefore will not stratify according to geographical region, urban versus suburban GPs, respectively.
Patient inclusion criteria
Primary care patients with diabetes mellitus will be identified from the FIRE database according to the following criteria:
Patients with ICPC-2 codes T89 (insulin-dependent diabetes mellitus) and T90 (insulin-independent diabetes mellitus).
Patients with antidiabetic medication (oral antidiabetics and/or insulin) according to the pharmaceutical cost group (PCG) (A10A/A10B/A10X).29
Intervention
Both the intervention and control group will receive intensified feedback reports on the characteristics of their current patients with diabetes, including last data of blood pressure and HbA1c measurements. Moreover, excerpts of current diabetes treatment guidelines will be provided within the feedback report as recommendations.
After randomisation, GPs in the intervention group will additionally be informed that they will receive a financial incentive after 12 months for increasing achievements regarding the following two QI:
Percentage of patients with diabetes with blood pressure <140/85 mm Hg (clinical QI).
Percentage of patients where HbA1c was measured within the last 12 months (process QI).
At baseline, the percentage of patients meeting criteria of each QI will be measured. After one year, the percentage of patients meeting the QI will again be measured. For each improved percentage point, GPs in the intervention group will be entitled to a singular payment of 75 Swiss francs. GPs in the control group will not receive a financial incentive and will not be informed about the provision of incentives in the intervention group. The intervention stops 12 months after baseline, bimonthly intensified feedback reports will continue for another 12 months. Twenty-four months after baseline, performance will be measured again in order to estimate long-term effects of the incentive and the evidence-based feedback reports.
Data analysis
In a first step, we will perform a retrospective analysis of patient characteristics and GP QI achievements 12 months before inclusion. This analysis will allow an estimation of increasing QI achievements over time despite any financial incentive, as described in previous studies.30–32
The primary and secondary outcomes 12 and 24 months after randomisation will be compared using random effects logistic regression analysis with the individual as the unit of analysis. The GPs and practices will be included as the random effect to control for the effects of clustering.
Ethics and dissemination
Description of risk
Participants will only be exposed to the usual care of their medical provider, which is generally expected to be best practice even in a non-study setting. Participants taking part might notice and benefit from an improved quality of care as the participating GPs are motivated to reach higher achievements regarding the QI. No risks are expected.
Patient and public involvement
Patients were not involved in the process of writing the protocol. Public was involved through the governmental funder.
Ethical principles
According to the Local Ethics Committee of the Canton of Zurich, the project does not fall under the scope of the law on human research and therefore no ethical consent is necessary (BASEC-Nr. Req-2017-00797).
Dissemination plan
A first manuscript with the results of the intervention phase will be published in a peer-reviewed journal after the first 12 months. A second manuscript will also be published in a peer-reviewed journal after the completion of the whole study, covering the sustainability of P4P.
Data sharing statement
The data are gathered within the ongoing FIRE project. Additional data that are regularly gathered are stored in the FIRE database. The FIRE database can be accessed at any time by the scientific team of the institute. For external requests, access has to be requested from the head of the institute.
Discussion
The introduction of QOF in UK’s NHS suggested improvement of all QI. However, it is unclear to which amount the financial incentives or the general increase in evidence-based medicine account for this improvement, since no control group existed in this nationwide system change. RCTs in the field of P4P are scarce and often deal with preventive services, particularly immunisation1 33 or originate from very different healthcare systems outside Europe or the USA.10 11 There is particularly scarce research on the impact of financial incentives on prescribing behaviour of GPs.34 Moreover, it must be acknowledged that most RCTs in this context originate from the United Kingdom and the United States. Also, the implementation success of P4P has been shown to highly depend on environmental factors such as geographical region, practice forms, healthcare funding sources, general oversupply or undersupply of medical resources and so on.3 35 So, study results might not be applicable to differing healthcare systems such as in Switzerland.
This RCT will allow to directly observe the impact of a financial incentives on evidence-based QIs in patients with diabetes, comparing both a process and a clinical QI. We furthermore include the analysis of a QI not directly targeted by financial incentives, in order to assess the indirect impact of a P4P programme to improve cardiovascular risk in patients with diabetes.36 Additionally, the study includes a retrospective analysis to assess the baseline performance and a long-term follow-up in order to disentangle general time trends related to QI changes and to investigate the added value of the P4P intervention as well as long-term effects of P4P programmes. Following the proof of concept that the leading EMR software in Switzerland contain enough data to collect information for a QOF25 the current study will provide the first evaluation of Swiss physicians’ susceptibility to financial incentives. To our knowledge, this would be the first study assessing a P4P approach in primary care using an RCT in Switzerland.
Currently the Swiss healthcare system is undergoing massive transformations concerning reimbursement models. In the inpatient setting, the ‘diagnoses related groups’ (DRG) system has been implemented in 2012 according to the German DRG system. In the outpatient setting a revision of the reimbursement system (TARMED) is currently under way, consisting of a slight qualitative improvement of GP’s reimbursement compared with other medical specialties while limiting certain positions quantitatively. This latest revision has been introduced against the opposition of the Swiss Medical Association. On the other hand, health insurance companies are looking for new reimbursement models and QIs to differentiate among the very heterogeneous GP networks. The question, how reimbursement systems should be adapted is therefore a pressing issue. Evidence-based answers to this question are urgently needed. In order to provide stakeholders with an adequate basis of information and for a sound political decision-making process, it is essential to have a scientific knowledge based on the quality provided in primary care practices.
In conclusion, this study will provide a knowledge base for the ongoing political discussion on whether the implementation of P4P is a useful and realistic approach to improve care for patients with chronic diseases in primary care. This study might have a major impact on healthcare reimbursement models.
References
Footnotes
Contributors CC, OS and TR: initiators for this study, performed the conceptualisation and allocated the funding. OS: performed the sample size calculations. RM, LM and CC: developed the feedback report and organised the administration of the whole study. RM and CC: wrote the final manuscript. All authors read, revised and approved the manuscript.
Funding This project is supported by grants from the national research program ‘Smarter health care’ from the Swiss national science foundation (SNSF), grant number 407440_167204.
Competing interests None declared.
Patient consent Not required.
Ethics approval Ethics Committee of the Canton of Zurich.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.