Article Text

Abstract
Introduction Vasopressin stimulates cyst growth in autosomal dominant polycystic kidney disease (ADPKD) leading to enlarged kidneys, hypertension and renal failure. Vasopressin receptor blockade slows disease progression. Physiological suppression of vasopressin secretion through high water (HW) intake could achieve a similar effect, necessitating a definitive large-scale trial of HW intake in ADPKD. The objective of the DRINK trial is to answer the key design and feasibility questions required to deliver a successful definitive water intake trial.
Methods and analysis We describe the design of a single-centre, open-label, prospective, randomised controlled trial. The "Determining feasibility of R andomisation to high vs. ad libitum water In take in Polycystic K idney Disease" (DRINK) trial aims to enrol 50 patients with ADPKD, over the age of 16 years with an estimated glomerular filtration rate (eGFR) ≥20 mL/min/1.73 m2. Participants will be randomised 1:1 to HW intake based on an individualised water intake prescription, or to ad libitum (AW) water intake. The HW group will aim for a dilute urine (urine osmolality ≤270 mOsm/kg) as a surrogate marker of vasopressin suppression, and those in the AW group will target more concentrated urine. Participants will have an 8-week treatment period, and will be seen at weeks 0, 2, 4 and 8, undergoing assessments of fluid status, renal function and serum and urine osmolalities. They will receive dietary advice, and self-monitor urine specific gravity and fluid intake. The trial employs smartphone technology to permit home monitoring and remote direct data capture. The primary feasibility end points are recruitment rate and separation between arms in measured urinary osmolality. Key secondary assessments include acceptability, adherence, health-related quality of life, acute effects of HW intake on measured (51Cr-EDTA) and eGFR and ADPKD-related pain.
Ethics and dissemination Ethical approval was awarded by the East of England Essex Research Ethics Committee (16/EE/0026). The results of DRINK will be submitted to peer-reviewed journals, and presented to patients via the PKD Charity.
Trial registration number NCT02933268 and ISCRTN16794957
- autosomal dominant polcystic kidney disease
- vasopressin
- water
- osmolality
- urine specific gravity
- feasibility
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- autosomal dominant polcystic kidney disease
- vasopressin
- water
- osmolality
- urine specific gravity
- feasibility
Strengths and limitations of this study
The use of a randomised controlled feasibility trial designed to determine adherence and adequate separation between treatment arms will provide crucial data on the practical and biological feasibility of a definitive global high water trial.
Self-monitoring and recording of results using smartphone technology will aid compliance and allow remote data capture, thereby reducing the burden of trial visits on participants and facilitate recruitment and streamlining of future trials.
The effect of high water intake in autosomal dominant polycystic kidney disease (ADPKD) was identified as a research priority by patients with ADPKD . The trial was designed and is being conducted in partnership with the PKD Charity.
DRINK will include those with more advanced kidney disease (chronic kidney disease (CKD)3 and CKD4), representative of typical patients under hospital care.
DRINK is limited by the relatively short duration of follow-up, thus not providing data on the long-term sustainability of fluid prescription adherence.
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is the the most common human inherited renal disorder affecting 12 million people worldwide.1 Kidney cyst growth throughout the life span leads to enlarged kidneys, hypertension and impaired kidney function. More than two-thirds of those affected will develop kidney failure by a median age of 58 years,2 approximately 10 years earlier than for most other primary kidney diseases.3 Interventions that slow the progression of ADPKD are urgently needed.
ADPKD is usually caused by mutations in PKD1, PKD2 or, rarely, GANAB.4 Its pathogenesis is incompletely understood. PKD1 and PKD2 encode the polycystins PC1 and PC2, respectively. PKD1 or PKD2 mutations lead to reductions in intracellular calcium, accumulation and impaired destruction of cyclic adenosine monophosphate (cAMP) and reduced intracellular ATP. This promotes sensitivity of collecting duct epithelial cells for the tonic effects of vasopressin.5 Since vasopressin promotes cyst growth, it has emerged as a therapeutic target for ADPKD.6 Recent evidence has confirmed efficacy of vasopressin receptor blockade with the V2 receptor antagonist Tolvaptan in slowing ADPKD progression, reducing the annual increase in total kidney volume (TKV) by 2.7%7 and slowing the rate of estimated glomerular filtration rate (eGFR) decline.8 However, the utility of Tolvaptan is limited by cost and side effects, with up to 25% of patients intolerant of the drug.7
Vasopressin release from the posterior pituitary is driven by plasma osmolality,9 and is readily suppressed by drinking beyond thirst. It is therefore plausible that high water (HW) intake could slow the progression of ADPKD through reduced exposure of the kidneys to vasopressin. Congruent with this hypothesis, studies in the PCK rat have shown slowing of cystic kidney disease and vasopressin suppression with HW consumption.10 11 In humans, Amro et al 12 showed significant reductions in copeptin concentration and urine osmolality after 2 weeks of solute restriction and HW intake in 34 patients with ADPKD. In a prospective observational study, HW intake in 13 patients with ADPKD resulted in reduced urine osmolality and increased urine volume compared with healthy controls after 7 days13. However, in a non-randomised prospective study of 30 patients with ADPKD, HW intake resulted in a more rapid decline in eGFR and increase in TKV despite a significant reduction in urine osmolality and plasma copeptin level compared with controls.14 Uncertainty therefore remains over the effectiveness and safety of HW intake in preserving kidney function in patients with ADPKD. Adequately powered randomised trials are urgently needed.
One other trial of HW intake is currently underway (PREVENT-ADPKD ACTRN12614001216606), with the aim of recruiting 180 patients with ADPKD who will be randomised to HW or standard water intake.15 However, PREVENT-ADPKD has several important limitations. First, patients with eGFR <30 mL/min are excluded from the trial. Second, the primary outcome is change in height-adjusted TKV (htTKV), a surrogate for kidney function decline. Powered (87%) to detect a relatively large difference in htTKV increase, there is a very real risk that clinically meaningful effect may exist but might not be detected in a trial of this size. Third, the validity of htTKV as a surrogate for disease progression is disputed.7 16 PREVENT-ADPKD will therefore not determine the effect of HW intake on kidney function. Finally, PREVENT-ADPKD will not assess the acute effects of increased hydration in eGFR. Acute effects are of high importance in selecting the most appropriate kidney function end point for interventional trials in CKD.17 It is apparent that, irrespective of the outcome of this trial, a large randomised comparison of the effect of HW intake versus standard of care on kidney function will remain necessary.
We report the design and set-up of a randomised feasibility trial of HW versus ad libitum (AW) water intake, developed to rigorously assess the feasibility of a definitive trial powered to detect a difference in kidney function decline in patients with ADPKD. This trial was initiated by patient members of the PKD Charity through a research proposal to the Patient Led Research Hub during 2016, and has been codesigned and produced (and part funded) by the PKD Charity. A full version of the trial protocol can be found at the following link http://cctu.medschl.cam.ac.uk/Trials/Drink/Materials.htm on the DRINK trial website.
Methods and analysis
Objectives
The primary feasibility objectives are: 1) recruitment rate and 2) achievement of target urine osmolality in ≥85% of study participants in the HW group. Secondary end points include separation in urine osmolality between trial arms, the completeness of self-monitored urine specific gravity (uSG) data (adherence to the self-monitoring regimen), serious adverse event rate, changes in quality of life using the EuroQol Five Dimensions (EQ5D) scores from baseline to 8 weeks, change in pain scores between groups, change in measured GFR between baseline and 4 weeks and change in eGFR between baseline and 4 weeks (box 1).
DRINK trial primary and secondary end points
Primary end points
The number of patients eligible for, and randomised to the trial
The proportion of patients in the high water intake group achieving a urine osmolality <270 mOsm/kg
Secondary end points
The proportion in each of the high and ad libitum water intake groups achieving their target urine osmolality (between-group separation)
The proportion of participants that can self-monitor and report urine SG reliably
Acceptability and usability of the SPLASH app (qualitative questionnaires and interviews)
Incidence of serious adverse events
Change between baseline and 8 weeks in quality of life scores (measured using EQ5D)
Change between baseline and 8wk pain scores (measured using Pain Questionnaire)
Change in measured glomerular filtration rate (GFR) between baseline and 4 weeks (acute GFR effects in high water intake group)
Change in estimated GFR between baseline and 4 weeks (both groups)
Acute GFR effects measured as the change in 51CR-EDTA measured GFR from week 0 to week 4
Trial design
This prospective, open-label, randomised trial was designed to assess the feasibility of a large definitive randomised controlled trial comparing the effectiveness and safety of HW intake in patients with ADPKD with a control arm of AW water intake. Participants were randomly assigned (1:1) to receive either a prescribed (high) fluid intake sufficient to achieve vasopressin suppression, or to AW water intake (figure 1). Following an 8-week treatment period where participants will undertake all the trial assessments, they will undergo a 4-week washout and have one final end of trial visit at week 12. The trial was first proposed by the PKD Charity, and was developed through and supported by the Cambridge Patient Led Research Hub, and run by the Cambridge Clinical Trials Unit.

Schematic of the DRINK trial design. Participants are randomised 1:1 to the high water (HW) or ad libitum (AW) water intake groups. Each participant in the HW group is given an individualised daily water prescription with urinary dilution targets consistent with vasopressin suppression. The AW group has more concentrated urinary targets. ADPKD, autosomal dominant polycystic kidney disease; uSG, urine specific gravity.
Two nested substudies will be conducted: 1) substudy A includes 51CR-EDTA measured GFR and is designed to assess the acute effects on GFR of HW intake in the HW group. This substudy aims to enrol a minimum of eight participants; 2) substudy B is designed to assess the impact of a novel smartphone-based fluid intake monitoring device (termed SPLASH)18 in promoting adherence to fluid prescriptions (figure 2). Substudy B aims to enrol at least 10 participants.

Smartphone technology used during the DRINK study. The SPLASH app uses near field communication technology to automate fluid intake monitoring (left). The DRINK app will be used to record urine specific gravity results allowing remote data collection and monitoring of progress (right).
Trial population, eligibility criteria and recruitment
Patients with a confirmed diagnosis of ADPKD aged 16 years or older are eligible for enrolment in the trial (box 2). Patients are deemed ineligible if they have advanced renal impairment (defined as an eGFR <20 mL/min/1.73 m2), are unable to provide informed consent, are unable or unwilling to comply with study procedures including self-monitoring of uSG, have evidence of fluid excess (defined as peripheral oedema, pulmonary oedema, heart failure, liver cirrhosis) or are receiving treatment with diuretics for such states, have concomitant renal diseases other than ADPKD, are pregnant or breast feeding or are receiving treatment with Tolvaptan within 4 weeks of screening.
Eligibility criteria
Inclusion criteria
Diagnosis of autosomal dominant polycystic kidney disease (radiological and or genetic evidence of PKD1 or PKD2 mutations)
Aged 16 years or older
Ability to provide informed consent estimated glomerular filtration rate ≥20 mL/min/1.73 m2
Able to self-monitor urine specific gravity
Exclusion criteria
Fluid overload states, eg, heart failure, cirrhosis or requirement for fluid restriction
Confounding illness impacting on renal disease, eg, concomitant diabetes or glomerulonephritis
Treatment with diuretics for fluid overload (those on diuretics for hypertension may participate in the trial after a run-in period of 2 weeks)
Treatment with Tolvaptan in the last 4 weeks
Pregnancy or breast feeding
In this single-centre trial, participants will be recruited from the renal genetics and tubular disorders clinic at Addenbrooke’s Hospital, Cambridge. Patients from other centres are eligible for entry, but have to attend Addenbrooke’s Hospital for screening, enrolment and study procedures. Patients will be reimbursed for travel and other expenses, but will not receive any other payment or incentives for trial participation.
The DRINK trial was advertised nationally on the PKD Charity and RaDAR websites and presented at PKD Patient Information days. Recruitment commenced in September 2016. The trial aims to enrol up to 50 participants. The trial steering committee may recommend halting recruitment at any point after 30 patients have been enrolled if it is clear that the feasibility questions have been adequately addressed.
Randomisation
Participants will be randomly assigned (1:1) to HW or AW water intake using a manual sealed envelope system prepared by the Cambridge Clinical Trials Unit statistician and to which the trial team will be blinded.
Although we have chosen patient level randomisation, the autosomal dominant inheritance pattern of ADPKD raises the particular challenge that multiple members of the same family or household may participate in a trial. In the context of HW intake, this may result in contamination between trial arms since fluid consumption patterns of one family member may be influenced by that of another. This is particularly relevant given that we have previously reported that up to 80% of patients with ADPKD regularly discuss their condition and treatments with their family members.19 The ability to draw inferences on contamination between trial arms within family clusters will be dependent on the number of related participants enrolled into the trial. Were contamination between arms apparent within family clusters, this may need to be taken into account in the randomisation strategy for a definitive trial.
Intervention
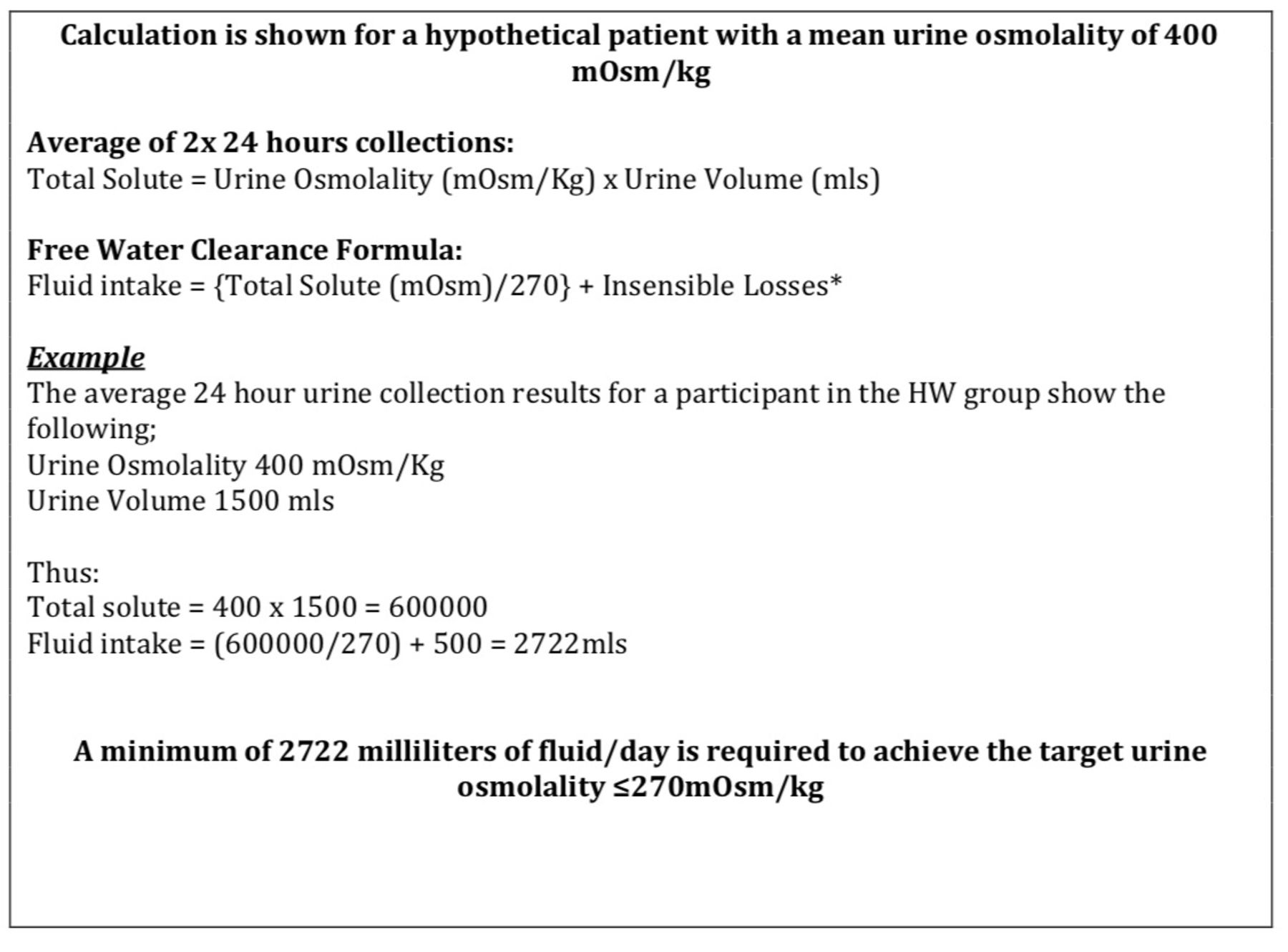
Participants allocated to the HW intake arm will receive an individualised daily fluid intake prescription based on the free water clearance formula (figure 3) and designed to achieve suppression of vasopressin.

{kind=link}
{kind=link}
{kind=link}
Calculation of fluid prescription using the free water clearance equation. Insensible losses were arbitrarily set at 500 mL as an average.
The fluid prescription will be titrated to response against uSG (table 1), since a uSG ≤1.010 correlates with vasopressin suppression and is easily assessable by urine indicator strip testing.20 Urine osmolality will also be measured during study visits, and fluid prescription titrated in order to achieve a urine osmolality of ≤270 mOsm/kg. Participants are required to self-monitor uSG twice weekly to ensure that their fluid intake is sufficient to maintain the dilution target. Remote monitoring of home uSG values will be facilitated through the use of a bespoke smartphone application (app) that allows participants to input and monitor their uSG values. Titration instructions are embedded within the app. Participants will be encouraged to preferentially consume water, but consumption of other beverages is not restricted and will contribute to calculation of the daily fluid consumption total. Participants will undergo regular dietary evaluation encouraging them to maintain moderate sodium (<2 g/day) and protein (0.75–1 g/kg/day) intake in order to facilitate adherence to the urinary dilution target.
Advice given to participants based on urine SG and treatment group
Control
Participants allocated to the AW arm will not be given any fluid intake target, but will be asked to drink according to their usual practice and guided by thirst. They will also be required to monitor uSG using as for the HW group, but with a uSG target of >1.010 (corresponding to a urine osmolality >300 mOsm/kg) given that, above this threshold, vasopressin is not suppressed. If the uSG is below this threshold, fluid intake is to be titrated to achieve the target (table 1), requiring a reduction in fluid intake. Dietary advice will be as for the HW group.
Adherence
Any attempt to conduct a trial of HW intake will need to identify mechanism for, and demonstrate the feasibility of, achieving and maintaining separation between trial arms sufficient to realistically translate into a biologically meaningful effect. Studies of the effect of HW intake advice on renal stone disease have shown the majority of patients are non-adherent to fluid prescription21 and, in patients with ADPKD,19 often overestimate daily fluid intake. Several methods have been used to increase water intake in adults including education and counselling, goal setting, self-monitoring or the provision of calibrated containers. A recent systematic review of 16 studies showed that self-monitoring (urine volume and uSG) were the most effective strategy to increase fluid intake, highlighting the importance for adherence-promoting methods.21 In order to maximise the likelihood of achieving separation between trial arms, the DRINK trial will employ several novel approaches that include home monitoring of uSG and the use of smartphone technology for both monitoring and direct feedback purposes. Given that these strategies will be combined with education and counselling and regular dietary review of solute intake, failure to achieve and maintain separation between arms using the DRINK trial design would cast serious doubt on the feasibility of a larger trial powered to detect effects on kidney function decline. Assessment of the potential for a biologically meaningful separation will be facilitated by the objective analysis of measured urine osmolality and plasma copeptin concentrations.
Determinations
Blood pressure will be assessed after 5 min rest while seated. Screening blood pressure will be assessed using the DINAMAP Carescape monitor in routine clinic use. Blood pressure measurements will be taken in triplicate, and the mean of the second and third measurement reported. Brachial blood pressure will be taken in the non-dominant arm with an appropriately sized cuff, according to British Hypertension Society guidance. Side room urinalysis will be carried out using Siemens Multistix GP indicator strips, read by Siemens CliniTek Status+ auto-analyser. uSG will be measured as a surrogate for urine osmolality by automated analysis of colorimetric change on Siemens Multistix.
Home measurement will be conducted by visual assessment of colorimetric change, read after 45 s against the manufacturer’s standard reference colour chart. Urine volume and measured urine osmolality will be obtained by performing two 24 hours urine collections at baseline. Further 24 hours urine samples will be obtained at 2, 8 and 12 weeks. Spot urine samples will be collected for urine osmolality estimation at every visit. Urine and plasma osmolality is measured on the Advanced Instruments Micro-Osmometer, Model 3320 using the freezing point depression method.
Creatinine will be measured using the Siemens Advia 2400 autoanalyser. Screening eGFR will be derived from the 4-variable MDRD GFR equation.22 All within-trial eGFR measurements will be calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.23 Serum copeptin (a surrogate for vasopressin concentrations)24 will be analysed by the Department of Clinical Chemistry at the Royal Victoria Infirmary, Newcastle, UK.
Plasma samples will be obtained on all participants at all time points for biobanking.
Measured GFR will be determined by 51CR-EDTA. On the day preceding the test, participants will be asked to abstain from high protein meals and excessive caffeine, and to abstain from caffeine consumption after 22:00 hours. They will be permitted a light breakfast on the day of the test. An intravenous injection of 2MBq 51CR-EDTA was administered via a 16G cannula. Venous blood (10 mL) will be drawn from the contralateral arm at baseline, 2, 3 and 4 hours after the injection. Samples will be centrifuged for 15 min at 2000 rpm to allow plasma separation, and read using a Wizard2 2480 gamma counter (PerkinElmer). The GFR will be derived from the area under the plasma clearance curve using the slope intercept method.
Health-related quality of life will be assessed using the EQ5D quality of life questionnaire, administered at baseline and 8 weeks.
Secondary outcome data from the efficacy trial of tolvaptan suggests that the drug reduces the frequency of acute episodic pain in ADPKD.25 Although the mechanism for pain relief is unclear, it was partly explained by the reduced incidence of urinary tract infection, stones, and cyst rupture and haemorrhage. As HW intake is associated with reduced incidences of urinary stones and infections in the general population26 and the increasing recognition of chronic pain in the condition,27 we have chosen to assess pain in DRINK. This will be assessed using a bespoke pain assessment tool to collect longitudinal data on the nature, frequency and pattern of pain, and analgesic use (see online supplementary appendix I). To date, no questionnaires have been validated for the assessment of pain in ADPKD. We will employ two brief questionnaires, which are validated and widely used for a broad range of chronic pain disorders in the general population, which are Short-form Brief Pain Inventory28 and McGill Pain Questionnaire.28 The questionnaire will be completed at baseline and week 8, but participants can also record any acute episodes of pain at any time during the study. This will be facilitated through provision of the pain assessment tool within the trial smartphone app. A separate paper will follow that describes the results and feasibility of use in the DRINK cohort.
Supplemental material
An acceptability questionnaire, adapted from that used by Torres et al,7 will be administered at the end of the trial to determine the sustainability and acceptability of long-term adherence to the trial fluid intake prescription. All questionnaire-based assessments (EQ5D, pain, acceptability) can be completed on paper, via email or via smartphone app. The trial smartphone app has been developed in collaboration with FatFractile . The app will be used to record home uSG results, capture questionnaire data as described above, allow messaging and reminder functionality and to direct participants to help and additional information if required (see online supplementary appendix II). In order to avoid contamination between trial arms, two distinct versions of the app were developed, each specific to one of the trial arms. Identification of the version of the app used by participants could be monitored centrally to avoid use of the incorrect version.
Supplemental material
Run-in period
Eligible patients who are prescribed either diuretics or Tolvaptan will be allowed to enter a 2-week run-in period after enrolment during which these drugs will be withdrawn. At the end of the run-in period, these participants will be reassessed to ensure that they still met the eligibility criteria before commencing the trial. Diuretics will only be withdrawn if the indication is hypertension, and which case alternative antihypertensives will be prescribed. Alternatives that would result in acute effects on GFR will be avoided (ACE inhibitors and angiotensin receptor blockers).
Participant timeline
The trial design is represented graphically in figure 1 and the schedule of events in table 2.
Schedule of enrolment, intervention and assessments
Screening
Patients who are potentially eligible will be invited for a screening visit. Screening will include a medical history and a targeted ADPKD-related history that captures data on the timing and nature of the diagnosis, kidney size and function, and the presence of any complications such as pain, haemorrhage, nephrolithiasis or infections. Comorbidities and medications will be recorded. A full physical examination will be conducted that includes assessment of blood pressure. Indicator strip side room urinalysis will be performed. Blood analysis will include a full blood count, liver function tests, electrolytes and creatinine and paired serum and spot urine osmolalities. Participants that are deemed eligible will be provided with two 24 hours urine collection bottles for return at the time of the baseline visit in order to measure osmolality and urine volume.
Baseline
Eligible participants who have provided informed consent will be randomised at the time of the baseline visit. A targeted physical examination to assess fluid status and vital signs will be conducted. Participants will be weighed, prescribed medications noted and blood and urine taken to measure electrolytes and creatinine, osmolality and urinalysis. A baseline quality of life EQ5D questionnaire will be completed. Participants will be instructed on how to conduct indicator strip uSG analysis, and asked to perform urinalysis twice weekly on Mondays and Thursdays between 16:00 and 20:00 hours. They will be assisted in installing the DRINK trial smartphone app on their smartphone, and will be provided with a tutorial on its use. This will allow input of home uSG measurements. Participants who do not own a smartphone will be required to telephone, email or text uSG results to the trial team. Finally, participants will be required to complete the DRINK trial pain assessment tool (see online supplementary appendix I).
Follow-up (weeks 2, 4, 8)
Participants will be recalled for follow-up visits after 2, 4 and 8 weeks. During these visits, a physical examination will be carried out and weight and vital signs recorded. Blood and urine samples will be taken to measure electrolytes and creatinine, osmolality and urinalysis. Urine for 24 hours urine osmolality will be collected at weeks 2 and 8, respectively. A dietary assessment will be carried out at weeks 4 and 8. A pain assessment and EQ5D questionnaire will be completed at the 8-week visit.
Washout period and final visit
After completion of the intervention period (week 8), participants will be asked to revert to their pre-enrolment fluid intake. After a further 4 weeks, a final visit will be conducted (week 12). This will include all assessments conducted at the 8-week visit, with the exception of pain and quality of life questionnaires.
Substudy A
Effect of high water intake on 51CR-EDTA GFR
Determining the acute effects of HW intake on GFR is a prerequisite to the definition of renal end points in any future trial.22 We will conduct a substudy to determine the acute effect of HW intake on 51CR-EDTA GFR, to allow a more rigorous assessment of GFR than that derived from estimation equations. Eight patients will be enrolled in this substudy, which will require a negative pregnancy test in addition to the eligibility criteria for the main trial.
Participants in substudy A will undergo 51CR-EDTA GFR measurement at baseline, week 2 and week 4 in addition to all other trial measurements.
Substudy B
SPLASH smartphone fluid intake monitoring
Substudy B was designed to evaluate the feasibility and usability of a novel smartphone-based fluid intake monitoring device termed SPLASH.18 This Android-based app uses reusable near field communication (NFC) adhesive tags that attach to drink holders (glasses, cups or bottles). Tags are calibrated before use by measuring the drinks container volume (using a standard measuring jug) and programming the app accordingly. The app is activated by holding the phone near the NFC tag, allowing the user to select the volume consumed by identifying the corresponding fraction of the container (eg, full, one-half, one-quarter, etc). Ad hoc consumption of fluids from uncalibrated drinks holders is captured using customised credit card or keyring NFC tags precalibrated for most drinking scenarios. The app also allows input of daily fluid intake targets and displays progress towards this. Given that the system is android-specific, android phones will be provided to substudy B participants on loan where required.
At least 10 participants will be enrolled in substudy B. Participants in both trial arms will be eligible for substudy B enrolment. Training in the use of the SPLASH system will be provided in person, through provision of written information, and via an online training video (https://vimeo.com/208818645). Participants will be allowed to use the SPLASH system freely, but will be specifically required to use this for at least 24 hours at the time of the baseline, week 2 and week 8 visits (to coincide with measured 24 hours urine osmolality).
At the end of substudy B, participants will be interviewed to provide qualitative data on their experience of using the SPLASH app.
Patient and public involvement
HW intake is an issue of great importance and was identified as a key research priority by patients with ADPKD. The DRINK trial was first proposed by the PKD Charity in 2015 and, facilitated by the Patient Led Research Hub. Patient coinvestigators have remained involved throughout the design and set-up, and are coapplicants on the awarded funding grants for the trial. The study design was presented at several PKD Charity information days, and patients have provided valuable feedback on the intervention and the use of smartphone apps.
The findings of the DRINK trial will be available to patients on the DRINK trial-specific and PKD websites. They will also be presented at the PKD information days that are run throughout the year by the charity.
Adverse events and safety
Adverse events will be assessed at each study visit. Additionally, a 24-hour trial participant helpline will be made available. Given the nature of the intervention, fluid retention, worsening hypertension and hyponatraemia are adverse events of special interest.
Participants will be withdrawn from the trial in the case of persistent hyponatraemia (<132 mmol/L on two consecutive samples), fluid retention defined by the presence of one of 1) pulmonary oedema, 2) significant lower limb swelling or 3) uncontrolled hypertension on two consecutive visits despite optimal antihypertensive treatment (as judged by the responsible clinician). Participants will also be withdrawn for a decline in eGFR by ≥10 mL/min/1.73 m2 or 25% from baseline, confirmed on two consecutive samples at separate time points.
All adverse events will be recorded from the point of informed consent on the appropriate case report forms. All serious adverse events will be assessed by the chief investigator in terms of seriousness and causality and reported to the sponsor in accordance with Good Clinical Practice (GCP) guidance.
Sample size
Data from a small pilot study by Armo et al showed that using a low osmolar diet and HW intake, urine osmolality could be reduced from 426±193 to 258±147 (p=0.01) with a non-significant change in the control group.12 This is comparable to the reduction seen in the TEMPO3:4 trial (472–264 mOsm/kg), where 81% receiving Tolvaptan achieved a urine osmolality <300 mOsm/kg compared with 17% in the placebo group.29 In order to observe a benefit of HW intake on the rate of kidney function decline, we estimate that a comparable proportion of the HW intake group should achieve a urine osmolality consistent with vasopressin suppression. We estimate that 28 participants would be required to detect 85% of the HW intervention group reaching their target urine osmolality and 15% of controls achieving a urine osmolality less than the target threshold (99% power, two-sided α=0.05). Assuming a 15% dropout rate, the minimum required sample size is 30.
Statistical analysis
Analysis of the primary and secondary outcomes of the trial will use the intention-to-treat principle. All randomised participants will be included in the final analysis within their treatment group allocation regardless of compliance, withdrawal or protocol deviations. Data will be analysed as proportions/percentages, mean±SD and with linear mixed-level modelling for repeated measures (uSG, renal function and blood pressure). For non-parametric data median with IQR (2th–75th) with minimum and maximum values will be reported as appropriate. We will be using a 95% CI and a significance level of ≤0.05. The analysis will be carried out using the STATA V.15, College Station TX.
We will perform a qualitative assessment of SPLASH looking at ease and acceptability of use through participant questionnaires and face-to-face interviews. We will also collect exploratory data on the validity of SPLASH as a potential fluid intake-monitoring device, comparing the app-based intake volumes recorded to the coinciding urine osmolality results of 24 hours collections.
Data management and monitoring
Data collection will be performed by trained local research staff at each of the trial visits in the form of case report forms. This will then be entered into the DRINK trial database, which is housed in the National Institute for Health Research-accredited Cambridge Clinical Trials Unit and supervised by the trial data manager. Data from the DRINK and SPLASH smartphone apps will be transferred securely to the N3 NHS Database, where it can be accessed securely via a specialised administration panel by members of the research team using an encrypted password.
The DRINK study will undergo monitoring for regulatory compliance in accordance with the GCP guidance via the trial steering committee, which independently monitors progress and conduct of the trial and will also provide advice on the continuation, termination or amendments to the trial protocol. DRINK is sponsored by Cambridge University Hospital NHS Foundation Trust and will be subject to regular monitoring visits and audits.
Discussion
The DRINK trial will address the key feasibility issues facing future definitive HW intake trials in ADPKD. Importantly, it will determine the recruitment potential especially given the uptake of Tolvaptan, the optimal renal end point and effect size, the randomisation strategy and demonstrate whether biological feasibility which is essential to any subsequent efficacy findings is achievable. Water as a disease-modifying intervention could revolutionise the management of ADPKD, by providing a low cost, widely available treatment option for those in low-income and middle-income countries, and those with early disease for whom it is essential to target cyst development early. Yet the early stage of their condition and lack of renal function decline makes it difficult to justify the use of medications with potentially toxic side effects as the risk-benefit ratio in this group remains largely unknown.
Ethics and dissemination
DRINK opened to recruitment in September 2016, and the last study visit is anticipated to be April 2018. The primary and secondary outcomes results will be published in peer-reviewed journals, this will include a separate report on the use of smartphone technology in clinical trial design and the longitudinal ADPKD pain characteristics. A synopsis of the trial findings will also be made available to participants and the public through the trial-specific website and the PKD Charity. All the DRINK data will be shared through the Cambridge Data Repository.
Acknowledgments
The authors would like to thank the PKD Charity and the Patient Led Research Hub for their input in the design and delivery of the DRINK trial and the British Renal Society for their grant towards the funding of DRINK. RED is supported by the PKD Charity, Kidney Research UK and the Addenbrooke’s Charitable Trust. TFH and FEKF are supported by the NIHR and the Cambridge Biomedical Research Centre. The DRINK smartphone application was developed in conjunction with FatFractile and funded by the PKD Charity. The SPLASH application was developed by SPHERE IRC and was funded by the UK Engineering and Physical Sciences Research Council (EPSRC) and the Addenbrookes Charitable Trust.
References
Footnotes
Contributors All the authors contributed to the design and development of the study protocol, and have reviewed the manuscript. TFH and TH conceived the study. TFH, RE-D, IBW, FEKF and RNS designed the study, and contributed to recruitment, trial oversight and implementation of the intervention. ML provided specific support with regard to the assessment of pain in trial participants. SB and HP provided statistical expertise and supported the development of the statistical analysis plan. LBM supported the development of the patient-led proposal through the Patient Led Research Hub. AB, PW and YB-S developed the SPLASH app and contributed to development of the protocol for the SPLASH substudy.
Funding The study is funded by the British Renal Society and Kidney Care UK (formerly British Kidney Patient Association) grant programme (15-004), the PKD Charity, the Addenbrooke’s Charitable Trust (45/16) and Kidney Research UK (TF-009-20161125), and is supported by the UKCRC-registered Cambridge Clinical Trials Unit and the Cambridge NIHR Clinical Research Facility.
Competing interests None declared.
Patient consent Not required.
Ethics approval East of England Essex Research Ethics Committee (16/EE/0026).
Provenance and peer review Not commissioned; externally peer reviewed.