Article Text

Abstract
Objectives To quantify exposure to vapour, gas, dust and fumes (VGDF) and smoking in male rheumatoid arthritis (RA) and investigate impact on rheumatoid factor (RF) and anti-citrullinated protein antibody (ACPA) levels.
Design A retrospective observational study.
Setting The Royal Cornwall Hospital Trust, UK. A single university hospital setting.
Participants 726 men followed up between February 2015 and August 2016, fulfilling RA diagnostic criteria.
Main outcome measures Prevalence of VGDF exposure and smoking prior to RA diagnosis. Determination of association between VGDF, smoking and autoantibody levels.
Results 546/726 (75%) had been exposed to VGDF for >1 year. 561/726 (77%) had been smokers. Only 58/726 (8%) had no exposure to VGDF and had never smoked. A significant difference in RF levels was observed between unexposed and VGDF exposed never smokers (median RF 24 vs 36, p=0.03), more marked when comparing unexposed with ≥2 VGDF exposures (median RF 24 vs 57, p=0.02). A significant difference in RF levels was also observed between unexposed and VGDF exposed smokers (median RF 71 vs RF 95, p=0.04), more marked when comparing unexposed with ≥2 VGDF exposures (median RF 71 vs RF 113, p=0.01). A significant difference in RF titre was observed between never smokers >2 VGDF exposures and smokers with >2 VGDF exposures (RF 57 vs RF 113, p=0.02). No association of ACPA seropositivity rates or titres with VGDF exposure was observed. Smokers with >2 VGDF exposures had a significantly lower age of RA diagnosis than smokers with no VGDF exposure (53 years vs 57 years, p=0.03). All results remained similar when corrected for social class.
Conclusions VGDF exposure increases RF levels. Combination exposure to smoking and VDGF results in higher RF levels, particularly with multiple exposures. These compelling findings demonstrate the importance of combined inhaled exposures in RF generation.
- rheumatology
- immunology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Methodology allowed follow up of an entire male rheumatoid arthritis cohort, with fixed diagnostic criteria applied and non-response minimised.
Rheumatoid factor titres were reported rather than seropositive or seronegative status.
Adjustment for social deprivation and educational level was made.
Heterogeneity was noted between the cohorts studied with regard to education and social deprivation.
As a single-centre retrospective study, it is subject to a range of possible biases, with further study necessary to confirm the results in a population of wider demographic diversity.
Introduction
Rheumatoid arthritis (RA) is an inflammatory disease which primarily targets the small joints of the hands.1 Individuals with RA develop debilitating fatigue, joint inflammation, resulting in weakened grip and the subsequent development of joint deformities impairing physical function and dexterity.2
The estimated global prevalence is 0.3–1.0%.3 A UK study of patients with RA with disease duration of 10–15 years reported an annual cost of approximately £3000 per patient (2013 prices) for direct healthcare alone.4 The overall direct health cost is estimated to be £700 million in 2010 in the UK, with a further £8 billion lost to the UK economy when work productivity loss and state benefit requirements are considered.5
Identifying the underlying causes for progressive RA has centred on a combination of environmental and genetic risk factors that stimulate inflammation via autoantibody production. The RA-associated autoantibodies rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPAs) are both associated with progressive joint damage in RA6 and with mortality.7 Smoking is a risk factor for the presence of the combination of RF and ACPA in RA and the number of pack years smoked is proportional to the RF titre, but not ACPA titre in RA.8 Given the multifactorial basis for disease development, it is surprising that the effect of combined environmental exposures on autoantibody development has not been more widely investigated.
Case–control studies have observed an association independent of smoking between occupational dust and fume inhalation and the risk of male RA. This is relevant to RA as in the UK approximately 28% of patients with RA are men (reviewed in9).
Recent studies investigating the relationship between occupational exposures and chronic obstructive pulmonary disease (COPD) have used self-report of any occupational inhalational exposures together and considered these exposures as an entity that can trigger COPD. Reported exposure to vapours, gas, dust and fumes (VGDF) is independently, but modestly associated with COPD development.10 VGDF exposure greatly increases the risk of chronic obstructive pulmonary disease (COPD) particularly in smokers, with an OR 14.1 (9.33–21.2) compared with never smokers with no such work exposures.10 The combined risk of VGDF and smoking was far higher than the OR of 6.71 (4.58–9.82) in those smokers without such exposures.
The lung is considered an initiating site for RA development11 and the occupational inhalational insults associated with male RA development and COPD are concordant.9 Considering grouped inhalational exposures as the potential risk for RA development (rather than ‘last occupation’ only) has not been previously undertaken.
We aimed to study the occupational and smoking histories of all male patients with RA attending the rheumatology department in Cornwall, UK, to test a hypothesis that combinations of inhalational insults would interact to increase autoantibody levels in RA.
Materials and methods
Subjects
The data in this study were collected as part of project IRAS ID 194833, approved by South West regional ethical committee (UK). The cohort consisted of men attending routine rheumatology clinics at the Royal Cornwall Hospital, Cornwall, UK, from February 2015 to August 2016. Data were anonymised at source. Patients reviewed in clinic with a new or existing diagnosis of RA during the study period were included for analysis, initially invited to complete a written questionnaire. Data were recorded by clinicians in a standard questionnaire via face-to-face interview to determine current occupation, former occupation if retired and previously held employments for >1 year. Answers to open questions on occupation and main duties for each response were recorded, to be coded using SOC 2010, the current standard occupational classification for the UK.12 As in previous COPD literature,10 an item used in the European Community Respiratory Health Survey (ECRHS II) main questionnaire was used, with each case asked about self-reported exposures to VGDF in the line of their work.13 Missing data were obtained by follow-up telephone administration of the same questionnaire. Written consent was obtained for patients enrolled as part of the IRAS ID 194833 project investigating the role of cadmium inhalation and the development of RA. Individuals were stratified for the number of self-reported VGDF exposures in each occupation held for >1 year (0, 1, ≥2). Age, age of RA onset, disease duration, smoking history prior to disease development, RF levels at disease onset and subsequent ACPA levels were recorded as part of routine clinical practice. All patients fulfilled 2010 American College of Rheumatology/ European League Against Rheumatism (ACR/EULAR) RA criteria at diagnosis.14
Seven hundred and twenty-six patients were included for initial analysis. Of these, 22/726 (3%) had incomplete smoking data and were excluded from linear regression analysis. 3/726 (0.4%) had no verifiable RF data and were excluded from RF analysis. 54/726 (7%) had no ACPA data and were excluded from ACPA analysis. 16/726 (2%) were excluded from occupational analysis; 5/16 died during the study period and therefore had incomplete occupational data, 3/16 did not want to disclose occupation in writing or on subsequent interview. 8/16 did not return initial questionnaires and were lost to follow-up (figure 1). Prevalence analysis of VGDF and smoking was analysed as a proportion of the entire identified cohort (n=726) to bias towards the null hypothesis.

Flow diagram of patients included for analysis with reasons for exclusion.
Patient involvement
The initial concept of this research was developed from detailed histories of individual patient experiences of RA in Cornwall, UK. Initial hypotheses were presented at a local meeting of the National Rheumatoid Arthritis Society, attended by over 100 members, the majority of whom were patients with RA. Subsequent interest following the meeting led to further discussion as to the development of a protocol that would be acceptable to patients in terms of its design and acceptability. From initial ideas, this was refined and presented to the committee of the Cornwall Arthritis Trust, a local charity supporting patients with arthritis. Specific feedback was offered on wording of consent forms, questionnaire design and arrangements for follow up on patients who may not have been able to complete written questionnaires. Patient involvement in this process was invaluable for how best to manage and undertake the research in a way that was minimally intrusive for patients in their regular clinical care.
Dissemination of results to patients will take place via departmental displays post publication.
Autoantibody measurement
RF was measured with Tina-quant Rheumatoid Factors I1 Test System (Roche Diagnostics Corporation), with a value of <14 IU/mL considered as negative as per manufacturer guidelines. ACPA was measured by Second Generation E170 Anti-CCP analysis (Roche Modular Analytics), with a negative value of <17 U/mL as per manufacturer guidelines.
Social deprivation analysis
Social deprivation analysis was undertaken through the UK government validated Index of Multiple Deprivation (IMD),15 a deprivation rank score of 32 844 neighbourhoods weighted by income, health/disability, education, housing/service access, crime and living environment, converted to equal deciles.
Statistical analysis
The values are expressed as a median (IQR) or number (%). The Mann-Whitney U test was used for non-parametric comparisons of continuous data of differing sample group sizes. All data were analysed using commercially available software (Microsoft Excel (Microsoft Corp) and Number Cruncher Statistical System for Windows (NCSS60)).
Results
546/726 (75%) had been exposed to VGDF for >1 year, with 254/726 (35%) having two or more identified VGDF exposures. 561/726 (77%) had been smokers, with 349/726 (48%) having accumulated 20 pack years or more at the time of diagnosis. 58/726 (8%) had never smoked and had no exposure to VGDF (table 1). No significant difference was seen in deprivation analysis (IMD) between VGDF and smoking exposed or unexposed cohorts, even when comparing never smokers with no VGDF exposure with smokers with ≥2 VGDF exposures (median IMD decile 4, IQR ranges 3–5 to 4–6, p=0.29).
Patient characteristics for whole cohort n=726
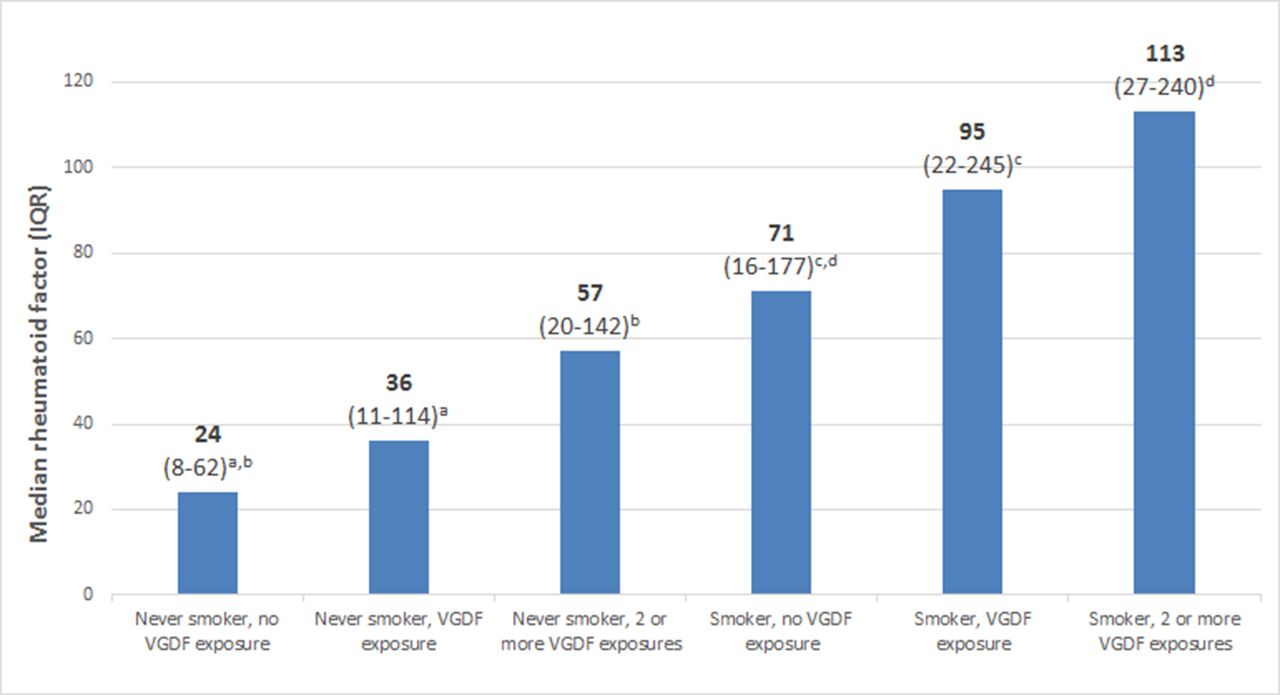
545/710 (77%) had occupations with VGDF. In never smokers and ever smokers, there was a significant dose response in terms of number of VGDF exposures and RF levels (never smoker/no VGDF, RF 24 vs never smoker/VGDF, RF 36, p=0.03; never smoker/no VGDF, RF 24 vs never smoker/≥2 VGDF, RF 57, p=0.02; smoker/no VGDF, RF 71 vs smoker/VGDF, RF 95, p=0.04 and smoker/no VGDF, RF 71 vs smoker/≥2 VGDF, RF 113, p=0.01, figure 2).
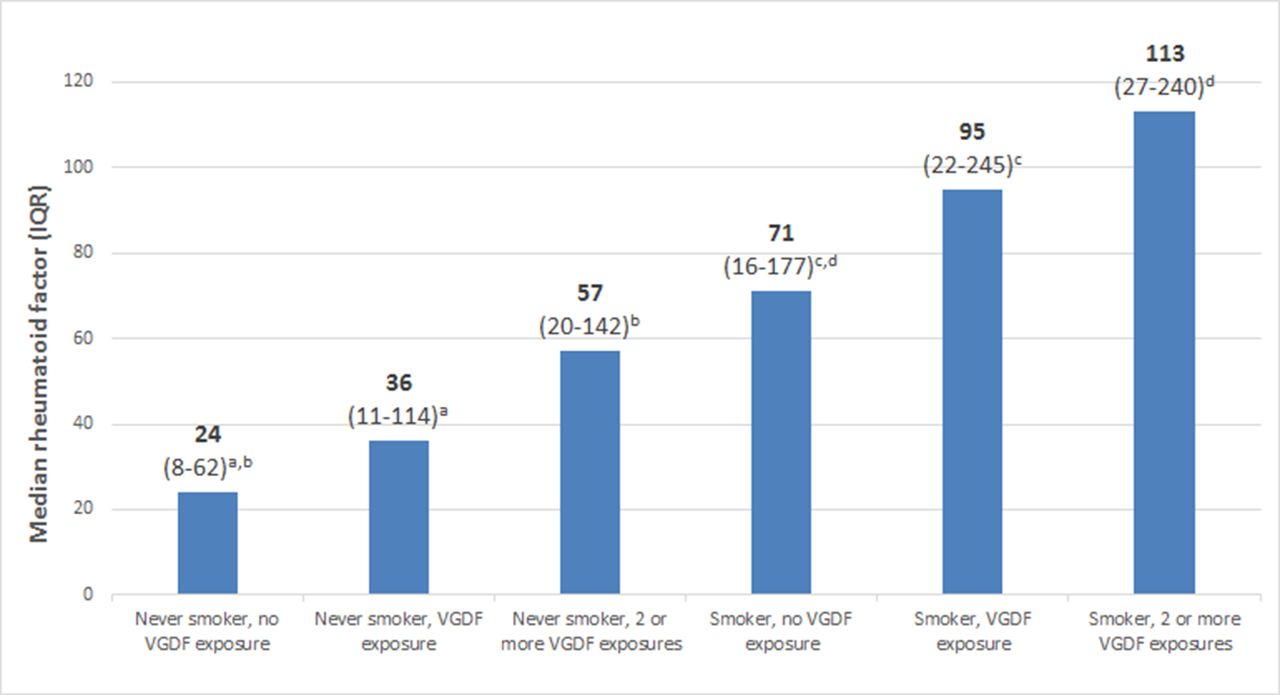
Median rheumatoid factor (IQR) by exposure group. aP=0.03 bP=0.02 cP=0.04 dP=0.01. VGDF, vapour, gas, dust and fumes.
No titre trends or significant additive relationship was seen in ACPA titres with VGDF exposure (figure 3), but smoking cohorts all had significantly higher ACPA titres than non-smoking counterparts with similar VGDF exposure (table 2). No significant association was found in ACPA seropositivity rates among VGDF exposed or unexposed groups. ACPA seropositivity rates for never smokers with 0, 1 and >2 VGDF exposures were 50.9% v 52.0% v 58.7%, p (trend)=0.44. In ever smokers, ACPA rates for 0, 1 and > 2 VGDF exposures were 70.8% v 68.4% v 66.4%, p (trend)=0.72.

{kind=link}
{kind=link}
{kind=link}
Median ACPA (IQR) by exposure group. aP=0.34 (not sig) bP=0.33 (not sig) cP=0.41 (not sig) dP=0.22 (not sig). ACPA, anti-citrullinated protein antibody; VGDF, vapour, gas, dust and fumes.
Index of Multiple Deprivation (IMD), age, rheumatoid factor (RF) and anti-citrullinated protein antibody (ACPA) by smoking and vapour, gas, dust and fumes (VGDF) exposure
Only 58/726 (8%) had never smoked and had no exposure to VGDFs and had the lowest median RF titres (24, IQR 8–62). In never smokers with ≥2 VGDF exposures, the median RF titre levels at RA diagnosis reflected ever smokers without VGDF exposure (57 vs 71). Smokers with a history of ≥2 VGDF exposures had the highest median RF titres (113, IQR 27–240) and had a significantly lower age of RA diagnosis than smokers with no VGDF exposure (53 years, IQR 44–61 vs 57 years, IQR 42–68, p=0.03, table 2).
Further analysis by multivariate linear regression on the effect of pack years smoked and cumulative VGDF exposures on RF levels demonstrated significance (R2 <0.03, p<0.0001).
In analysis of occupations listed, 33/726 (4%) had an occupation that required an educational level greater than standard UK secondary education with a school leaving age of 15 or 16 years. 10/33 (30%) were teachers or lecturers, 1/10 (10%) of which was a never smoker with no reported dust or fume exposure. 7/33 (21%) were engineering or surveying professionals with a range of reported VGDF exposures. 7/726 (<1%) were professionally occupied never smokers with no dust or fume exposures.
By broad exposure types, construction dust (a mixed group of combinations of wood, cement/concrete, fine sand/rock and gypsum, incorporating both silica, non-silica inorganic and organic dusts) was the most common type of VGDF exposure, with 330/726 (45%) reporting such exposure. More prevalent exposures included diesel fumes (239/726, 33%) and oils, including mineral oil exposure (207/726, 28%). Other exposures that were less prevalent but still existed in >10% of the total cohort included those reporting fume exposure as part of plastics manufacturing (98/726, 13%), metal fumes from electrical work (103/726, 14%) and specific dust exposure involved with rock mining (98/726, 13%), metals extraction (196/726, 27%) and wood-related trades such as carpentry and boatbuilding (155/726, 21%,).
Discussion
Principal findings
We believe this is the first study to link occupations in combination with smoking to RA autoantibody development. Strikingly high numbers of cases in this study had been exposed to VGDF (75%) or had been smokers (77%). VGDF exposure combined with smoking leads to RA development at a significantly younger age. While these findings are unique in an RA population, they reflect a trend of exposure risk as seen in COPD.10
We have found compelling evidence that a combination of environmental exposures influences RF levels, more than observed in individual exposure. RF levels were highest in those with smoking and multiple VGDF exposures.
Strengths and weaknesses of this study
There is a relative lack of comparable RA cases that are unexposed to VGDF and smoking, giving limited ability to provide statistical significance via an adequate control group to analyse specific occupational exposures in which self-report of VGDF exposure was found. The relative homogeneity of educational levels and social deprivation indices between groups in our study may explain why no significant differences were found here, though this may reflect how inhalational exposures manifest in a male RA cohort. A wider unexposed RA population and a similarly matched, non- RA cohort would both be useful for further study.
Face-to-face interview with telephone follow-up was designed to minimise non-response. At termination, only 8/726 (1%) were non-responders. Non-response, particularly in postal studies, is strongly correlated with low levels of formal education. Established literature links RA to low levels of formal education,16–18 with two UK studies observing a functional illiteracy rate of 15%.19 20 Perhaps unsurprisingly, divergence in occupations related to literacy scores has been noted, with lower scores recorded in agriculture, construction, manufacturing and mining.21 These occupations associate with male RA.9 Ninety-five per cent of occupations held by individuals in this study required no formal academic qualifications beyond secondary education; therefore, it was not possible to compare lower and higher levels of formal education for RA autoantibody prevalence. We suggest that further studies investigating the impact of socioeconomic status or formal education levels on male RA susceptibility, severity, comorbidity and mortality consider an individual’s occupation as a confounding factor.
Previous database referent studies have chosen to include patients under the age of 70.22 Occupational disease can have a long latency period; asbestos exposure and mesothelioma development are associated with a latency of between 14 and 72 years (median 51 years), with the majority of cases presenting in the seventh and eighth decade of life.23 Though we found a significantly earlier age of onset in our most severely co-exposed cohort, 104/726 (14%) cases studied were diagnosed over the age of 70. The risk of smoking and RA is evident up to 15 years after smoking cessation.24 As polarisation of RA risk estimates occurs when a latency period is used in occupational exposures,25 using an age cut-off of 70 does not allow an adequate latency period between exposure and disease development.
Much of the literature investigating occupational risk and RA has been undertaken in Sweden, in the form of case control/case referent or linkage studies from large data set analysis (reviewed in9). Studies investigating occupation and RA risk may only consider the last occupation undertaken by the respondent22 or occupation noted on the database studied. It is not uncommon for individuals with low literacy levels to move from one casual job to another, accruing different occupational exposures over time. The last recorded job may not reflect these exposures. In poorer populations, trade subspecialisation and health and safety legislation adherence may be less evident. Throughout an occupational career, unskilled workers may have multiple exposures. Construction labourers, for example, may be co-exposed to silica dust, inorganic non-silica dusts, wood dust and diesel fumes.
We suggest that studies investigating individual occupational risk and RA via single job title analysis may be confounded by multiple inhalational insults, even when correcting for smoking and quantifying single job exposure risk through the use of job exposure matrices. In a well-conducted analysis of silica versus non-silica dust exposed construction workers, Blanc et al 26 demonstrated that in ever smokers, both silica and other inorganic dust exposure were associated with increased risk of RA (Relative risks (RR) 1.36, 95% CI 1.11 to 1.68 and 1.42, 95% CI 1.17 to 1.73, respectively), while in never smokers, neither exposure was associated significantly with an increased risk of RA. This large, longitudinal cohort registry study contained detailed information on occupations and exposure types. 40 645/240 983 cases were excluded due to co-exposure to wood dust, gas or fumes to reduce confounding. It would be interesting to study these types of multiple exposures to investigate enhanced RA risk.
Possible explanations and implications for clinicians and policymakers, unanswered questions and directions for future research
We suggest potential reasons why VGDF may associate with RF and not ACPA. Newkirk et al 27 described RF generation via upregulation of IgG-heat shock protein 70 complexes stimulating production of IgA and IgM RF. Both cigarette smoke27 and harsh working environments, including exposure to dust,28 induce IgG-heat shock protein 70 complexes, with potential synergistic action on the same pathway to induce an enhanced RF response. An ACPA response is clearly related to smoking, but the mechanism by which this occurs is unclear. We acknowledge that VGDF exposure appears to have less of an influence on this process.
Furthermore, there appears to be a discordant RA autoantibody response in COPD. This is important as COPD is related to VGDF exposure and smoking in combination10 and may be pertinent to the population studied here. Newkirk et al 27 observed that 20/20 COPD cases were IgA RF positive (20/20), but 0/14 tested ACPA positive. Yang et al 29 found 29/70 COPD cases positive for RF, but 0/70 were ACPA positive. We suggest that COPD individuals either have an increased propensity for RF generation but not ACPA or that the COPD lung differentially sequesters ACPA rather than RF.
This study cannot address if multiple work exposures to VGDFs increase the risk of developing RA. Further studies are needed to address this important question. An increasing titre of RF in the general population increases the incidence of RA development by 20-fold when comparing the lowest versus highest titre of RF.30 We suggest that studies of RF in the general population and the risk of developing RA consider the smoking history and occupational inhalations.
It is well established that smoking blunts clinical response to RA treatment with both methotrexate and tumour necrosis factor (TNF) inhibitors,31 32 and higher levels of RF in patients with RA with established disease receiving TNF inhibitors are much less likely to be in remission at 12 months follow-up.33 We suggest that patients with RA exposed to VGDF will have a more pronounced blunting of response to conventional treatment due to high RF levels, generated by sequential inhalational insults.
Prospective, large-scale multicentre studies of patients with RA using occupational classification criteria and job exposure matrices may help to determine if occupational exposures in never smokers increase RF levels, increase disease activity and affect treatment response. Cohort studies using similar detailed exposure classification criteria may compare respiratory mortality rates among RA and non-RA cases with the same exposures, as it has been demonstrated that exposures to both smoking and VGDF greatly increase the risk of COPD in the general population with an OR of 14.1 (9.33–21.2) compared with never smokers with no such work exposures.10 If our findings are representative, this is likely to be highly relevant to the comorbidity and mortality of male RA.
Given the single-centre nature of this study, we cannot comment on how representative this male RA cohort compares with a wider RA population and suggest that wider study is needed. We suggest that rheumatologists undertake a detailed occupational and smoking history when assessing patients with RA.
Conclusion
The overwhelming majority of RA men is this analysis of an entire University Hospital male RA cohort had exposure to vapours, gas, dust or fumes and had been smokers before diagnosis. Men who had such exposures combined had significantly higher RF titres and were diagnosed at a significantly younger age. Given the prevalence of these exposures in an RA male cohort, further study is needed to uncover the pathophysiological mechanisms underlying these compelling findings as the environmental exposures driving the autoantibody generation seen here may affect response to treatment.
Acknowledgments
The authors would like to thank Professor Karen Walker-Bone for input on questionnaire design. The authors would like to thank the focus group patients in setting and informing the research agenda and the wider patient group of male patients with rheumatoid arthritis agreeing to complete this study.
References
Footnotes
Contributors DM: conceptualisation, data curation, formal analysis, investigation, methodology, project administration, resources, software, validation, writing—original draft and writing—review and editing. KB: data curation, investigation, project administration, software, validation and writing—review and editing. DH: conceptualisation, funding acquisition, methodology, project administration, supervision, visualisation and writing—review and editing.
Funding The authors would like to thank the Cornwall Arthritis Trust, a not-for-profit charity for ongoing support research into occupations and rheumatoid arthritis and support for financing open publication of data. Cornwall Arthritis Trust’s patient focus group were involved in setting the research question and were informed of the study design, having input into follow-up arrangements of patients who may not have been able to respond in writing.
Disclaimer Cornwall Arthritis Trust played no part in the collection, analysis and interpretation of the data; in the writing of the report and in the decision to submit the paper for publication.
Competing interests None declared.
Patient consent Not required.
Ethics approval South West regional ethics comittee IRAS ID 194833.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Due to Hospital Trust ethical restrictions, some data cannot be made available publicly. Data are available on application to the Royal Cornwall Hospitals Trust R&D department as Sponsor, responsible for Institutional Data Access, for researchers who meet the criteria for access to such data. Data can be requested from Mr Nick Morley, Research Manager at Royal Cornwall Hospitals Trust. Email: Tel 01872256422 nickmorley@nhs.net.