Article Text

Abstract
Introduction Despite advances in infection prevention and control, catheter-associated urinary tract infections (CAUTIs) are common and remain problematic. Prolonged urinary catheterisation is the main risk factor for development of CAUTIs; hence, interventions that target early catheter removal warrant investigation. The study’s objectives are to examine the efficacy of an electronic reminder system, the CATH TAG, in reducing urinary catheter use (device utilisation ratio) and to determine the effect of the CATH TAG on nurses’ ability to deliver patient care.
Methods and analysis This study uses a mixed methods approach in which both quantitative and qualitative data will be collected. A stepped wedge randomised controlled design in which wards provide before and after observations will be undertaken in one large Australian hospital over 24 weeks. The intervention is the use of the CATH TAG. Eligible hospital wards will receive the intervention and act as their own control, with analysis undertaken of the change within each ward using data collected in control and intervention periods. An online survey will be administered to nurses on study completion, and a focus group for nurses will be conducted 2 months after study completion. The primary outcomes are the urinary catheter device utilisation ratio and perceptions of nurses about ease of use of the CATH TAG. Secondary outcomes include a reduced number of cases of catheter-associated asymptomatic bacteriuria, a reduced number of urinary catheters inserted per 100 patient admissions, perceptions of nurses regarding effectiveness of the CATH TAG, changes in ownership/interest by patients in catheter management, as well as possible barriers to successful implementation of the CATH TAG.
Ethics and dissemination Approval has been obtained from the Human Research Ethics Committees of Avondale College of Higher Education (2017:15) and Queensland Health (HREC17QTHS19). Results will be disseminated via peer-reviewed journals and conference presentations.
Trial registration number ACTRN12617001191381 (Pre-results).
- healthcare-associated infection
- catheter-associated urinary tract infection
- cath tag
- infection control
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to investigate the use of a novel electronic device as a reminder intervention to reduce urinary catheter use and the burden of catheter-associated urinary tract infections.
Stepped wedge randomised controlled design maximises feasibility and statistical power.
Minimal risk for participants.
Results that will inform infection prevention and control practice and guidelines internationally.
Data collection is limited to one Australian hospital.
Introduction
Urinary tract infections (UTIs) are one of the most frequently reported healthcare-associated infections globally.1–3 The majority of healthcare-associated urinary tract infections (HAUTIs) are related to urinary catheters, which are estimated to be placed in up to 26% of patients admitted to hospitals.4 HAUTIs, including catheter-associated urinary tract infections (CAUTIs), are associated with increased morbidity and mortality and prolonged hospital stay.5 6 Furthermore, they are associated with higher risk of antimicrobial resistance, which complicates treatment.7–10 In addition to their clinical consequences, CAUTIs are costly to patients and health systems. In the USA, symptomatic episodes of CAUTIs may add an estimated US$1200–US$4700 to patient costs.3 In Australia, hospital-acquired UTIs were estimated to contribute an additional cost of $A24.7 million to the hospital system.11 An estimated 380 000 infections and 9000 deaths attributed to CAUTIs each year may be preventable through the use of effective infection prevention and control strategies.3 However, despite advances in infection prevention and control, CAUTIs remain problematic,12 hence further research is needed to identify ways to reduce the burden they create.4 13–16
Prolonged urinary catheterisation has been identified as the greatest risk factor for CAUTIs.16 Indwelling urinary catheters are often placed unnecessarily, lack documented reasons for insertion and are not promptly removed when no longer warranted.16 A national study of US hospitals that examined current practices used by hospitals to prevent HAUTIs found that 56% of hospitals did not have a system for monitoring which patients had urinary catheters placed and 75% did not monitor catheterisation duration.17 When a urinary catheter remains in situ, the daily risk of acquiring bacteriuria is estimated to range from 3% to 7%.18 An intervention that prompts removal of catheters at the earliest opportunity when they are no longer medically indicated should therefore be an effective method for reducing urinary catheterisation duration and preventing subsequent development of CAUTIs.19
Maintaining awareness of the continued presence of urinary catheters is a key step towards initiating prompt removal of catheters as healthcare staff may be unaware of the catheters’ existence.20 Hence, interventions that promote frequent reminders about catheters are needed. A reminder intervention is a mechanism used to remind either a physician or nurse that the catheter is still in place and that removal may be warranted if the catheter is no longer required.16 A systematic review and meta-analysis that evaluated the effect of urinary catheter reminder systems on urinary catheter use and CAUTI rates was published in 201016 and updated in 2013.20 In both reviews, the benefit of reminder systems in reducing urinary catheter use and CAUTIs was demonstrated. Catheter reminder interventions evaluated in these studies included verbal or written reminders, a sticker on the catheter bag or patient’s chart, computer-generated reminders or stop orders.16 20 However, no studies investigating the use of an electronic device as a reminder intervention were identified.
The frequency of unnecessary and prolonged catheter use, subsequent increase in the risk of CAUTIs, along with its clinical and financial implications in Australia and worldwide, provide a strong rationale for a novel method to reduce urinary catheter use and the burden of CAUTIs. To date, in Australia, there is limited research on interventions aimed at reducing urinary catheter use with no rigorously designed studies undertaken. Addressing this gap in knowledge, the two main objectives of the present study are to: (1) examine the efficacy of an electronic reminder system, the CATH TAG, to reduce the urinary catheter device utilisation ratio in hospitalised patients and (2) to determine whether the CATH TAG has an effect on nurses’ ability to deliver patient care.
Methods
Study design
A mixed methods approach will be used, including both quantitative and qualitative data collection. For quantitative data collection, a stepped wedge randomised controlled design in which clusters provide before and after observations21 will be undertaken in one hospital over a 24-week period (figure 1). The clusters in the study are individual hospital wards. The design includes an initial baseline period where no wards are exposed to the intervention.21 Subsequently, at regular intervals, two wards forming two clusters will cross over from the control phase to the intervention with the process continuing until all enrolled wards have crossed over.21 There will be a random sequential allocation of the intervention to the wards, that is, each enrolled ward will be introduced to the intervention two at a time, approximately every 4 weeks until week 20, when all wards would have been exposed to the intervention. The study design enables each ward to act as its own control, which mitigates the potential for some confounders such as variations in ward size and case mix. Staggered commencement and duration of the intervention supports feasibility while maintaining the rigour of the study.22 This design will allow research staff to work with individual wards as they change over, maximising consistency of the intervention and aiding implementation.22 In addition, data collection continues throughout the study, so that each cluster contributes observations under both control and intervention observation periods. In month 6 of the study, qualitative data will be collected through an online survey administered to nursing staff. Approximately 2 months after the study is completed, a focus group comprising nurses will be conducted to obtain additional qualitative data about the nurses’ perceptions of how the CATH TAG was used in practice.

Study design overview. Blue=control phase; green=intervention phase.
Study setting
One Australian hospital with an intensive care unit and over 30 000 patient admissions per year will be enrolled in the study using convenience sampling.
Recruitment of hospital
The recruitment process will purposively invite eligible hospitals to participate through stakeholder and partner networks. The first confirmed hospital will be accepted.
Ward-level inclusion and exclusion criteria
Potential wards and units eligible for inclusion are medical wards, surgical wards and intensive care units.
Day-stay units and psychiatric wards will be excluded.
Patient-level inclusion and exclusion criteria
All patients in eligible wards of the hospital who have an indwelling urinary catheter administered as part of their usual clinical care will be included.
Neonates (<2 years old) may be excluded if the CATH TAG is too large for the catheter bag or interferes with patient care.
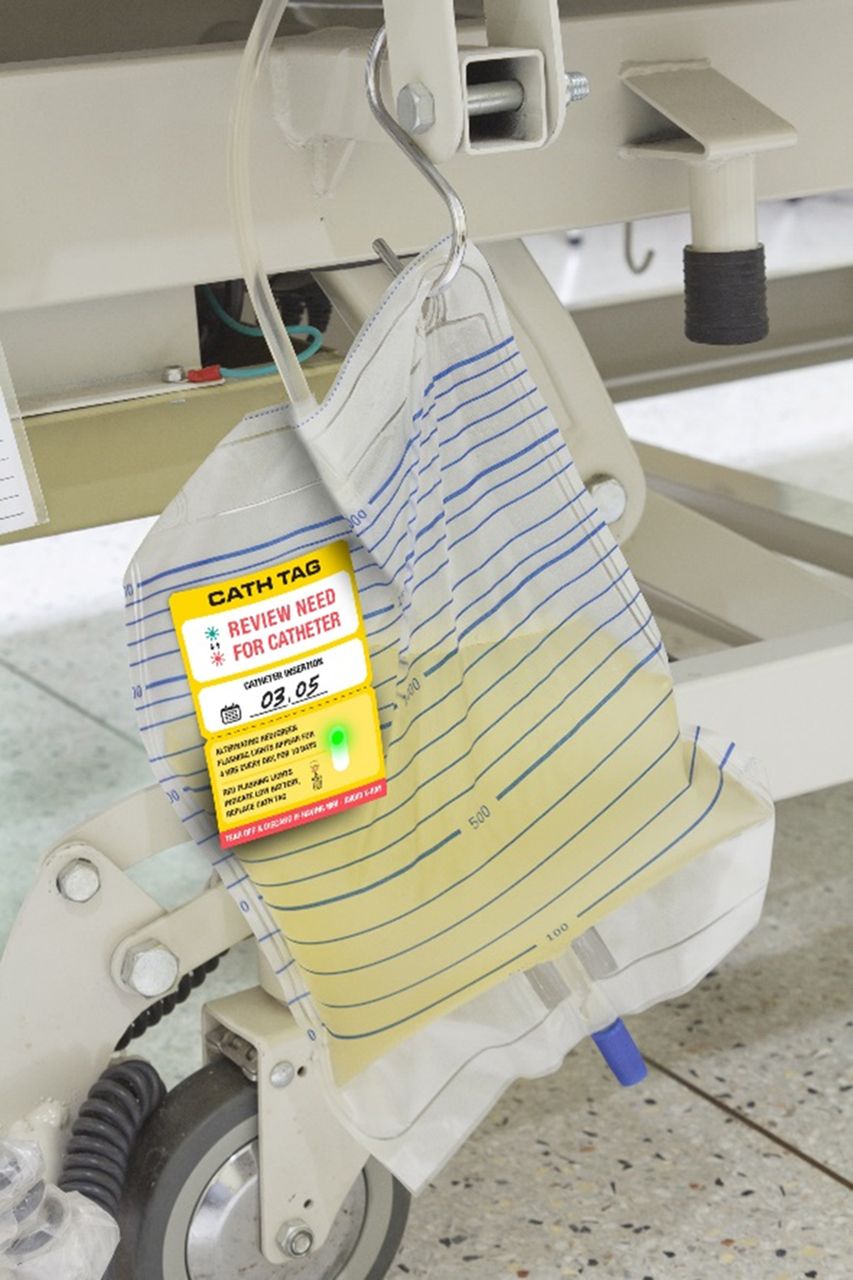
Intervention
The intervention is the use of the CATH TAG (figure 2). The CATH TAG is an electronic device in the form of a sticker that adhesively attaches to the catheter bag. It weighs approximately 5 g and has a non-intrusive green light that flashes intermittently for a period of 24 hours on activation. After 24 hours, the green flashing light changes to red, flashing with increased rapidity and visibility. The light will flash red for 4 hours and subsequently change back to green, slower flashing, restarting the cycle. The red flashing light is an indication for the nurse to reassess the need for a urinary catheter and remove it if no longer required. This cycle will continue for 10 days and then change permanently to the red flashing light to indicate that the battery of the CATH TAG is exhausted. There is no option for nurses to manipulate the flashing light or amend the flashing cycle.

The CATH TAG attached to a catheter bag.
Implementing the intervention
Randomisation and blinding
Eligible wards in the hospital will be randomly assigned to cross over to the intervention every 4 weeks over the trial duration of 24 weeks. If no clustering, the sample size for 80% power at 0.05 significance would be 816. Allocation of wards to the intervention will be concealed. Computer-generated randomisation of the crossover dates for the wards will be performed independently by one of the investigators, who will not be involved in assessment or delivery of the intervention. All included wards will be provided with sufficient notice of the dates to cross over to the intervention. Wards will not be blinded, because it is not feasible to blind staff to the intervention.
Implementation
In the week prior to the intervention commencing, information sessions about the study will be provided to the participating hospital and staff. A variety of methods will be used to further alert staff and raise awareness about the intervention prior to it being rolled out. These methods include placing wall posters in wards and key locations, handing out flyers and information leaflets as well as branded promotional material, such as pens. Nurses will be trained to use the CATH TAG.
Control phase
During the control phase, usual practice regarding catheter care and removal will occur, according to local policy or process guidelines. No electronic or alert systems for catheter removal will be used.
Intervention phase
Every 4 weeks, after an initial control phase with no intervention, two wards will cross over to the intervention. With commencement of the intervention on the ward, a CATH TAG will be attached to every urinary catheter bag.
For patients who are transferred from a control ward to an intervention ward, a CATH TAG will be attached to their urinary catheter on transfer. For patients who are transferred from an intervention ward to a control ward, the CATH TAG will be removed on transfer.
When a ward transitions to the intervention, a CATH TAG will be attached to all new catheter insertions. This includes transfers of patients with a urinary catheter to the transitioning ward. Patients who had a urinary catheter inserted before the transition date will not receive a CATH TAG on their urinary catheter bag to prevent non-independence of observations and to increase feasibility of the implementation of the intervention in the hospital. Their data will contribute to the control group data set.
Outcome measures
The outcomes for each objective of the study are outlined in table 1.
Key outcome measures
Definitions
Catheter-associated asymptomatic bacteriuria (CA-ASB) is defined as the presence of ≥105 colony forming unit (cfu)/mL of ≥1 bacterial species in a single catheter urine specimen in a patient without symptoms compatible with UTI.23
Data collection
Urinary catheter data
Data will be collected by an appointed staff member at the hospital, supported by the research team. If data collection results in increased workload for the hospital staff, the research team will provide additional resources in the form of funding to cover additional hours for the staff member or employment of a second staff member for the purpose of data collection. For the purpose of this protocol, the hospital staff member(s) undertaking data collection will be referred to as hospital personnel. The research team will provide the hospital personnel with training about the project, data collection processes and data collection tools, as well as ongoing on-site and telephone support. Figure 3 summarises the data collection process.

{kind=link}
{kind=link}
{kind=link}
Overview of data collection process.
Hospital personnel will visit inpatient areas, and patients who receive an indwelling urinary catheter will be identified and followed up until discharge or catheter removal. Hospital personnel will check that a CATH TAG has been attached to every catheter bag, on wards that have crossed over to the intervention. A review of medical notes and microbiology laboratory records will be undertaken by the hospital personnel for each patient who receives a catheter and has a urinary sample taken. Data to be collected at the time of visit of the hospital personnel to the ward include: hospital number, date and time of catheter insertion, date and time of catheter removal, use of CATH TAG (yes/no). Additional patient data collected include: age, sex, date of admission, reason for censoring follow-up, date and time of discharge or catheter removal, designation of person inserting the catheter and ward. If a patient has a positive urine culture after catheterisation and prior to removal, the following data will be collected: date of specimen collection, organism(s) isolated, cfus and white cell count. Online supplementary file A provides a detailed list of types, sources and timing of data to be collected.
Supplemental material
The number of catheter days for each patient included in the study will be estimated from the date and time of catheter insertion to the date and time of removal. Hospital personnel will record all captured data locally on a spreadsheet, designed by the research team specifically for the purpose of the study.
Survey data
Data collection will involve the use of a structured anonymous survey administered using an online tool. Nurse participants will be asked a series of questions that relate to their perceptions about ease of use of the CATH TAG, their views on effectiveness of the CATH TAG, an exploration of their perceptions of change in ownership or interest by patients in catheter management and any barriers to the CATH TAG working successfully that nurses might be experiencing, forming the following four dimensions, based on the objectives of the study:
Ease of use.
Effectiveness.
Perceived changes in ownership regarding patients’ healthcare.
Barriers.
Items exploring those dimensions will be presented to participants in the form of statements, to be answered on a 5-point Likert scale, as well as in the form of open questions and yes/no questions to investigate possible themes for the focus group.
Additionally, demographic information about the participants will be collected, including the ward on which they primarily work, age, gender, years of nursing experience (postqualification) and their highest (completed) qualification. No identifiable or reidentifiable information will be collected.
Focus group data
Participants in the focus group will be limited to approximately six to eight nurses to ensure the group can be run effectively. If required for the purposes of data saturation, a second focus group might be run to ensure representation from more wards. The focus group will be conducted in a location other than the ward on which the participants work. A person with relevant training and experience will lead the group discussion. An exploration of experiences of the CATH TAG users will be undertaken using a series of questions to prompt discussion. The questions will be designed to validate the broad responses and themes received in the online survey and provide the opportunity for in-depth feedback not otherwise possible from the online survey.
The timing of this focus group is important. As this study adopted a staggered approach to implement the intervention, scheduling the focus group towards the end of the study will enable the researchers to capture the participants’ responses after staggered levels of involvement in use of the CATH TAG.
To further understand the participants’ experience using the CATH TAG, the focus group questions will aim to capture information about the personal experiences of the hospital personnel and their construed perceptions of patients’ perceptions, regarding the use and effectiveness of the CATH TAG. The objective of the focus group is to acquire maximum in-depth feedback about the CATH TAG. In combination with the quantitative analysis of the survey data and the catheter data collected, gathering qualitative data by conducting a focus group contributes to a more holistic measure of the experience of the CATH TAG. In so doing, we considered the end-user perspective. The focus group provides the researchers with the unique opportunity to receive suggestions for improvement of the CATH TAG based on the participants’ experiences. Participants will be asked to provide responses to questions about the following issues, including both their own perceptions about use of the CATH TAG as well as their construed perceptions of patients’ response to its use:
Perceived ease of use of the CATH TAG.
Perceived impact of the CATH TAG on patient care (effectiveness).
Perceived impact on interactions with patients as a result of using the CATH TAG.
Perceptions of patients’ experiences with, interest in and reactions to use of the CATH TAG.
Perceptions of impact on patients’ ownership of their own healthcare as a result of using the CATH TAG.
Perceived barriers to using the CATH TAG.
Additional issues that emerge from analysis of the participants’ survey responses.
The focus group will be audio-recorded, with the permission of participants, to enable thematic analysis of the discussion at a later date. No identifiable or reidentifiable information provided during the focus group will be linked to any participant.
Recruitment of participants for survey and focus group
Nurses have been chosen as the participants for the survey and focus group as they have the primary role in day-to-day urinary catheter management and care. In order to recruit nurses to participate in an online survey, information leaflets will be distributed to each participating ward during month 6 of the study. If approved by the hospital, the same information will be sent to nurses via email. Other communication methods such as a ward communication diary, a reminder at a staff meeting or during handover may also be used.
The information leaflet/email will contain details about the survey and a web link (presented as a URL or alternatively as a QR code) to participate. Additional information regarding the study, in addition to a consent form, will be included at the beginning of the survey. To improve response rates, an incentive of 10 $A40 gift cards will be made available and will be allocated at random to those who complete the survey. To enter the draw for a gift card, participants will need to click on a separate web link provided at the end of the survey. This will ensure that no personal details are linked to the survey.
To recruit participants for a focus group, the participants will be provided with an opportunity to indicate their interest by registering their name at the end of the online survey by clicking on a separate web link. Again, this will ensure that no personal details are linked to the survey. Focus group participants will receive an $A80 gift card to compensate them for their time. If more nurses register for the focus group than are required, purposive sampling will occur to ensure a representative sample of different wards. If it remains such that there are still too many registered than can be enrolled, participants will be chosen at random within each representative sample group. The focus group will be conducted 2 months after completion of the intervention (the eighth month of the study). Prior to or on the day of the focus group, information regarding the study will be provided, in addition to obtaining informed consent.
Data monitoring and management
Data monitoring will be overseen by the chief investigator, and the data monitoring committee consists of all investigators on the study. Data will be stored electronically in a secure location at the administering institution. Data quality will be enhanced by the provision of a data collection form and quality checks by the project manager. A data collection guide has been developed to aide and document this process. Any approved changes to the study protocol will be updated in the Australia New Zealand Clinical Trial Registry.
Sample size and power estimation
The population at risk has been defined as patients receiving urinary catheters in hospital. Based on pilot work, an estimated 25% of patients on admission will receive a catheter.4 We estimate that, at baseline, the median duration of catheterisation is 4 days (equivalent to a 50% probability that a catheter will be in situ on day 4).24 We aim to detect a difference of 20% relative risk (10% absolute risk) reduction in catheterisation on day 4 using a stepped wedge design.21 It is assumed the intraward correlation in catheter duration is ρ=0.1. Based on pilot work, it is anticipated that there will be 50 patients with a catheter per month on each ward, and the study will be for 6 months.4 A power calculation was performed using the stepped wedge module in Stata.25 This accounts for both the clustering in outcomes by ward, as well as the crossover design of the study.21 26
At a significance level of 0.05, 2100 patients (10 clusters (wards), with two clusters implementing the intervention at each month) will be required to demonstrate a change in the probability of a catheter being in situ on day 4 from 50% to 40% with a power of 81%. Similar power would be expected with 35 patients with catheters per month in 10 clusters, with two clusters implementing the intervention each month (n=2100, power 81%).
Data analysis
Objective 1
Analysis will be by an intention-to-treat strategy, and this will involve inclusion of all patients in the randomised clusters in the analysis regardless of any deviations from the study protocol.27 Descriptive statistics will be used to summarise the characteristics of the study sample. Analysis will be performed using the generalised estimating equations, using the duration of catheterisation as the dependent variable and intervention as the independent variable. The confounding effect of calendar time on intervention exposure will be adjusted for in the analysis. We will consider time at risk for the control and intervention periods separately for patients present at the time of the crossover. The use of the analysis considering clustering at the ward level implicitly accounts for the non-independence of these patient observations. It is anticipated that duration of catheterisation will be log-normally distributed, but exploratory analyses (and where necessary transformation) will be performed. Robust SEs will be used to adjust for correlation at ward level and autocorrelation in time. There is no expected delay in the effect of the intervention on the outcome.
Analyses of secondary outcomes of the number of cases of CA-ASB per 100 catheter days and number of urinary catheters inserted per 100 patient admissions will also be undertaken, and these outcomes will be compared from data collected preintervention and postintervention. A sensitivity analysis will exclude the first month following implementation, and a subgroup analysis will consider medical and surgical wards separately.
Objective 2
Survey
Data from the online survey will be analysed quantitatively using SPSS. It is anticipated that data will be normally distributed, but exploratory analyses will be performed, including testing of assumptions of linearity, homoscedasticity, multicollinearity and normality of errors and if necessary transformation of data. Validity and reliability of the survey will be assessed, as outlined in further detail below. During development of the survey items, experts have been consulted to ensure face validity. Construct validity will be measured by respectively correlating nurses’ scores on three general items included in the survey for this purpose. To approach criterion validity, the predictive validity of the survey will be assessed by comparing survey data with focus group data, that is, by predicting the attitude of nurses towards the CATH TAG in the focus group, based on nurses’ attitudes towards the CATH TAG, measured by the survey. Reliability will be determined by calculating Cronbach’s α using SPSS. Subsequently, a general satisfaction score and individual satisfaction scores for the four dimensions of nurses’ experiences with the CATH TAG (ease of use, effectiveness, changes in ownership and barriers) will be calculated. Regression analysis will be conducted to determine if the duration of the intervention or the ward that nurses primarily work on had an effect on nurses’ experiences with the CATH TAG. Any problems reported in the open questions will be taken into the focus group to be discussed and subsequently analysed qualitatively.
Focus group
Data gathered from the focus group will be managed using qualitative software (NVivo). The data analysis process will aim to identify and investigate both predetermined and emerging themes in the data. Each piece of qualitative data will be systematically treated by being labelled with a meaningful code. The predetermined themes will be drawn from the broad responses to the open questions in the survey, as well as from the study’s objectives and will be reflected in the focus group questions. Furthermore, thematic analysis will be used to establish emerging themes in the qualitative data gathered during the focus group. This process of considering both predetermined and emergent themes reduces redundancy in the analysis results by collapsing similar themes, identifies any relationships between the themes and ensures saturation is achieved. In this way, the essence of the hospital personnel’s perceptions will be determined. Data saturation will be achieved when no new data, no new themes, no new coding and ability to replicate the study is achieved. One focus group is planned; however, a second will be undertaken if required (to achieve saturation).
Patient and public involvement
Patients and/or public were not involved in the development of this study protocol. However, patients’ perspectives and interaction with the CATH TAG will be explored as part of the focus group.
Ethics and dissemination
Ethics
Any risks or harms associated with the study will be reported to the relevant human research ethics committee (HREC). Reporting of the study and progress, including any audits, will be conducted consistent with the requests of the HRECs who approved the study. Any modification to the study that has ethical implications will be forwarded to the HRECs for approval. Only the chief investigator and coinvestigators will have full authority to access the data collected. No identifiable or reidentifiable patient data will be collected by the investigators, thereby protecting anonymity and confidentiality of participants.
Informed consent
A waiver of individual patient consent has been obtained for this study from the relevant HRECs. No intervention is directly administered to patients, rather an addition to existing procedures regarding catheter removal is being undertaken. Consent will be obtained from participants in both the online survey and focus group. Participants undertaking the survey and/or focus group can withdraw their participation at anytime without being disadvantaged.
Dissemination
Results will be published in peer-reviewed journals, presented at relevant conferences and communicated via professional networks. The study protocol has been presented at the 2017 Infection Prevention Society Conference, Manchester, UK and the 2017 Australasian College for Infection Prevention and Control Conference, Canberra, Australia.
Discussion
Urinary catheters are important medical devices for patient management.28 However, unnecessary and prolonged use of these devices poses an important risk to patient safety as they have the potential to result in both infectious and non-infectious complications.29 30 Therefore, interventions aimed at reducing urinary catheter use should be investigated. To our knowledge, this is the first randomised controlled study evaluating the effectiveness of a novel electronic reminder device, the CATH TAG, in reducing urinary catheter usage in hospitalised patients.
Confounders
Potential confounders include the effect from different staff inserting and caring for patients with an indwelling catheter and the indications for urinary catheterisation. The design of this study minimises many of these issues, as wards (clusters) act as their own control. Furthermore, there is no reason to suggest a fundamental change in the control and intervention periods for these variables. Given the potential for secular changes in the outcome due to the influence of external forces such as changes in healthcare delivery, calendar time might have a confounding effect on intervention exposure and will be adjusted for in the data analysis.31 A Hawthorne effect32 may occur from study awareness and impending rollout of the intervention in each ward, thereby increasing diligence in catheter maintenance that may lead to possible ‘contamination’ of the intervention. To reduce this potential bias, educational events and training on the use of the CATH TAG will be staggered and delivered to wards individually in the week prior to implementing the intervention. In addition, any change in the primary outcome in the lead up to the intervention will be modelled and taken into account in the analysis.
Furthermore, nurses working on a casual basis or across wards have the potential to provide responses to the survey or focus group from a range of perspectives based on their experiences on different wards. To minimise this, the survey will focus the respondent to experiences in one particular area and obtain details about their exposure to working in different hospital wards or units.
Strengths
The study is strengthened by the use of a stepped wedge randomised controlled design in which clusters provide before and after observations. This design has been found to be particularly useful in studies evaluating intervention effectiveness during routine implementation such as this study where the insertion of a urinary catheter is considered to be part of the usual care of the patient.33 The study design also improves feasibility and enables each individual ward to act as its own control, which removes the potential for some confounders such as variations in ward size and case mix. Furthermore, the stepped wedge design is useful in pragmatic research such as that undertaken in this study where the researchers wish to gain a first estimate of the efficacy of the CATH TAG in a clinical setting, and staggered implementation of the intervention is therefore appropriate.34
Limitations
Data collection is limited to one Australian hospital. There might be variations in hospital size and case mix that influence the effectiveness and feasibility of the CATH TAG.
Trial status
The study team is finalising hospital recruitment. The trial is due to commence in late 2017.
Acknowledgments
The authors would like to acknowledge Victoria Gregory for her assistance as project manager.
References
Footnotes
Contributors OF and HR drafted the initial manuscript. All authors made contributions to the development of the manuscript and were involved in revising it critically for important intellectual content. BGM is chief investigator and provides expertise in infection control. ACC and PLR provided expertise in clinical epidemiology. BGM and ACC provide expertise in statistics and quantitative data analysis. MN is responsible for qualitative data analysis. OF provides expertise in urinary tract infection and was responsible for protocol development. All authors have approved the final manuscript.
Funding This study is supported by an industry grant provided by Senver. Responsibility for the study design, conduct, data collection, analysis and interpretation are solely the responsibility of the authors.
Competing interests None declared.
Patient consent Not required.
Ethics approval This study has been approved by the Avondale College of Higher Education Human Research Ethics Committee (HREC) (2017:15) and the Queensland Health HREC (HREC17QTHS19).
Provenance and peer review Not commissioned; externally peer reviewed.