Article Text

Abstract
Objective To assess the impact of behaviour modification interventions to promote restrictive red blood cell (RBC) transfusion practices.
Design Systematic review and meta-analysis.
Setting, participants, interventions Seven electronic databases were searched to January 2018. Published randomised controlled trials (RCTs) or non-randomised studies examining an intervention to modify healthcare providers’ RBC transfusion practice in any healthcare setting were included.
Primary and secondary outcomes The primary outcome was the proportion of patients transfused. Secondary outcomes included the proportion of inappropriate transfusions, RBC units transfused per patient, in-hospital mortality, length of stay (LOS), pretransfusion haemoglobin and healthcare costs. Meta-analysis was conducted using a random-effects model and meta-regression was performed in cases of heterogeneity. Publication bias was assessed by Begg’s funnel plot.
Results Eighty-four low to moderate quality studies were included: 3 were RCTs and 81 were non-randomised studies. Thirty-one studies evaluated a single intervention, 44 examined a multimodal intervention. The comparator in all studies was standard of care or historical control. In 33 non-randomised studies, use of an intervention was associated with reduced odds of transfusion (OR 0.63 (95% CI 0.56 to 0.71)), odds of inappropriate transfusion (OR 0.46 (95% CI 0.36 to 0.59)), RBC units/patient weighted mean difference (WMD: −0.50 units (95% CI −0.85 to −0.16)), LOS (WMD: −1.14 days (95% CI −2.12 to −0.16)) and pretransfusion haemoglobin (−0.28 g/dL (95% CI −0.48 to −0.08)). There was no difference in odds of mortality (OR 0.90 (95% CI 0.80 to 1.02)). Protocol/algorithm and multimodal interventions were associated with the greatest decreases in the primary outcome. There was high heterogeneity among estimates and evidence for publication bias.
Conclusions The literature examining the impact of interventions on RBC transfusions is extensive, although most studies are non-randomised. Despite this, pooled analysis of 33 studies revealed improvement in the primary outcome. Future work needs to shift from asking, ‘does it work?’ to ‘what works best and at what cost?’
PROSPERO registration number CRD42015024757.
- systematic review
- red blood cell transfusion
- restrictive transfusion threshold
- behaviour modification
- implementation intervention
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- systematic review
- red blood cell transfusion
- restrictive transfusion threshold
- behaviour modification
- implementation intervention
Strengths and limitations of this study
In this systematic review and meta-analysis, 84 studies examining single and multimodal interventions to modify red blood cell transfusion practices were identified.
This is the most comprehensive systematic review and the first meta-analysis of these interventions to date.
Included studies were of low to moderate quality and almost all were designed as non-randomised, before and after studies.
No studies examined the comparative effectiveness between behaviour modification interventions, nor the cost-effectiveness of interventions.
There was significant statistical heterogeneity and evidence for publication bias.
Introduction
Blood transfusions are commonly administered as a life-saving therapy to restore haemoglobin levels among patients with severe anaemia.1–3 Blood and blood products, such as red blood cells (RBCs), are, however, scarce and expensive health resources that must be managed carefully to ensure judicious use and availability for those most in need of transfusions.4 Beyond blood conservation, transfusion safety and reducing the adverse events associated with transfusion must be considered. RBC transfusions have been associated with increased risk of infections, acute transfusion reactions and in certain cases, mortality.5–7 High-quality evidence has accumulated over the past two decades in support of reducing patient exposure to RBC transfusions, through the adoption of more restrictive RBC transfusion thresholds.8–12 A number of guidelines, such as those most recently released by the AABB (formerly the American Association of Blood Banks),13 have also recommended against transfusion if haemoglobin levels are above 7–8 g/dL for most patients groups.
It is well documented that publication of such evidence alone is insufficient for affecting change.14 Clinical practice is influenced by a myriad of social, cultural and environmental factors that are not necessarily considered in guidelines.15 Concerted change management efforts are, therefore, commonly undertaken to actively address these factors in order to implement recommended guidelines and achieve the desired practice change.
Interventions to specifically modify provider transfusion practices, such as education, audit and feedback, and computerised or paper order entry systems, have been described in prior studies.16–19 Previous systematic reviews have examined the impact of these interventions, alone or in combination, on transfusion practices for various blood components (eg, RBCs, fresh frozen plasma, platelets, cryoprecipitate). The findings of these syntheses report variability in outcomes—including a paucity of economic outcomes—and limitations in both the quality of evidence and breadth of interventions examined.16–18 With the exception of one systematic review published in 2015 that exclusively focused on the impacts of electronic decision support,18 these previous reviews are dated (last published in 2005).16 17
Therefore, a de novo systematic review synthesising the current literature in this area, concentrating on all behaviour modification interventions targeting RBC transfusion practices, is useful as healthcare organisations respond to meet recent RBC transfusion guideline recommendations. The objective of this study was to determine the effectiveness of behaviour modification interventions that change RBC transfusion practices, specifically, the effects of interventions on the proportion of patients transfused, as well as patient and healthcare system outcomes.
Materials and methods
A systematic review of the published literature was completed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (online supplementary file 1).20 The protocol for this systematic review is registered on the International Prospective Register for Systemic Reviews website (2015:CRD42015024757; online supplementary file 2).21
Supplementary file 1
Supplementary file 2
Search strategy
The electronic search strategy was developed by an Information Specialist (DLL). MEDLINE, PubMed, EMBASE, the Cochrane Central Registry of Controlled Trials, the Cumulative Index to Nursing and Allied Health, the Cochrane Database of Systematic Reviews and the Health Technology Assessment database were searched from inception to 12 January 2018. A sample search strategy is available in online supplementary file 3. Animal studies, case reports, comments, editorials and letters were excluded; no other limitations were applied. The references lists of identified systematic reviews were also hand searched for relevant articles not found through database searches.
Supplementary file 3
Selection of literature
Studies were included if they: reported original data; examined the impact of a behaviour modification intervention on healthcare provider RBC transfusion practices; had a comparator group (eg, no intervention or another intervention) and were designed as either a randomised controlled trial (RCT) or non-randomised study. A non-randomised study involves the selection of groups each exposed to a different intervention without random assignment.22 23 Common non-randomised designs in behaviour modification studies include non-randomised trials (also referred to as between subjects or between group trials), time series studies, and uncontrolled and controlled before and after studies.23 24 No fixed definition of a behaviour modification intervention was applied; thus, any definition used within the included studies was accepted. Included interventions were grouped using an inductive approach based on descriptors and labels provided from the studies themselves. Studies were excluded if they did not meet any of the above criteria, including if they only assessed transfusion of other blood products (ie, fresh frozen plasma, platelets, cryoprecipitate) and not in conjunction with RBCs. Detailed inclusion and exclusion criteria are provided in online supplementary file 4. Abstract and full-text screening were completed in duplicate (LJJS, LED, HMH, KM) and any disagreement was resolved through discussion and consensus, or through consultation with a third reviewer. Agreement between reviewers was calculated using a kappa statistic.
Supplementary file 4
Data extraction
Data extraction was completed in duplicate using a standardised data extraction form (LJJS and KM). Data on publication date, country, healthcare setting, study design, follow-up period, type of intervention and comparator groups, intervention characteristics, RBC transfusion criteria, definition of an ‘inappropriate’ transfusion, number of patients treated in each group and the primary outcome of interest (the proportion of patients transfused) were extracted. Secondary outcomes, including the proportion of inappropriate transfusions, mean RBC units transfused per patient, in-hospital mortality, hospital length of stay (LOS), pretransfusion haemoglobin and changes in costs (eg, RBC unit costs) were also extracted where available.
Quality assessment
Risk of bias and quality assessments of included studies were completed in duplicate (LJJS and KM). The Cochrane Risk of Bias tool was used to evaluate the risk of bias among included RCTs.25 Quality of non-randomised studies were assessed using the Downs and Black Checklist.26 Typically scored out of 28 points, the Downs and Black Checklist was modified because several items do not apply to the non-randomised studies (eg, randomisation), thereby reducing the denominator to 22 for uncontrolled before and after studies, and 23 for controlled before and after and non-randomised trials.
Data analysis
Meta-analyses were conducted using a random-effects model. Pooled odds ratios (ORs) and weighted mean differences (WMDs), and their respective 95% CIs were calculated for categorical and continuous outcomes, respectively. Stratified analyses by intervention type and study design were completed. Statistical heterogeneity was examined using both the I2 (percentage of total interstudy variation due to heterogeneity rather than chance) and Q statistic p value (test of homogeneity). An I2 greater than 50% was considered as evidence for significant heterogeneity.27 Random-effects meta-regression was performed with the year of publication, the number of interventions per study, having a multimodal intervention, a study setting in a single unit or clinical service, follow-up period (greater than 1 year) and each of the identified intervention types as covariates. A regression coefficient with a p<0.10 was considered a significant predictor of the primary outcome. Publication bias was examined using Begg’s funnel plot and Egger’s regression test. In the case of funnel plot asymmetry, the trim-and-fill method was used to impute estimates from potentially suppressed publications. This method assumes that studies that do not demonstrate a desired effect (eg, decrease in proportion transfused) were not likely published.28 All statistical analyses were completed using Stata/IC V.13.1.
Results
Search results
The flow chart of included studies is provided in figure 1. Five thousand four hundred and twenty unique abstracts were identified, of which 270 proceeded to full-text review. Thirteen additional relevant studies were identified through hand-searching. One hundred and eighty-six studies were excluded during full-text review, resulting in 84 articles included in the final analysis (Kappa=87.0%, 95% CI 80.8% to 93.1%).

Preferred Reporting for Systematic Reviews and Meta-Analyses flow diagram of included studies. CPOE, computerised physician order entry; LOS, length of stay; RBC, red blood cell.
Characteristics of included studies
The characteristics of included studies are summarised in online supplementary file 5. The 84 included articles comprised 83 unique study populations, as two articles29 30 reported different outcomes for the same population. In addition, one article31 reported outcomes from two unique study studies; thus, the non-overlapping findings from both studies were included. The included studies were published between 198332 and 2017,33–38 with the majority of studies conducted in the USA (n=50). Only three studies were RCTs (one cluster RCT, two randomised at the individual level)31 39 40; the remaining 81 were non-randomised studies, specifically uncontrolled before and after (n=74)29–31 33–36 38 41–106; controlled before and after (n=2)107 108; interrupted time series (n=1)37 and non-randomised trial (n=4)32 109–111 designs.
Supplementary file 5
In all cases, an intervention was compared with either historical controls or standard of care. Most studies were conducted in a single acute care facility, often an academic hospital. Follow-up periods varied considerably from 2 weeks82 to 6 years48 postintervention. Targeted populations included primarily physicians (eg, intensivists, anaesthesiologists, surgeons) ordering RBC transfusions, as well as medical trainees (eg, residents), other healthcare providers (eg, nurses) and hospital staff (eg, hospital laboratory and blood bank technologists) involved in the care of patients receiving transfusions. The unit of intervention was the individual healthcare provider, ward or unit, or institution (ie, not patients themselves).
Types of interventions
The effectiveness of either a single (n=32) or multiple interventions (n=52) in combination (referred to as multimodal interventions) was evaluated. The following single intervention categories were identified: education sessions or materials (n=9)40 80–86 109, protocols or algorithms (n=7)39 90–95, guidelines (n=4)87–89 110, computerised physician order entry (CPOE) systems and decision support (n=4)31 97–99, reminders (n=2)100 108, audit and feedback (n=2)101 111, audit approval (n=2)102 103, a clinical policy (n=1)96and prospective audit of transfusion practices (n=1).37 Descriptions of each, along with examples from the included studies, are provided in table 1.
Categories of single and multimodal behaviour modification interventions
Multimodal interventions included between 2 and 5 strategies, applied concurrently or in sequence. Combinations of multimodal interventions are summarised in online supplementary file 6. The interventions most commonly included in multimodal interventions were: education (n=38)29–36 38 41 42 47–51 53–55 57–60 62–65 67–70 72 74–77 104 105 107, guidelines (n=25)31 34 38 42 44 45 50 53–56 58 59 61 62 64 65 67 69 72 73 75 76 105 107, and audit and feedback (n=23).32 34 36 38 44 46 49 52–55 57–60 65 67–69 71–73 77 Some multimodal interventions applied additional interventions not examined among the single intervention studies, including paper order forms (n=4),61 67 71 73 financial incentives (n=1),68 and physician checklists and order sets (n=2).105 106
Supplementary file 6
Quality of included studies
All three RCTs31 39 40 incorporated study elements that were deemed to be of high, low and unclear risk of bias (online supplementary file 7). Due to the nature of the interventions, treatment allocation was not concealed, nor could the participants, personnel or outcome assessors be blinded; thus, risk of bias was consistently high in these areas. In contrast, risk of bias was low across all studies with respect to both attrition and reporting bias.
Supplementary file 7
The majority of non-randomised studies (n=63) were of moderate quality, where quality assessment scores ranged from 12 to 15; 12 studies32 42 44 47 51 52 56 81 88 92 107 109 were of low quality (scores from 0 to 11) and no studies were deemed to be of high quality (score >17) (online supplementary file 8). Most studies were found to have low scores due to poor reporting (Q1–Q10), particularly of the characteristics of the targeted population and distribution of principal confounders. External validity (Q11 and Q13) was moderate for most studies; however, Q12 (ie, subjects prepared to participate representative of the entire population) was deemed ‘unable to determine’ for all studies. The internal validity was low to moderate across studies (Q16–Q26). Adequate adjustment for confounding (Q25) and whether losses to follow-up were taken into account (Q26) were also deemed ‘unable to determine’ for all studies.
Supplementary file 8
Impact of behaviour modification interventions on RBC usage and patient outcomes
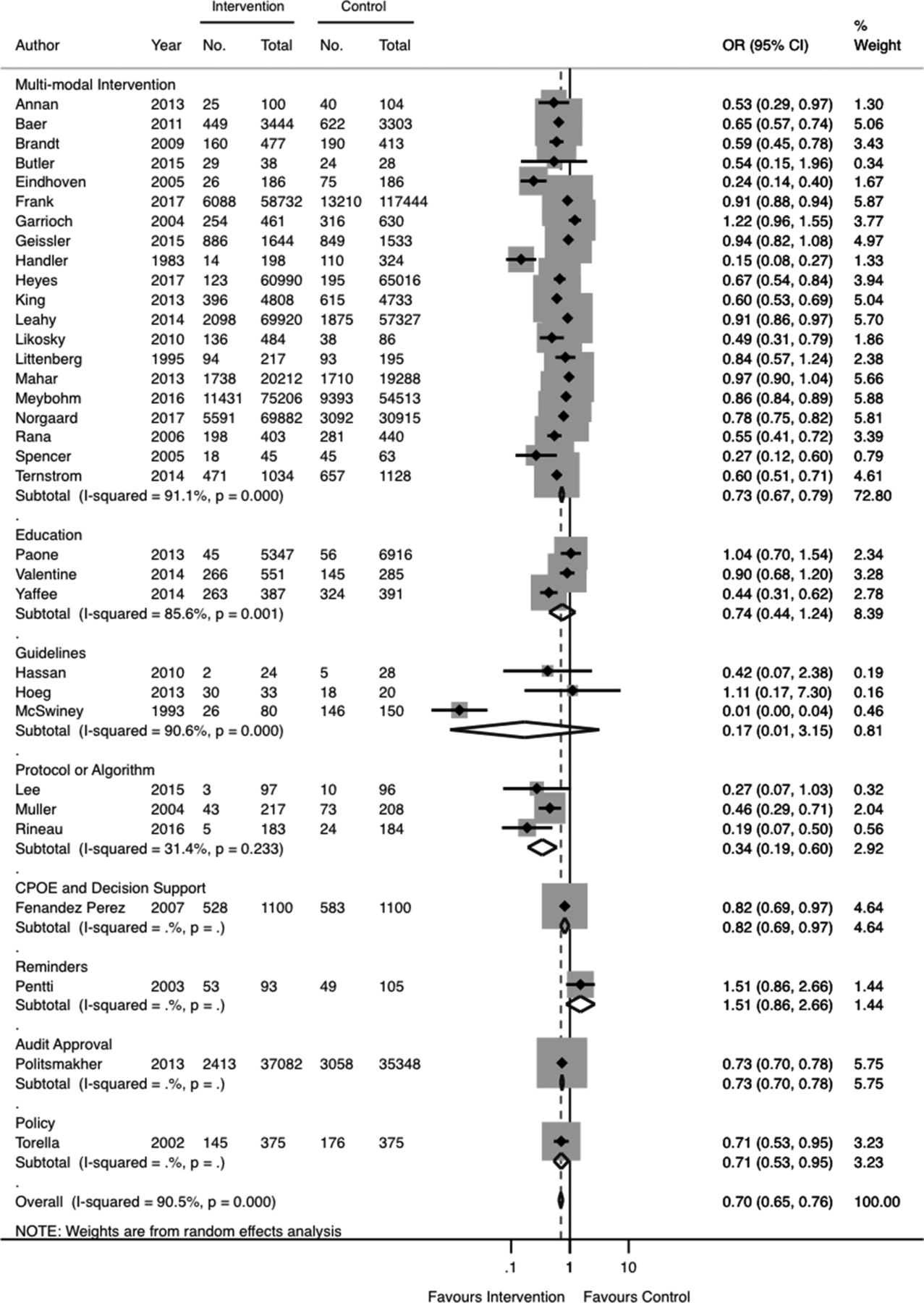
A summary of the pooled analyses is provided in table 2. The primary outcome, the proportion of patients transfused, was reported in 33 studies. The pooled odds of a patient receiving a RBC transfusion was 0.70 (95% CI 0.65 to 0.76; n=33) (figure 2; table 2). There was strong evidence of heterogeneity in this estimate (I2=90.5%, Q-statistic p=0.00), although this was not apparent on visual inspection as a number of studies crossed the null value. Sorting studies by year of publication showed that, with the exception of the two earliest studies,32 89 the associated decrease in the odds of transfusion was fairly consistent over time (online supplementary file 9).
Supplementary file 9

Forest plot of odds of patients being transfused, stratified by intervention. CPOE, computerised physician order entry.
Results of meta-analysis for RBC usage and patient outcomes
All 33 studies included in this analysis were non-randomised studies. A stratified analysis by non-randomised study design (online supplementary file 10) revealed high subgroup heterogeneity between the uncontrolled before and after studies (I2=89.6%, Q-statistic p=0.00). However, the variability between the two non-randomised trials was much lower (I2=18.7%) and was likely due to chance alone (ie, not due to heterogeneity) (Q-statistic p=0.267), suggesting that differences in study design might have contributed to some of the observed heterogeneity in the crude pooled estimate.
Supplementary file 10
Further, stratification by intervention category revealed that differences in techniques across studies might have also contributed to study heterogeneity (figure 2; table 2). Among these interventions, the use of a protocol or algorithm (pooled OR 0.34 (95% CI 0.19 to 0.60); n=3) and a multimodal intervention (pooled OR 0.73 (95% CI 0.67 to 0.79); n=20) were associated with significantly decreased odds of patients being transfused. CPOE and decision support (OR 0.82 (95% CI 0.69 to 0.9); n=1),98 audit approval (OR 0.73 (95% CI 0.70 to 0.78); n=1)103 and policy interventions (OR 0.71 (95% CI 0.53 to 0.95); n=1)96 were also associated with decreases in the odds of transfusion; these point estimates, however, were derived from a single study in each subgroup(figure 2; table 2). No significant differences were observed between groups following the use of education (pooled OR 0.74 (95% CI 0.44 to 1.24); n=3) and guidelines (pooled OR 0.17 (95% CI 0.01 to 3.15); n=3) or reminders (OR 1.51 (95% 0.86 to 2.66); n=1).
The impacts of behaviour modification interventions on secondary outcomes are summarised in table 2 and online supplementary files 11–15. An ‘inappropriate’ transfusion was defined by the included studies as a RBC transfusion initiated at a pretransfusion haemoglobin above 7–9 g/dL for most, non-bleeding adult patients.55 57 59 70 76 77 89 90 100–102 Use of an intervention was associated with a decrease in the pooled odds of inappropriate transfusion (pooled OR 0.46 (95% CI 0.36 to 0.59; I2=97.6%, Q-statistic p=0.00; n=11). The mean RBC units transfused per patient (WMD: −0.35 units (95% CI −0.38 to −0.32); I2=99.9%, Q-statistic p=0.00; n=14) and mean patient LOS (WMD: −0.63 days (95% CI −1.02 to −0.24); I2=79.7%, Q-statistic p=0.00; n=9) also decreased following the use of an intervention (table 2). The change in mean pretransfusion haemoglobin level was only examined among studies of multimodal interventions and was associated with a WMD of −0.28 g/dL (95% CI −0.48 to −0.08; I2=95.5%, Q-statistic p=0.00; n=5).
There was also significant heterogeneity in the pooled analyses of secondary outcomes (I2 ranging from 57.4% to 99.9%). It was unclear whether differences in interventions contributed to the heterogeneity, as stratification by intervention category left many subgroups with only one study; this precluded calculation of all subgroup I2 values (online supplementary files 11–15). Single modality interventions were associated with greater impacts on RBC usage, compared with multimodality interventions (table 2). Specifically, implementation of a guideline in one study resulted in the lowest odds of inappropriate transfusion (OR 0.07 (95% CI 0.02 to 0.19) and the greatest decrease in mean RBC units transfused (WMD: −1.42 units (95% CI −1.67 to −1.17)).89 Another study examining a treatment algorithm reported the largest decrease in hospital LOS, however, there was marked variability in this estimate (WMD: −6.30 days (95% CI−14.43 to 1.83)).39 A significant increase in the odds of inappropriate transfusion (OR 1.74 (95% CI 1.39 to 2.19)) was observed following audit and feedback in one study.101
There was no significant difference in the odds of in-hospital mortality (pooled OR 0.92 (95% CI 0.84 to 1.02; I2=64.8%, Q-statistic p=0.00; n=19) (table 2). The stratified meta-analysis (by intervention type) suggested that the observed heterogeneity in the pooled estimate was likely attributed to the variability in interventions examined across studies (online supplementary file 15).
Supplementary file 15
Potential predictors of RBC usage
Studies published on or after 1995, the year in which evidence of efficacy and safety of restrictive transfusion practices were first published,112 were included in the meta-regression. The year of publication, number of interventions, having a multimodal intervention, a single unit or clinical service setting, follow-up greater than 1 year, and the individual component interventions in a given study were not identified as significant predictors of RBC transfusion (online supplementary file 16).
Supplementary file 16
Publication bias
Evidence for publication bias among included studies (open circle symbols) was indicated by the asymmetry in the funnel plot (figure 3) and Egger’s regression test (p=0.001). Ten studies were imputed using the trim-and-fill method (square with circle symbols) resulting in a pooled OR of 0.803 (95% CI 0.663 to 0.972) for the primary outcome of patients being transfused. This suggests that studies of smaller patient sample size, reporting an increased likelihood of transfusion postintervention, may have been suppressed from publication.

{kind=link}
{kind=link}
{kind=link}
Filled funnel plot with pseudo 95% CIs. The open circles represent the included studies and the squares with circles represent the imputed studies. The horizontal line represents the estimated measure of effect following the trim-and-fill method and the diagonal lines forming the triangle region represent the pseudo 95% CIs.
Discussion
Efforts to modify transfusion practices are not novel and have been described internationally for over four decades. We identified 84 studies, primarily non-randomised studies of low to moderate quality, examining the impact of a behaviour modification intervention, compared with no intervention, on RBC transfusion practices. Among single modality interventions examined, nine categories were identified: education, protocol/algorithm, guidelines, CPOE and decision support, reminders, audit and feedback, audit approval, clinical policy, and prospective audit of transfusion practices. The majority of studies used multimodal interventions. Meta-analysis was permitted for a small subset of only non-randomised studies (n=33). On average, the pooled odds of patients being transfused decreased by 30% (pooled OR 0.70; 95% CI 0.65 to 0.76) and patients received 0.35 fewer RBC units postintervention. In addition, the pooled average pretransfusion haemoglobin levels decreased by 0.28 g/dL and the proportion of inappropriate transfusion (above a haemoglobin of 7–9 g/dL) decreased by approximately 54% (pooled OR 0.46; 95% CI 0.36 to 0.59). As expected, given the increasing body of evidence suggesting similar safety profiles between restrictive and liberal transfusion practices,13 there was no difference in the pooled odds of in-hospital mortality between intervention and comparator groups. Among all interventions examined, the protocol/algorithm and multimodal interventions were associated with the greatest decreases in the pooled odds of patients being transfused.
The present study represents the most up-to-date collection of published literature and the first meta-analysis of interventional studies in this field. Therefore, the analytical investigations performed in our study represent a substantial and novel contribution to the existing knowledge of how to achieve restricted RBC transfusion practices. Across all pooled estimates, we observed significant statistical heterogeneity, which was only partly attributed to the variability between interventions. Context-specific factors, not easily discernable from the available evidence, are also likely contributing to the observed heterogeneity among included studies. These may include variability in physician experience, clinical practice or flow, perceived ease of an intervention, and/or organisational capacity or receptivity for change.113 Work from the audit and feedback literature—which is among the most extensive in the area of behaviour modification interventions—also report variability in effect size of the intervention based on differences in baseline performance of the targeted behaviour, as well as nuances in delivery of the intervention (ie, how feedback is provided).114 Collectively, this information suggests that the decision to adopt a given intervention should, therefore, consider evidence of effectiveness and the factors related to the context and implementation. For instance, a labour-intensive intervention, such as a CPOE and decision support system, will be more feasible and efficient to implement in a setting with electronic ordering systems already in place, rather than in a one without. Explicit methodology to first identify relevant determinants to change and selection of an intervention(s) to address such determinants, such as through theory-based frameworks, might prove useful in tailoring an appropriate intervention to a given clinical setting.115 116
Our findings are consistent with the evidence from the broader knowledge translation literature.117 In one of the most comprehensive systematic reviews, Grimshaw et al 117 identified over 200 studies examining the impact of interventions on a wide range of healthcare provider behaviours and settings. The authors identified a similar array of interventions (eg, education, audit and feedback, reminders) that were all were effective to varying degrees, and their observed effectiveness was not associated with the number of interventions implemented within a given study.117 The results of our meta-regression analysis further support that a multimodal intervention and the number of component interventions are not predictive of the impact of the interventions on the primary outcome.
Our results are also in line with the qualitative findings of previous systematic reviews of interventions to modify transfusion practices more broadly.16–18 Identified interventions were similarly found to be effective at reducing transfusion use, however, the previous reviews were unable to comment on their comparative effectiveness due to the dearth of direct comparisons between intervention types and reported heterogeneity among studies.16 17 With our updated review of the literature, meta-analysis was feasible given the high prevalence of common study designs, as well as frequent reporting of our primary and secondary outcomes. While the comparator groups among included studies were also restricted to historical controls or standard of care, our stratified meta-analyses still enabled crude comparisons of effectiveness between interventions.
Limitations
The majority of included studies were non-randomised studies of low to moderate quality and susceptible to bias. For example, most studies employed an uncontrolled before and after study design and, in the absence of a concomitant control group, these studies were at high risk of bias due to both secular trends and maturation bias.118 Due to the lack of randomisation, such studies can also be susceptible to selection bias.23 In addition, we found limited to no reporting of participant characteristics and it is unclear whether and to what extent these characteristics led to confounding of the reported outcomes. The non-randomised studies were deemed to have moderate external validity, thus, generalisability of findings across all clinical settings and/or international healthcare systems is unclear.
Despite the large number of studies included in the systematic review, the primary outcome was only available for a minority of non-randomised studies (n=33). Our stratified meta-analysis resulted in a very limited number of studies (or even one study) often of moderate quality, in many of the single modality subgroups. Taken together, these limited our ability to make inferences of comparative effectiveness across all intervention types and precluded our ability to perform further statistical techniques, such as network meta-analysis.119 While meta-regression was permitted for the primary outcome, similar analyses were underpowered for most secondary outcomes.120 Finally, the findings from our meta-analyses must be interpreted with caution given the evidence for publication bias. Previous reviews similarly suggested of publication bias among earlier included studies due to the tendency of outcomes to favour the intervention group.16 17
Given such limitations of the non-randomised studies (particularly the uncontrolled before and after studies) and the meta-analytical efforts, it is difficult to state with certainty which intervention is the most effective at modifying RBC transfusion practice.
Future research
Further comparative effectiveness studies designed as large, high-quality RCTs are recommended to determine the effectiveness of the present interventions. However, the prevalence of low to moderate quality non-randomised studies included in this present review may indicate the logistical difficulty in evaluating these interventions through RCTs. As such, pragmatic trial designs may be considered to aid in balancing issues of feasibility with methodological rigour.121 Also, none of the included studies evaluated the effectiveness of a behaviour modification intervention to that of another behaviour modification intervention (of either single or multimodality). Such direct comparisons would aid in confirming effectiveness of interventions and help determine the comparative effectiveness of interventions. In the case of multimodal interventions, further research should also attempt to address which elements of the intervention are key to affecting the desired change. This information may better and more appropriately advise healthcare organisations seeking to implement the most effective behaviour modification intervention.
Lastly, we did not identify any studies that performed a concomitant economic evaluation. This information is critical to selecting an intervention that is also efficient within a given healthcare budget. Sixteen of the included studies did report of changes in healthcare costs, primarily cost savings in RBC usage, following either a single or multimodal intervention.30 34–37 45 57 61 72 75 80 86 90 98 103 104 Only two studies factored in the cost of implementing the intervention into their estimate.34 98 Given the often costly, labour-intensive nature of many interventions, future cost-effectiveness studies should include the cost of implementation to determine whether true savings are realised from a given intervention.
Conclusions
We found a large body of literature evaluating the impact of behaviour modification interventions on RBC transfusion practices. The types of interventions are diverse, including single and multimodality interventions. The quality of included studies was low to moderate and the proportion of non-randomised studies was high (n=81). The protocol or algorithm and multimodal interventions were associated with statistically significant reductions in the pooled odds of RBC transfusion. These results must be interpreted with caution due to the prevalence of uncontrolled before and after studies, statistical heterogeneity, limited study sample size within intervention groups and evidence for publication bias. Given these limitations, further large, high-quality pragmatic trials would aid to confirm and directly compare effectiveness and cost-effectiveness of different types of behaviour modification interventions. This shift in the field from simply understanding ‘does it work’, towards investigating ‘what works best’ and ‘at what cost’ is required as healthcare organisations respond to meet the transfusion guideline recommendations.
Supplementary file 11
Supplementary file 12
Supplementary file 13
Supplementary file 14
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
Footnotes
Contributors Design of the study (LJJS, TWN, DLL and FMC); management of data (LJJS, FMC); analysis of data (LJJS, LED, KM, HMH and FMC); interpretation of the data (LJJS, TWN, HTS, DAZ and FMC); preparation of manuscript (LJJS, FMC); review of manuscript (LJJS, TWN, LED, KM, HMH, DLL, HTS, DAZ and FMC); approval of manuscript (LJJS, TWN, LED, KM, HMH, DLL, HTS, DAZ and FMC).
Funding LJJS is supported by an Alberta Innovates-Health Solutions (AIHS) Graduate Studentship Award (Record Number: 201500076).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data generated or analysed during this study are included in this published article, its supplementary information files and the included reference articles (listed under Reference List).