Article Text

Abstract
Objectives There is limited published research studying the effect of antibiotic prophylaxis on surgical site infection (SSI) in dermatological surgery, and there is no consensus for its use in higher-risk cases. The objective of this study was to determine the effectiveness of a single oral preoperative 2 g dose of cephalexin in preventing SSI following flap and graft dermatological closures on the nose and ear.
Design Prospective double-blinded, randomised, placebo-controlled trial testing for difference in infection rates.
Setting Primary care skin cancer clinics in North Queensland, Australia, were randomised to 2 g oral cephalexin or placebo 40–60 min prior to skin incision.
Participants 154 consecutive eligible patients booked for flap or graft closure following skin cancer excision on the ear and nose.
Intervention 2 g dose of cephalexin administered 40–60 min prior to surgery.
Results Overall 8/69 (11.6%) controls and 1/73 (1.4%) in the intervention group developed SSI (p=0.015; absolute SSI reduction 10.2%; number needed to treat (NNT) for benefit 9.8, 95% CI 5.5 to 45.5). In males, 7/44 controls and 0/33 in the intervention group developed SSI (p=0.018; absolute SSI reduction 15.9%; NNT for benefit 6.3, 95% CI 3.8 to 19.2). SSI was much lower in female controls (1/25) and antibiotic prophylaxis did not further reduce this (p=1.0). There was no difference between the study groups in adverse symptoms attributable to high-dose antibiotic administration (p=0.871).
Conclusion A single oral 2 g dose of cephalexin given before complex skin closure on the nose and ear reduced SSI.
Trial registration number ANZCTR 365115; Post-results.
- antibiotic prophylaxis
- surgical site infection
- dermatologic surgical wound infection
- operative surgical procedures
- flaps
- grafts
- ear
- nose
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- antibiotic prophylaxis
- surgical site infection
- dermatologic surgical wound infection
- operative surgical procedures
- flaps
- grafts
- ear
- nose
Strengths and limitations of this study
Blinded randomised design with placebo control.
Standardised protocols used for excision and follow-up.
Low baseline infection rate in women meant underpowered to draw conclusions for this subgroup.
Introduction
Though limited published evidence is available to support or refute the use of oral antibiotic prophylaxis for prevention of surgical site infection (SSI) in dermatological surgery, several authorities suggest considering it for selected high-risk cases.1–4
As the ears and noses are especially vulnerable to ultraviolet (UV) radiation, generally being uncovered and protruding from the body, skin cancers are more commonly found at these sites than most other body sites.5 Furthermore, the cancers that develop on the nose and ear are more likely to be of an aggressive subtype6 requiring wider excision margins and subsequent flap or graft surgical repair for optimal cosmetic and functional outcome. The body site and the need for complex closure put patients with auricular or nasal skin cancers at significantly higher risk of SSI than is normally observed for clean dermatological surgery.1–4
Despite the paucity of evidence for dermatological antibiotic prophylaxis, first-generation cephalosporins or penicillinase-resistant penicillins are generally recommended as Staphylococcus aureus and Streptococci are the most prevalent bacteria causing SSI.1 2 Oral cephalexin or dicloxacillin given as a 2 g oral dose 30–60 min before the procedure has been recommended by several authorities.1 2 7
The aim of this study was to determine whether the use of a single 2 g dose of cephalexin given 40–60 min prior to surgery would significantly reduce infection rates following complex auricular and nasal dermatological surgery.
Method
Consecutive eligible patients booked for flap or graft closure following skin cancer excision on the ear and nose were recruited by six doctors (including the principal researcher HR) working at a primary care skin cancer clinic in Townsville, North Queensland, Australia, between December 2013 and March 2016. Study participation was allowed once only for each individual patient. All participants2 gave signed informed consent.
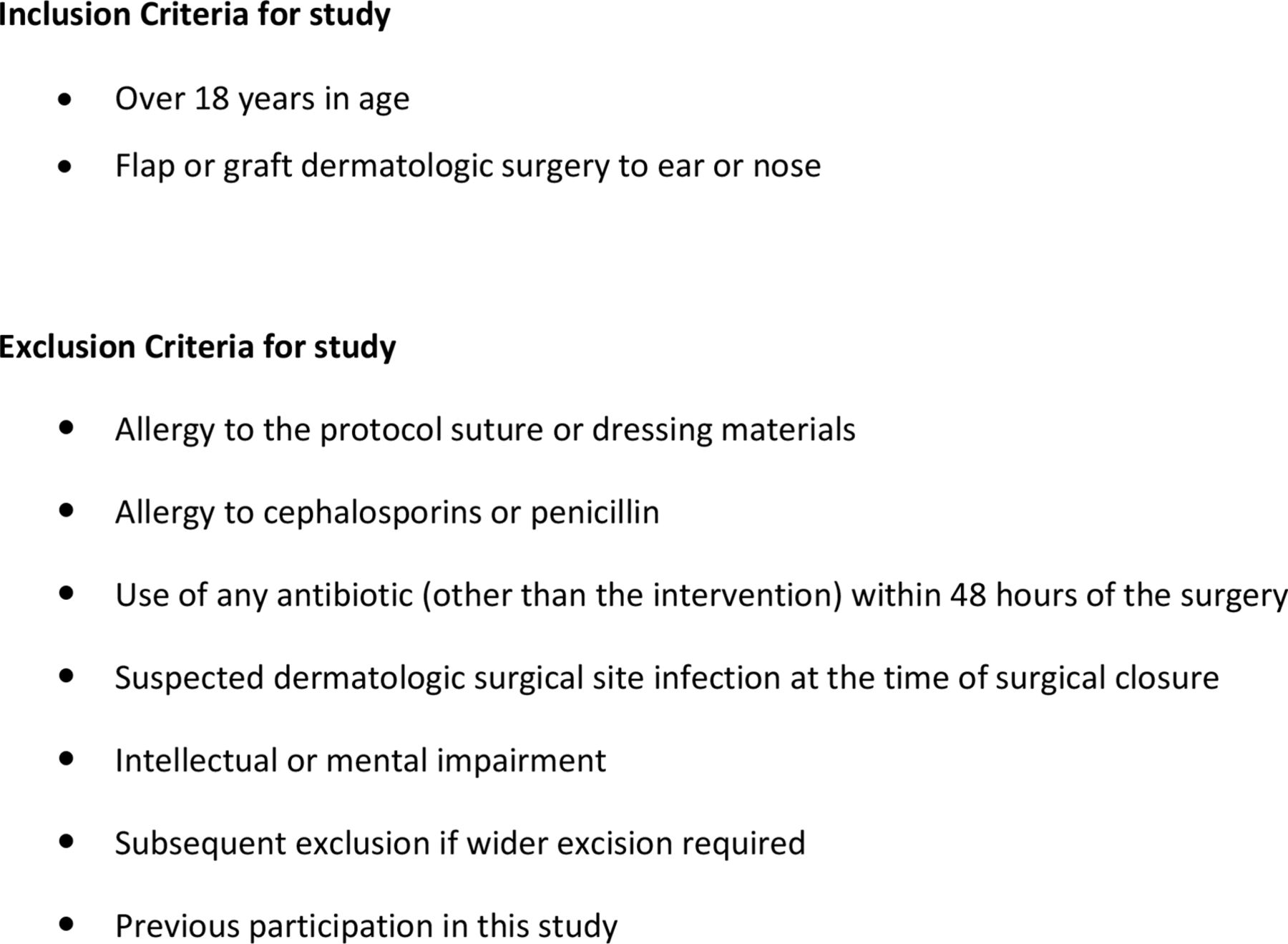
Specific exclusion criteria (figure 1) were aged under 18, intellectual or mental impairment affecting ability to give informed consent, allergy to the protocol suture or dressing materials, allergy to cephalosporins or penicillin, use of any antibiotic (other than the intervention) within 48 hours of the surgery and suspected SSI at the time of surgical closure. If pathology confirmed residual tumour and the need for a wider excision the participant was subsequently excluded from the study.

Inclusion and exclusion criteria.
All participants presented 30 min prior to their surgery for administration of capsules containing either 2 g cephalexin or a placebo. The initial skin incision was made 40–60 min after ingestion of capsules. Cephalexin was used because it has an antistaphylococcal activity and therefore covers organisms most likely to cause wound infection, but can be used in most patients with penicillin allergy and is cheaper than flucloxacillin.2 Pharmacokinetic data show average peak dose serum levels of approximately 19 µg/mL at 1 hour following a 500 mg dose.8 A 2 g dose has been used effectively in previous studies.8 Baseline demographic data, relevant medical and drug history, histology, defect size, time from intervention to surgery and closure technique were documented at the time of surgery.
Modified Mohs micrographic surgery
We used an adaptation of classical Mohs micrographic surgery (MMS) for patients with biopsy-proven aggressive tumours that had indistinct margins or were 10 mm or larger. The wound was left open under a dressing for 2 days awaiting complete histological deep and peripheral margin analysis using traditional H&E staining of wax-embedded samples in a pathology laboratory. Further excision and detailed histological analysis was undertaken if required with the wound only being closed once histology confirmed complete excision. It is known that SSI following secondary intention healing is very low,9 10 hence antibiotic or placebo was only given prior to the actual flap or graft wound closure.
Intraoperative and postoperative protocol
Nylon sutures (Dynek, Hendon, South Australia) were used superficially for all defect closures. Where deep dermal absorbable sutures were deemed necessary, Monosyn (B Braun Australia) was used. Melolin (Smith and Nephew Medical, Hull, UK) and Fixomull (BSN Medical Luxembourg) were applied to wounds immediately after surgery. Participants were asked not to use topical creams, ointments or antiseptics on their wounds postoperatively and were given standardised written and verbal instructions on postoperative wound care. Early wound review was encouraged in the event of any participant concern. Sutures were removed 5–7 days postoperatively. Any wound that had not fully healed was redressed until the defect had fully epithelialised.
Clinical outcome
Though there is no validated gold-standard definition for SSI, the 1988 Centers of Disease Control and Prevention of National Nosocomial Infections Surveillance System definition11 has been widely adopted in Australia, USA and Europe. We used an adapted version of this definition (figure 2). The superficial surgical site skin infection had to occur within 30 days of surgery and at least one of the following wound characteristics had to be present:
purulent discharge
localised swelling, pain or heat
erythema >1 cm from wound edges
patient report of increasing tenderness.

Criteria for surgical site infection.
Using this classification, if SSI was suspected by the treating doctor a swab was taken for microbiology culture and sensitivity and a 5-day course of cephalexin (500 mg four times per day) prescribed pending swab results.
The study nurse phoned participants 1 month postoperatively to cross-check if Dermatological Surgical Site Infection (DSSI) or any other complication had occurred helping to ensure that this had not been inadvertently missed.
Randomisation and blinding
The randomisation sequence, generated off-site electronically by author and statistician PGB, was sent to a compounding pharmacy in Townsville. Here batches of generic gel capsules were filled with either cephalexin (intervention) or microcrystalline cellulose and calcium carbonate (placebo) and sent to the recruiting practice in small screw top containers numbered according to the randomisation sequence. Each numbered container held four identical-looking gel capsules filled with either 500 mg cephalexin or placebo. Staff and participants at the recruiting clinic remained blinded to group allocation until the study had been completed.
Sample size
The infection rate for complex auricular and nasal dermatological surgery in a small observational survey at out clinic prior to commencing this study was around 20%. Our hypothesis was that antibiotic prophylaxis would reduce SSI fivefold from 20% to 4%. To show this with statistical confidence (power in excess of 80%; significance level 0.05), 59 patients were required in each study group. Allowing for a 20% drop-out it was planned to recruit 142 participants (71 intervention and 71 placebo).
Statistical analysis and presentation
Numerical data were described using mean and SD when symmetrically distributed and median and IQR when skewed. Categorical data were presented using absolute and relative frequencies.
Eligible non-participants were compared with participants using unpaired t-test, χ2 and Fisher’s exact test. Intervention and control group differences at baseline as well as treatment modality differences were assessed using unpaired t-test, Mann-Whitney U test, χ2 and Fisher’s exact test.
The main analysis comparing intervention and control groups with regards to SSI was modified by intention-to-treat (ITT) analysis based on available cases at follow-up and adhered to Consolidated Standards of Reporting Trials (CONSORT) guidelines.12 Furthermore, ITT analysis was conducted assuming that: (1) none of the lost to follow-up cases had developed SSI and (2) all lost to follow-up cases had developed SSI.
Incidence of wound infection was compared between intervention and control groups using Fisher’s exact test. The differences in infection rates and number needed to treat for benefit (NNTB) were calculated with 95% CIs.13
χ2 test and Fisher’s exact test were used to compare postoperative complications, adverse effects and treatment of established postoperative infections between intervention and control groups.
Analysis was conducted using SPSS V.21 (IBM SPSS). A significance level of 0.05 was assumed. All statistical tests were conducted two sided.
Results
Of 199 consecutive patients requiring flap or graft closures on the nose or ear, 20 were ineligible due to penicillin or cephalosporin allergy (11), intellectual impairment (4) or taking antibiotics for other reasons within 48 hours of their skin surgery (5). See figure 3 for CONSORT flow diagram.

{kind=link}
{kind=link}
{kind=link}
Consolidated Standards of Reporting Trials flow chart references.
Twenty-five eligible patients opted not to participate most commonly as they were unwilling to take unnecessary medication (14). Other reasons for non-participation (11) included fear of diarrhoea or allergy, difficulty swallowing tablets and not having time to come in 30 min ahead of the scheduled appointment.
Inadvertently, 12 more participants were recruited than planned resulting in a total of 154 participants. The participants were slightly older (mean age 66.3 years) and more likely to be female (71, 46.1%) than the 25 eligible non-participants (mean age 63.2 years; 8 female). Otherwise no difference was found between participants and non-participants (table 1).
Comparison of participants with non-participants who fulfilled inclusion criteria
Four participants violated protocol because of the need for a wider excision (1) or the doctor or patient changing their mind about having flap or graft surgery after the antibiotic or placebo had been given (3). Due to death from unrelated causes during the postoperative study period (1) or failure to respond to repeated telephone follow-up (7) eight participants were lost to follow-up. These 12 participants who did not complete the study as intended (table 2) were more likely to be smokers (3) or study controls (8) than participants who did complete the study.
Comparison analyses of participants who completed the study to those who did not complete the study
Table 3 shows that the randomisation was mostly successful creating comparable groups at baseline. However, there were more male patients in the control group (63.8% vs 45.2%).
Baseline comparison of intervention group (n=73) with control group (n=69)
Surgical site infection
The main analysis based on available cases at follow-up (table 4) showed that one (1.4%; n=73) SSI occurred in the intervention group compared with eight (11.6%; n=69) in the control group (p=0.015).
SSI analysis of available cases, stratified by sex
The difference in incidence of infection was 10.2% (95% CI 2.2% to 18.2%). The NNTB was 9.8 (95% CI 5.5 to 45.5). These results were confirmed by the ITT analyses (table 5) assuming both that (1) none of the 12 cases lost to follow-up had developed SSI (p=0.034) and (2) all 12 cases had developed SSI (p=0.017).
SSI analysis by ‘ITT’ assuming (1) all and (2) none of the participants violating protocol or lost to follow-up would have developed SSI
SSI-stratified analysis by sex
Giving cephalexin prior to surgery significantly reduced SSI in men (table 4) with 7 of the 44 controls and none of the 33 intervention participants developing infection (p=0.018). Antibiotic prophylaxis resulted in an absolute SSI reduction of 15.9% (95% CI 5.2% to 26.6%) and a relative SSI reduction of 100% in men. In order to prevent one infection in male participants, 6.3 men need to be treated (95% CI 3.8 to 19.2).
Antibiotic prophylaxis made no difference to the low rate of SSI in women with one control (n=25) and one intervention participant (n=40) developing infection (p=1.0).
Regardless of group allocation, none of the participants who had modified MMS (delayed closure following complete histological margin analysis) developed SSI.
Swab results for SSI cases
For the nine participants who developed SSI (table 6), eight had swabs taken for microscopy, culture and sensitivity.
Details of participants that developed SSI
Cephalexin-sensitive S. aureus was confirmed in six participants. In one participant cephalexin-resistant Hafnia alvei infection was confirmed; the infection had already responded clinically to prescribed cephalexin by the time the microbiology report was available. Pseudomonas aeruginosa was confirmed in a control participant following an ear wound repair; this settled quickly once antibiotics were changed to the quinolone ciprofloxacin in accordance with culture sensitivity. The final participant with SSI inadvertently attended his general practitioner who prescribed flucloxacillin without taking a swab for culture and sensitivity. At the time of suture removal at the study practice, review of a photograph taken by the participant before antibiotics had been prescribed confirmed SSI clinically.
Secondary outcome measures
With respect to postoperative complications other than infection (table 7), there was no difference between the study groups (p=0.364) with two postoperative haemorrhages (both intervention), one flap necrosis (control) and one wound dehiscence (intervention).
Comparison of study groups with respect to postoperative complications and adverse events
Furthermore, there was no significant difference between the study groups in adverse symptoms (table 7) that might have been attributable to high-dose antibiotic administration (p=0.871) with one participant from each study group suffering some nausea and mild diarrhoea being reported in one intervention participant.
Discussion
Though infection rates are generally very low for clean dermatological surgery,1–3 a significant increase in SSI is observed for surgery on the ear and nose compared with other body sites.14–16 Of all body sites the nose and ear have the greatest concentration of sebaceous glands. With the latter being heavily colonised by bacteria, the increased risk of SSI on the nose and ear may be explained. Furthermore, with the nares being a principal source of S. aureus, it is postulated that its proximity puts nasal skin incisions at higher risk of infection still.
Complex wound closures have consistently been linked with greater risk of SSI than simple closures.14 16–19 In a large prospective study involving 3491 surgical dermatological procedures, Rogues et al observed that the difference in infection rates following flap and graft closure (14.7%) rather than simple closure (1.7%) was even more marked when clean rather than sterile gloves were worn.19 For complex dermatological closures also involving the nose and ear, Sylaidis et al found a much higher infection rate (6 of 27) than they did for complex skin closures elsewhere on the face (3 of 43).14
The evidence to support or refute the use of oral antibiotic prophylaxis for dermatological surgery at higher risk of SSI is scant.3 20 21 Though overt infection was seen in none of 30 randomised controlled trial (RCT) patients undergoing full thickness graft reconstruction surgery on the nose, Kuijpers et al found the graft survival was better for those randomised to antibiotic prophylaxis (azithromycin for 3 days).22 Subanalysis of 60 reconstructive dermatological flap procedures in an RCT confirmed that antibiotic prophylaxis resulted in significantly fewer SSIs.23 In a small non-randomised observational study involving 18 patients having facial graft surgery for Non Melanotic Skin Cancer (NMSC), Saleh et al observed that antibiotic prophylaxis resulted in significantly less infection, graft loss and graft necrosis.24 Conversely, in an RCT involving 82 patients undergoing secondary intention healing following auricular Mohs surgery, Mailler-Savage et al found no difference in wound healing or SSI with antibiotic prophylaxis (levofloxacin).25
In our RCT for patients having complex cutaneous repair on the nose and ear, a significant reduction in SSI was found following antibiotic prophylaxis. Although our baseline infection rate was lower than anticipated (11.6% rather than 20%), the study was still adequately powered to assess the effect of antibiotic prophylaxis as the intervention group had more than the fivefold reduction in infection rate (to 1.4%) that had been anticipated for the purpose of sample size calculation.
Our main analysis is presented as an available case analysis. The Cochrane definition of ITT is the analysis of all randomised participants even if they have violated the protocol or been lost to follow-up. We, therefore, imputed data for the 12 participants for whom we had been unable to collect outcome data (table 5). Our results remained significant regardless of whether those violating protocol and lost to follow-up had all developed SSI or all remained free of infection.
As sex was identified as a confounder, the analysis was stratified by sex. The benefit of antibiotic prophylaxis was clear in men. Just one of the 25 female controls developed SSI. The authors consider this too low an infection risk to justify routine antibiotic prophylaxis. Furthermore, no reduction in SSI was observed in the 40 women given antibiotic prophylaxis. It needs to be acknowledged, however, that due to the low baseline infection rate in women, the study was underpowered to draw conclusions regarding the effect of antibiotic prophylaxis in this subgroup.
Rogues et al also found that gender was an independent risk factor for SSI following complex reconstructive skin surgery with 6.3% of men and 1.1% of women developing infection.19 Men are known to have higher sebum production and thicker skin than women particularly following menopause.26 The higher concentration of pilosebaceous units on the thicker glabrous skin of the ear and nose in men may mean an increased bacterial skin commensal load at these sites explaining the marked gender difference in SSI found in our study.
With no difference between the study groups in adverse symptoms that might have been attributable to the administration of a single high-antibiotic dose, our study confirms that 2 g oral cephalexin is well tolerated. Other studies have confirmed that higher-dose short-term antibiotics have no increased side effects compared with lower dose longer-term antibiotic courses.27
Though higher infection rates have been observed following MMS on the nose than other body sites,16 studies confirm that SSI is generally low following MMS.2 28 29 The modified MMS we used, leaving wounds open under a dressing for up to 48-hour awaiting histology, was not associated with any increase in SSI compared with wounds closed immediately following excision.
Conclusion
With indiscriminate use of antibiotics causing the emergence of ever more antibiotic-resistant pathogens, antibiotics should always be prescribed with caution. Where antibiotic prophylaxis has been shown to be both warranted and effective its use preoperatively may be justified. Furthermore, antibiotic resistance may be less likely following a single high-antibiotic prophylactic dose than following prolonged antibiotic treatment of an established infection.
In our study, an unacceptably high rate of SSI was observed following complex auricular and nasal dermatological repair. A single high-dose preoperative oral antibiotic significantly reduced SSI. The effect was significant in men but not women. Additionally, a bolus oral dose of 2 g cephalexin dose was well tolerated with no measurable increase in adverse effects compared with placebo.
Acknowledgments
The authors would like to express their sincere thanks to trial recruiting doctors (Drs Alan Poggio, Jeremy Hudson, Robert Teunisse, Lauren Barcley, Sandra Steele, Michael Khong and Abid Vitani), the trial clinical nurse (Lyndie Terry) and data collection personnel (Lorraine Fisher, Lynne Kelly and Angela Byers).
References
Footnotes
Contributors HR established and oversaw the study design and implementation and compiled the data. CFH assisted with study design and analysis. PGB led the sample size calculation and study analysis. All authors contributed to the manuscript production.
Funding The Skin Cancer College of Australasia has provided funding to cover pharmaceutical costs associated with filling generic capsules with either active antibiotic or inert powder (placebo).
Disclaimer The funding body has not been involved in any way in the study design, data collection, data analysis, writing of the paper or making decisions regarding its publication.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This randomised double-blinded placebo controlled trial was approved by the Human Research Ethics Committee of the Townsville Hospital and Health Service (approval number HREC/13/QTHS/61, May 2013) and registered with the Australian New Zealand Clinical Trial Registry (ACTRN12613001253796).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data sharing can be discussed with the corresponding author.