Article Text

Abstract
Objectives To categorically describe cancer research funding in the UK by gender of primary investigator (PIs).
Design Systematic analysis of all open-access data.
Methods Data about public and philanthropic cancer research funding awarded to UK institutions between 2000 and 2013 were obtained from several sources. Fold differences were used to compare total investment, award number, mean and median award value between male and female PIs. Mann-Whitney U tests were performed to determine statistically significant associations between PI gender and median grant value.
Results Of the studies included in our analysis, 2890 (69%) grants with a total value of £1.82 billion (78%) were awarded to male PIs compared with 1296 (31%) grants with a total value of £512 million (22%) awarded to female PIs. Male PIs received 1.3 times the median award value of their female counterparts (P<0.001). These apparent absolute and relative differences largely persisted regardless of subanalyses.
Conclusions We demonstrate substantial differences in cancer research investment awarded by gender. Female PIs clearly and consistently receive less funding than their male counterparts in terms of total investment, the number of funded awards, mean funding awarded and median funding awarded.
- Funding
- Gender
- Research Investment
- Global Health
- Research And Development
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first study to present detailed quantifiable differences in cancer research funding between male and female primary investigators in the UK.
Our study is dependent on the accuracy of original investment data from the funding bodies.
We could not openly access data of private sector research funding, nor were we able to obtain disaggregated data from Cancer Research UK.
While the gender discrepancies in cancer research funding observed in our study period are likely multifactorial, this study does not allow us to postulate any potential underlying mechanisms responsible for these observations.
Introduction
Within the European Union (EU), women represent nearly half of the workforce and more than half of all university graduates; however, they are under-represented in senior positions in the workplace.1 In science, research and development, the attrition rate among women exceeds that of their male counterparts at every stage of career progression in a phenomenon termed the ‘leaky pipeline’, with women representing 46% of PhD graduates, 33% of career scientists and 22% of grade A researchers (the highest posts at which research is conducted—equivalent to professorships in the UK).2 In the field of medical science, women represent 17.8% of grade A researchers.2 This problem is not limited to the EU, and several studies have similarly explored the gender imbalance in the USA.3–5 Indeed data collected by Unesco suggest that just one in five countries worldwide has achieved gender parity in scientific research (defined as when 45% to 55% of researchers are women).6 Previous studies have proposed a number of factors that may contribute towards this observed ‘leaky pipeline’ including societally defined traditional gender roles, attitudes towards career deviation and career breaks, lack of mentorship, institutional discrimination and sexual harassment.7
This problem is an ongoing concern both to policy-makers and to the science community at large, particularly within the science, technology, engineering, maths and medicine (STEMM) fields.8 A number of initiatives have sought to highlight and promote change in order to address this issue. Gender equality is a central component of Horizon 2020, a flagship initiative to secure Europe’s global competitiveness.9 Whereas previous campaigns10 11 have had unclear impact and in some instances been described as offensive to gender equality,12 this will be one of the first efforts to be legally enshrine gender equality into research and innovation.9 Three central objectives of Horizon 2020 include fostering gender balance in research teams, ensuring gender balance in decision-making panels and groups as well as integrating gender analysis in research and innovation content.
With regard to science research funding, men receive a 4.4% higher funding application success rate compared with women in the EU (31.8% success rate for men, 27.4% success rate for women).13 Previous research has shown that in general, it is harder for women to obtain high prestige awards and that female applicants have proportionately more success when applying for smaller grants.14
In the biomedical sciences, women receive smaller grants compared with their male counterparts both in the USA15 and the UK.16 Women are noticeably under-represented in UK clinical oncology research17 and gender discrepancies exist in the success rates of grant applications to UK funders.18 Subconscious bias has been demonstrated in the decision-making of academic science recruiters19 and also reported by those who assess grant applications.18 Although gender discrepancies do appear to vary across specific fields of research, it has been previously reported that women do not appear overtly disadvantaged in social science research.20
Our group has previously undertaken a systematic comparison of infectious disease research funding by gender within the UK, showing clear and consistent differences between the genders in total funding and median award size, across a range of diseases and types of science.21 Here we examine the distribution of cancer research funding awarded to men and women primary investigators (PIs) across specific cancers, funder categories and along the research and development (R&D) continuum.
Materials and methods
Our methods build on those developed for previous analyses of infectious disease research investments, which are described in detail elsewhere,22–24 and adapted in subsequent peer-reviewed publications (www.researchinvestments.org/publications).
We systematically examined funding awards from a number of public and philanthropic cancer research funding bodies (including the Medical Research Council, Department of Health, Biotechnology and Biological Sciences Research Council, Engineering and Physical Science Research Council, Wellcome Trust, European Commission, as well as nine members of the Association of Medical Research Charities) between 2000 and 2013. Information was obtained by downloading openly accessible information on the funder website, contacting the funder to request information or searching existing funding databases. For each award, the title and abstract, where available, were individually screened for relevance to cancer research. We excluded awards that were (1) not obviously or immediately relevant to oncology; (2) led by a non-UK institution; (3) not considered to be for R&D activity. Studies that were completed without funding were also excluded. Private sector data were not available to evaluate at the same level of detail as public and philanthropic research award data and were therefore excluded from this analysis. Cancer Research UK (CRUK) would not provide their funding data at individual award level and so could not be included in the main analysis.
We assigned each study to one of 16 primary cancer site categories and also as many of 14 cross-cutting categories as appropriate. To reduce the impact of skew due to small sample size, we restricted our cancer site analysis to those site-specific cancers with at least 15 studies across both sexes. As a result, testicular (14 studies), bone (13 studies), bladder (10 studies), thyroid (4 studies) and cholangiocarcinoma (2 studies) were excluded from our site-specific cancer analysis.
The 14 cross-cutting categories were paediatric, geriatric, infection-associated, women’s health, men’s health, occupational health, pathogenesis, diagnostic/screening/monitoring, drug therapy, radiotherapy, surgery, immunology, psychosocial and global health. The ’other' category was only used when none of the aforementioned categories were deemed to be appropriate. We allocated studies to one of five categories along the R&D continuum: preclinical; phase I, II or III clinical trials; product development (including phase IV activity); public health; and cross-disciplinary research. Cross-disciplinary awards were defined as studies that clearly considered research across two or more different types of science (eg, preclinical science leading into a phase I trial).
Where the PI was named as the recipient of an award, the PIs were categorised as male or female. Where there was any uncertainty as to gender there was further scrutiny via review of the literature, institutional websites or publicly available publications and documents. Where we were finally unable to identify a PI’s gender, the study was assigned as ‘unclear’. Where the recipient PI of an award was not identified, the study was assigned as ‘unspecified’.
Where awards were described in currencies other than UK pounds, these were converted to UK pounds using the mean exchange rate in the year of the award. All included awards were adjusted for inflation and reported in 2013 UK pounds.
We report descriptive statistics including median, IQR and percentages for categorical variables. Data were graphically inspected for normality using histograms. Mann-Whitney U tests were performed to test for univariate associations between gender and funding. Data were collated in Microsoft Excel 2010 and statistical analysis was performed using R studio (V.0.99.903) and Stata (V.13).
Results
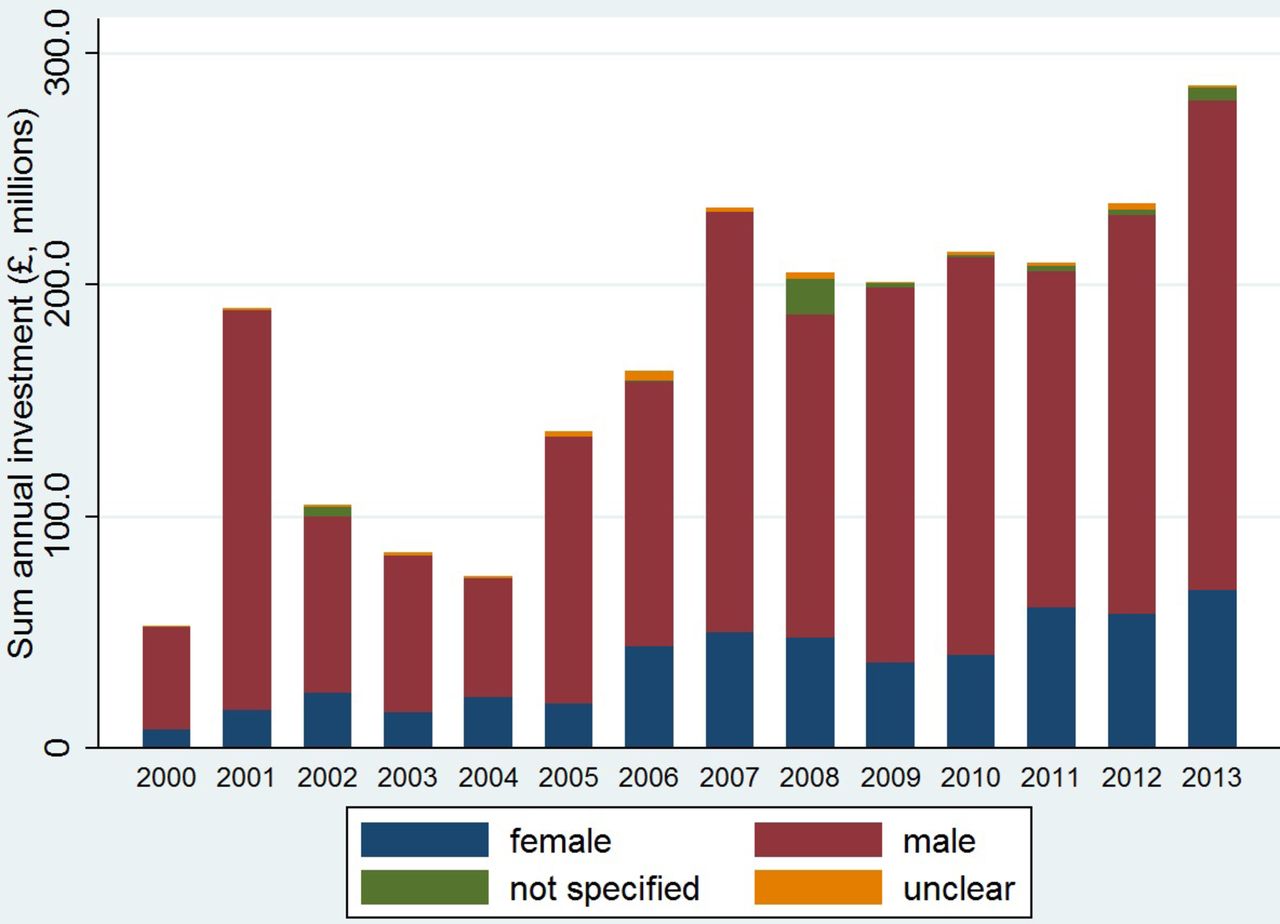
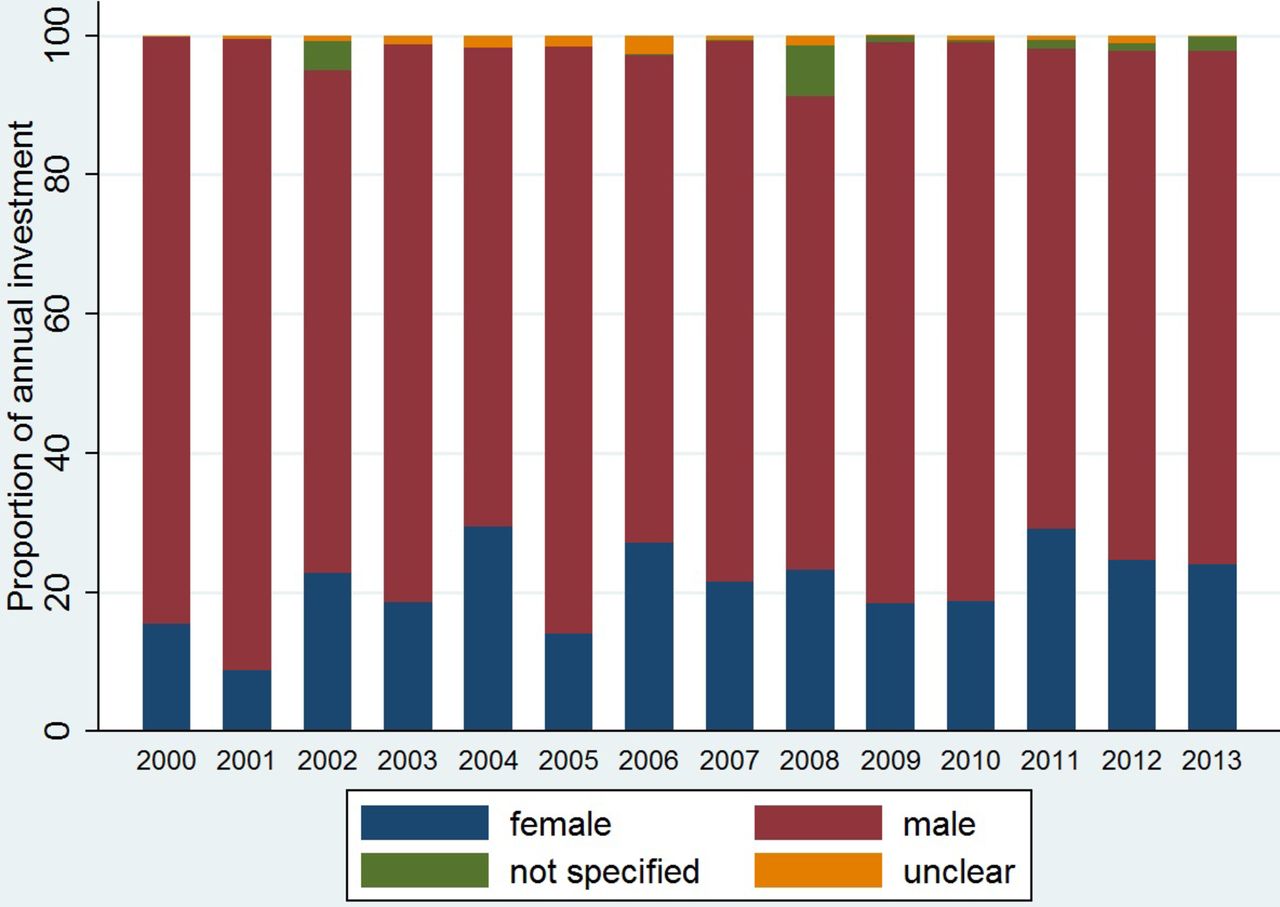
In our analysis of cancer research investment awarded by public and philanthropic funding bodies to UK institutions between 2000 and 2014, we identified 4299 funded studies suitable for inclusion. These studies represented a sum total monetary investment of almost £2.4 billion. Of these, 53 studies (1.2%, total investment of £33.2 million) did not specify PI name or gender, while we were unable to ascertain the gender of the named PI for a further 60 studies (1.4%, total investment of £21.8 million). Therefore, 4186 awards, totalling £2.33 billion, were included in our final gender analysis (table 1, figures 1 and 2).

Proportion of annual UK cancer research funding by gender.
{kind=link}
{kind=link}
Sum total of annual UK cancer research funding by gender.
Gender-specific UK cancer research funding by cancer site, disease theme, phase of research and development pipeline and by funding organisation
There were 2890 grants (69%) with a total value of £1.82 billion (78%) awarded to male PIs, while female PIs received 1296 grants (31%) with a total value of £512 million (22%). The median grant value was greater for men (£252 647; IQR: £127 343–£553 560) than for women (£198 485; IQR: £99 317–£382 650). Men received statistically significant larger grants in terms of median value compared with women (P<0.001). Similarly, mean grant value was greater for men (£630 324; SD £1 662 559) than for women (£394 730; SD: £666 574). Across all cancer research funding grants awarded, male PIs received 3.6 times the sum investment value, 1.6 times the mean award value and 1.3 times the median award values compared with their female counterparts.
There was a statistically significant difference between the genders in median grant value for research funding in three specific cancer sites. Men received 2.9 times the funding of women PIs in cervical cancer (P<0.001). Women received 2.4 and 2.0 times the funding of men in liver cancer (P<0.05) and mesothelioma (P<0.01), respectively. The differences in median funding for all other cancer sites were not statistically significant.
Some of the greatest apparent gender discrepancies in cancer funding by site are observed in awards for sex-specific cancers. For prostate cancer, male PIs receive 13.8, 3.5 and 2.0 times the investment of their female counterparts in total, mean and median funding, respectively. In cervical cancer research, men receive 9.9, 6.6 and 2.9 times the funding of women PIs in total, mean and median funding, respectively. In ovarian cancer research, there was a 4.6-fold, 5.7-fold and 1.2-fold difference between men and women in total, mean and median funding, respectively. And similarly in breast cancer, there was a 1.6-fold, 1.1-fold and 1.4-fold difference between men and women in total, mean and median funding, respectively.
Men received more total investment than women across all disease themes. A statistically significant difference in median grant value between the genders was present for 6 of the 14 disease themes included in our analysis. Men received greater median funding in all six of these disease themes: pathogenesis (1.2-fold difference, P<0.001); drug therapy (1.3-fold difference, P<0.001); diagnostic, screening and monitoring (1.6-fold difference, P<0.001); psychosocial (2.7-fold difference, P<0.01); men’s health (2.1-fold difference, P<0.05); and surgery (2.1-fold difference, P<0.05).
In keeping with our findings in our site-specific analysis, there was a consistent trend of increased funding for male PIs in sex-specific cancer research. In men’s health, there was a 14.1-fold, 3.7-fold and 2.7-fold difference in favour of male PIs in terms of total, mean and median investment, respectively. In women’s health, there was a 1.9-fold, 1.4-fold and 1.3-fold difference in favour of male PIs in total, mean and median investment, respectively.
Male PIs receive statistically significant greater median funding than women at all points of the R&D pipeline: preclinical (1.2-fold difference, P<0.001); phase I, II, or III clinical trials (1.9-fold difference, P<0.001); product development research (1.5-fold difference, P<0.01); cross-disciplinary research (1.2-fold difference, P<0.01); and public health (1.5-fold difference, P<0.001).
With the exception of the Biotechnology and Biological Sciences Research Council, all funding organisations on average awarded larger median awards to men than to women. These differences were statistically significant for four funding bodies: Medical Research Council (1.4-fold difference, P<0.001), charities—excluding Wellcome Trust (1.2-fold difference, P<0.001), Department of Health (1.6-fold difference, P<0.001) and Wellcome Trust (1.3-fold difference, P<0.05).
Discussion
In this first quantifiable systematic comparison of UK cancer research investment by PI gender for the period 2000–2013, we demonstrate that female PIs clearly and consistently receive less funding than their male counterparts in terms of total investment, the number of funded awards, mean funding awarded and median funding awarded. This apparent absolute and relative discrepancy in funding largely persisted regardless of analysis by cancer site, disease theme, research and development pipeline, or by funder.
Our study is a purely descriptive analysis which does not and cannot assess any potential explanatory mechanism that might underlie our observed gender discrepancy in cancer research funding. It cannot for example account for any potential influence of conscious or subconscious gender bias in cancer research funding decisions, and there is no evidence here of any bias on the part of funding bodies. We would caution against drawing conclusions regarding factors that may influence our reported observations from this study alone. Instead, we would advocate that these results be interpreted within the context of the existing scientific body of evidence on the topic. Nevertheless, this study provides further evidence into the apparent funding gap between the sexes in biomedical research.15 16 21
The attrition rate among women exceeds that of their male counterparts at every stage of scientific career progression.2 Existing data show that women are under-represented at the highest research posts in the UK, accounting for 23.2% of professors as of 2010,13 who would likely represent the great majority of PIs, particularly in larger awards. The lack of information on seniority and track record of funding applicants is an important gap in this study and precludes the conclusion that gender bias is responsible for the observed differences in cancer research funding. Indeed, if gender equality were to be achieved in medical science, a generational lag effect may be expected before this was reflected in funding data.
However, there is mounting evidence to suggest that the existing gender imbalances in researcher numbers do not wholly explain the observable gender gap in funding. At all stages of career progression, female scientists tend to experience lower success rates compared with male scientists when applying for research funding.25–27 Even when success rates are equal, female scientists tend to receive less in terms of award value.16 28 This is reflected by internal annual reports by Research Councils UK which represents a strategic partnership between seven of the UK research councils, awards from three of which have been included in our analysis. Female researchers made up 24% of standard grant applications (shorter in duration than 4 years or less than £1 million in value) and experienced a success rate of 25% compared with 29% among male applicants.29 This gender difference is even more pronounced for large grants (both longer than 4 years in duration and greater than £1 million in value) where women make up 17% of applicants and their success rate is 24% compared with 38% among their male counterparts.29
Within the UK, the Equality Challenge Unit set up the Athena SWAN charter in 2005. This scheme aims to tackle gender inequalities in STEMM by awarding bronze, silver or gold awards to universities, research institutions or departments which can demonstrate their commitment to reducing inequalities with measurable performance data. In 2011, the National Institute for Health Research (NIHR) decided that they would only consider application from research groups with at least a Silver Athena SWAN award,30 thereby further incentivising engagement with this scheme. Recent evidence suggests that there has been an associated positive impact in the advancement of gender equality as reported by participants of the scheme.31 Furthermore, in the latest call for research professorships, the NIHR guidance has specified a maximum of two nominations per institution at least one of which must be female.32
Further to those discussed, there are several additional limitations to our study. We are dependent on the accuracy of the original investment data sourced from the funding bodies. Private sector data was excluded from this study due to incompleteness of publicly available data from this sector. We were not able to include data on applicant success rate, the amount of funding initially requested, the gender co-applicants for each grant, the total gender pool of researchers in each disease area and within each type of science, or the proportion of awards made to clinical and non-clinical researchers, all of which would have provided a more holistic understanding of the research landscape. We lacked data on the academic rankings of PIs and were unable to adjust for seniority across both genders. Unfortunately, CRUK would not provide disaggregated funding data and so could not be included in our full analysis. However, the proportion of CRUK studies awarded by PI gender was comparable to our reported results (online supplementary appendix 1).
Supplementary file 1
While the gender discrepancies in cancer research funding observed over the 13-year study period are likely multifactorial, this study is fundamentally descriptive in nature and does not allow us to postulate the underlying mechanisms responsible for the observed gender differences. Nevertheless, this study demonstrates substantial gender imbalances in cancer research investment. We would strongly urge policy-makers, funders and the academic and scientific community to investigate the factors leading to our observed differences and seek to ensure that women are appropriately supported in scientific endeavour.
Acknowledgments
We would like to thank Joseph Fitchett for his contributions to the Research Investments in Global Health Study.
References
Footnotes
RA and MM are Joint senior authors.
RA and MM contributed equally.
Contributors CDZ, MM, MGH and RA conceived and designed the study. MGH, CDZ, BJG and MAE-H obtained the data. DCM and MGH conducted data formatting and statistical analysis. All authors helped interpret the findings. CDZ wrote the first draft of the manuscript with input from MM, MGH, RR, HO’C and RA. All authors provided input to subsequent drafts. All authors had full access to all of the data in the study and take responsibility for its integrity and the accuracy of data analysis.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data used are publicly available. Entire database and associated figures are permanently available with open access online (http://www.researchinvestments.org).