Article Text

Abstract
Objective To examine the associations between day of week and time of admission and 30-day mortality for six clinical conditions: ischaemic and haemorrhagic stroke, acute myocardial infarction, pneumonia, chronic obstructive pulmonary disease and congestive heart failure.
Design Retrospective population-based cohort analyses. Hospitalisation records were linked to emergency department and deaths data. Random-effect logistic regression models were used, adjusting for casemix and taking into account clustering within hospitals.
Setting All hospitals in New South Wales, Australia, from July 2009 to June 2012.
Participants Patients admitted to hospital with a primary diagnosis for one of the six clinical conditions examined.
Outcome measures Adjusted ORs for all-cause mortality within 30 days of admission, by day of week and time of day.
Results A total of 148 722 patients were included in the study, with 17 721 deaths within 30 days of admission. Day of week of admission was not associated with significantly higher likelihood of death for five of the six conditions after adjusting for casemix. There was significant variation in mortality for chronic obstructive pulmonary disease by day of week; however, this was not consistent with a strict weekend effect (Thursday: OR 1.29, 95% CI 1.12 to 1.48; Friday: OR 1.25, 95% CI 1.08 to 1.44; Saturday: OR 1.18, 95% CI 1.02 to 1.37; Sunday OR 1.05, 95% CI 0.90 to 1.22; compared with Monday). There was evidence for a night effect for patients admitted for stroke (ischaemic: OR 1.30, 95% CI 1.17 to 1.45; haemorrhagic: OR 1.58, 95% CI 1.40 to 1.78).
Conclusions Mortality outcomes for these conditions, adjusted for casemix, do not vary in accordance with the weekend effect hypothesis. Our findings support a growing body of evidence that questions the ubiquity of the weekend effect.
- public health
- quality in health care
- health policy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The examined conditions encompass a range of time sensitivity, interventions, acuity and prognosis, providing a gradient to assess potential causality of association.
The use of linked hospital admission and emergency department (ED) data allowed complete coverage of hospital admissions for the state, while minimising misclassification bias from time spent in ED and maximising validity and quality of diagnosis and comorbidity data.
The use of clinical cohorts of patients allows more precise adjustment for casemix than non-specific admissions.
Linkage to the deaths register allowed the capture of 30-day all-cause mortality. While mortality is a standard indicator, other outcomes may be more sensitive to clinical variations.
We focused on the New South Wales health system as a whole and did not explore the possible weekend effect at hospital level.
Introduction
In recent years, researchers and policy-makers have shown growing interest in the ‘weekend effect’, examining whether patients admitted to hospital at the weekend experience worse outcomes compared with patients admitted during the week. This effect has been observed in numerous studies of health systems around the world, for a wide range of conditions and procedures.1–6 Studies have also observed a ‘night effect’, suggesting that the phenomenon may extend to out-of-hours presentation more broadly.1–4
Considerable uncertainty remains as to the cause of the apparent effect of weekend and night-time (hereafter collectively ‘out-of-hours’) presentation on patient outcomes. Two main hypotheses have been proposed to explain the observed variation: these focus on healthcare service quality and on patient characteristics.2 The first hypothesis posits that the poorer outcomes seen among patients admitted on the weekend are explained by lower quality of care out of hours. More specifically, putative factors include lower staffing levels, fewer senior consultants and specialists, and reduced availability of diagnostic procedures.3 This hypothesis gained considerable traction with policy-makers and has contributed to the recent, controversial push towards 7-day hospital services in the UK.7
The second hypothesis proposes that the weekend effect is largely attributable to patient characteristics, and at least partly a data artefact resulting from insufficient information on patient characteristics in administrative datasets. There is little clear evidence that higher mortality is a consequence of staffing levels,7 and a number of studies have found no significant correlation between consultant seniority or specialist availability and mortality.8–11 There is also an increasing body of evidence to suggest that the weekend effect dissipates after adjustment for casemix,12 arrival by ambulance as a proxy for illness severity13 and a higher severity threshold for admission.12 This phenomenon may be influenced by self-selection, whereby patients wait until the weekend to present to hospital and may therefore present with more advanced disease, and less comprehensive note taking on the weekend limiting the ability to risk adjust.14
The night effect is less extensively studied than the weekend effect, and reasons for the night effect are usually presumed to be similar to the weekend effect. The few studies that have examined the effects of out-of-hours presentation on mortality in Australia have had mixed results.3 4 15 16 Previous studies have been limited by using in-hospital mortality only and therefore not capturing deaths that occurred postdischarge17 and reduced the ability to adequately risk adjust by focusing on clinically non-specific admissions.3 16 18 Further, previous studies have often relied on unlinked emergency department (ED) data,4 which contain limited or largely incomplete and inaccurate information on principal diagnosis and comorbidity, or unlinked hospitalisation data, which may be affected by misclassification bias due to time spent waiting in ED prior to admission.15 18
Overall, previous studies have shown that the out-of-hours effect does not apply to all clinical presentations and procedures.1–4 8 It is, therefore, beneficial to investigate conditions for which we can expect that the weekend effect is more likely to occur, based on theoretical grounds, on clinical plausibility or on previous evidence.2
We investigated the existence of the weekend effect and the night effect for acute hospitalisations for various conditions, comprising ischaemic stroke, haemorrhagic stroke, acute myocardial infarction (AMI), pneumonia, chronic obstructive pulmonary disease (COPD) and congestive heart failure (CHF), across all hospitals in New South Wales (NSW). These conditions provide insights into a range of aspects of healthcare, including timely delivery of interventions, surgical services, differences in acuity and prognosis, and provide a gradient to assess potential causality of association as they vary in the importance of immediate care. We predicted that if day and time effects exist, they would show strongest effects for the most urgent conditions (stroke and AMI) and be weakest for patients with the least urgent conditions (pneumonia and COPD). We hypothesised that presentations on Saturdays and Sundays would show higher 30-day mortality for the six conditions than presentations that occurred during the week, and that night-time presentations would show higher mortality than presentations that occurred during the day.
Methods
Retrospective cohort analyses were performed for the six conditions. Cohorts were identified from all admissions to NSW public and private hospitals for the period of 1 July 2009 to 30 June 2012, extracted from the NSW Admitted Patient Data Collection, which is a census of all hospital admissions in NSW. These data were linked to ED attendances in all NSW public hospitals recorded in the ED Data Collection, representing approximately 85% of all emergency presentations in NSW.19 20 ED data were linked to allow the capture of the start day and time of the patients’ contact with the hospital system for the episode of illness, minimising any bias imposed by time spent in the ED that may affect the day and time of hospitalisation, since patients may spend longer in the ED before admission at night or on weekends. Mortality data were obtained from the NSW Deaths Register. Data were linked by the NSW Centre for Health Record Linkage using probabilistic methods based on personal identifiers. The estimated false-positive rate for the current version of the Master Linkage Key is 5 per 1000.21
The principal diagnosis in the patient record, coded using International Classification of Diseases, 10th Revision, Australian modification, was used to identify each clinical cohort. Only complete records of admissions coded as acute and emergency were included. The proportion of records excluded for missing values on key variables such as age, sex, date of admission and separation, type of care and emergency status was less than 0.1%. Patients aged less than 15 years (ischaemic stroke, haemorrhagic stroke, AMI), 18 years (pneumonia) or 45 years (COPD, CHF) were excluded, consistent with existing mortality indicator definitions for these conditions, due to low mortality rates among these groups.22 23 AMI can be classified as ST-elevated myocardial infarction (STEMI) or non-STEMI (non-STEMI) based on the ECG reading or unspecified AMI when diagnostic records are unavailable. STEMI is associated with higher mortality at 30 days compared with non-STEMI, and the unspecified group is a heterogeneous mix of critically unwell patients who died before their AMI could be specified and patients for whom diagnostic records were less precise, so patients with AMI with a non-specific infarction were excluded to allow adjustment for STEMI.22 23 Transfers and multiple contiguous hospitalisations were considered as a single period of care. For patients with multiple periods of care during the study period, only the last period of care was included in the analyses.
Mortality was defined as death (in or out of hospital) occurring within 30 days of the start of the period of care. The day of week of presentation was defined as the first day of contact with the hospital system for the period of care (either hospital admission or ED presentation). Patients dead on arrival to ED and not admitted to hospital were excluded. An ED presentation was considered relevant for the hospital admission if it occurred on the same day or previous day, as the hospital admission. Same-day ED presentations were only included if the time was recorded as before the hospital admission time. In this study, the weekend comprises Saturday and Sunday, while weekdays are defined as Monday through Friday. Night-time presentation was defined as first presentation between 18:00 and 07:59, using hospital admission time or ED presentation time as described.
Random-effects logistic regression models were used to investigate associations between day of week, or time of presentation, with mortality. To account for clustering of patients within hospitals, hospitals were considered as random effects in the regression models. Risk adjustment was performed to account for casemix factors including age (continuous, tested for curvilinearity), sex, year and comorbidities. Condition-specific comorbidity sets defined by the Australian Commission for Safety and Quality in Health care were used as the basis for building risk adjustment models for each condition, where available (ischaemic stroke, haemorrhagic stroke, AMI, pneumonia), while COPD and CHF used Elixhauser comorbidities.22 Availability of thrombolysis treatment was also considered as a predictive variable for ischaemic stroke, and STEMI status was considered for AMI. Comorbidities were captured across all hospital admissions over a 1-year period prior to the index admission. Interactions between day of the week and night-time presentations were also explored in the final models using likelihood ratio tests.
Models were selected using backwards selection.24 Factors with a p value of less than 0.2 in the univariate analyses were included in the initial full models. Variables with a p value of less than 0.05 were retained in the model. Variables that were not significant at the 20% level in the univariate models were then checked for significance in the backwards-selected model, and retained in the final model where p<0.05. Overall performance of the models was assessed using c-statistics. In order to capture daily variation, 30-day mortality risks for each day of the week were compared against a reference weekday (Monday). We define observation of a weekend effect as significantly higher odds of 30-day mortality on weekend days (Saturday and Sunday) compared with Monday. To validate our findings, additional analyses were performed comparing weekend days against weekdays. Statistical analyses were performed using SAS V.9.4 and STATA V.12.1.
Results
There were a total of 213 834 acute, emergency hospital admissions for the conditions of interest during the study period. There were 10 658 admissions excluded as they did not meet the eligibility criteria for age, and 2161 patients were excluded who had a non-specified AMI. After accounting for transfers and multiple admissions, there were 148 722 patients were included in the study (table 1). There were 17 721 deaths within 30 days of admission (11.9%). A total of 127 268 admissions were linked to an ED presentation (85.6%). The clinical cohorts comprised between 5740 (haemorrhagic stroke) and 44 508 (pneumonia) patients who were admitted or presented to between 133 and 183 hospitals. Characteristics of patients are provided by day of week and time of day of arrival in table 2.
Numbers of patients admitted to hospital in NSW between July 2009 and June 2012 for the conditions examined, number and percentage of deaths within 30 days, by day and time of presentation*
Demographic and clinical characteristics of patients with acute, emergency hospital admissions for the conditions of interest by day of week and time of day of presentation*, NSW, July 2009–June 2012
The most frequent day of presentation was Monday, while Saturdays and Sundays had fewer presentations than weekdays for all conditions. More patients were admitted during daytime than at night, regardless of condition.
There were no significant associations in the univariate analyses between mortality and day of week, for haemorrhagic stroke, AMI, pneumonia or CHF (table 3). There was significant variation in unadjusted 30-day mortality by day of week for ischaemic stroke and COPD; however, this did not show a strict ‘weekend effect’ (ischaemic stroke: Friday, Saturday and Sunday significantly higher than Monday; COPD: Thursday, Friday and Saturday significantly higher than Monday).
Unadjusted ORs for 30-day mortality for day of week and time of day of presentation*
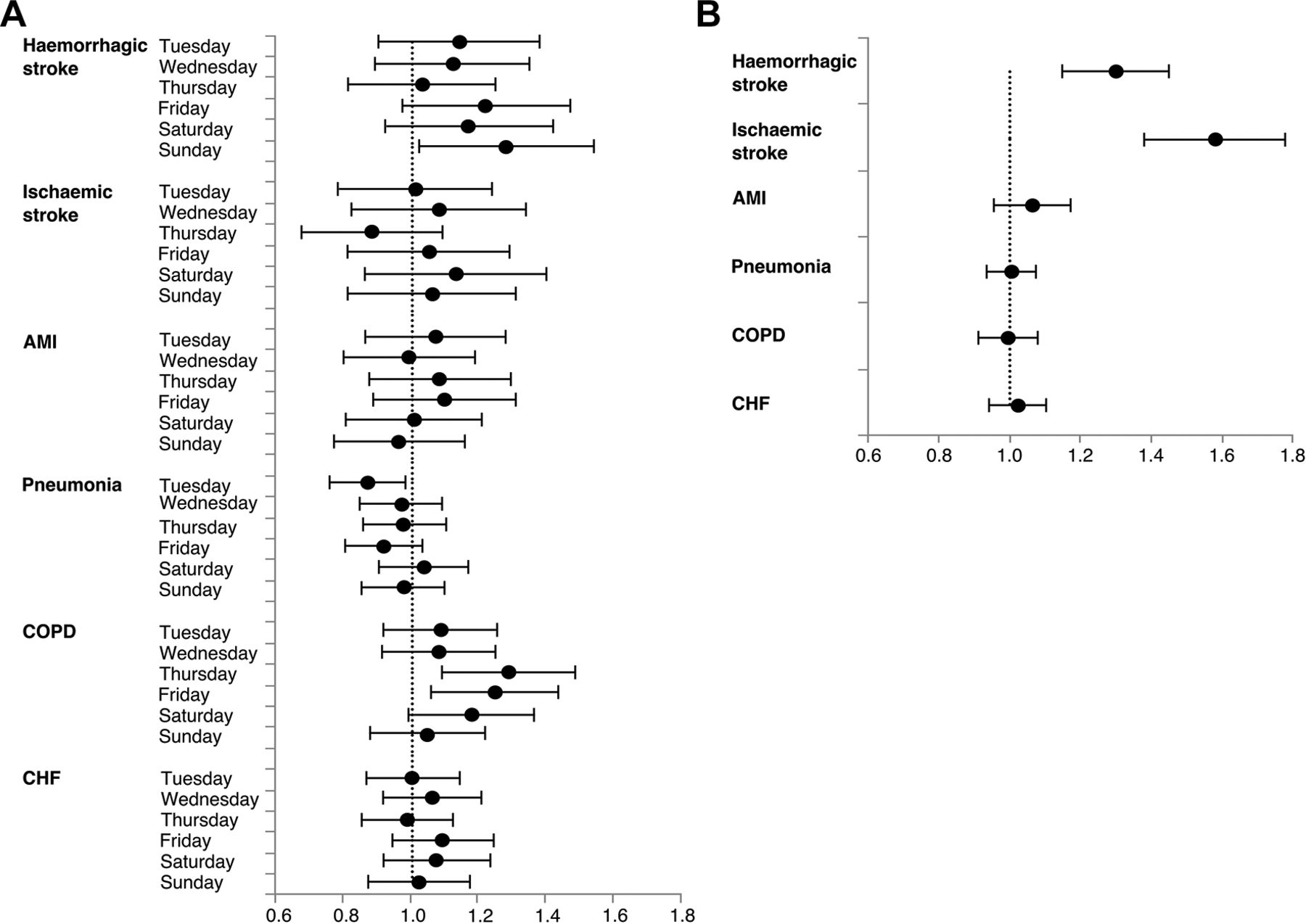
There was no significant difference in 30-day mortality by day of week after adjustment for casemix and other factors for five of the six conditions (table 4, figure 1). While Friday and Sunday presentations had significantly higher mortality than Monday for ischaemic stroke, overall day of the week was not significant in the model. Significant variation in mortality by day of week for COPD was not consistent with a weekend effect (with Thursday, Friday and Saturday being associated with higher mortality compared with Monday).
{kind=link}
(A) Adjusted ORs for 30-day mortality for day of week of presentation by clinical condition. Reference group is Monday (dotted line). (B) adjusted ORs for 30-day mortality for presentation to hospital at night compared with during the day, by clinical condition. AMI, acute myocardial infarction; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease.
Adjusted ORs for 30-day mortality by day of week and time of day of presentation*
Supplemental material
There was evidence for higher mortality among patients with ischaemic and haemorrhagic stroke who presented to hospital overnight. This night effect was observed in both the unadjusted and adjusted analyses (tables 3 and 4). There was no evidence of increased mortality among night admissions for the other conditions. There were no significant interactions between day of week and time of day, after adjustment for confounding factors, for any of the conditions.
The models performed moderately well, with c-statistics ranging from 0.68 to 0.82 (ischaemic stroke: 0.73, haemorrhagic stroke: 0.68, AMI: 0.81, pneumonia: 0.82, COPD: 0.74, CHF: 0.72).
Results from the analyses comparing 30-day mortality on pooled weekend versus weekdays showed that the weekend was associated with a higher unadjusted likelihood of 30-day mortality compared with weekday for ischaemic stroke and pneumonia (table 5). However, after taking into account other risk factors, no significant differences were observed in 30-day mortality between weekdays and weekend for any of the conditions studied.
Unadjusted and adjusted ORs for 30-day mortality for day of week, categorised as weekend versus weekday, of hospital presentation* using random-effect logistic regression models
Discussion
Main findings
Mortality outcomes do not vary in accordance with the weekend effect, after adjusting for casemix, for patients admitted to hospital with stroke, AMI, pneumonia, COPD or CHF in NSW. We found increased mortality for patients with stroke presenting to hospital at night, with no evidence for the night effect for the remaining conditions.
Our findings support a growing body of evidence that disputes the ubiquity of the weekend effect.7 12 14 15 25 26 Of the six conditions investigated in this study, only ischaemic stroke and COPD showed significant variation in crude mortality risk by day of week of presentation. Significant variation remained after risk adjustment for COPD only, and this was not consistent with predictions for the weekend effect, with the highest odds of death within 30 days was found for those who presented on Thursday and Friday. When weekend and week days were pooled, there were no significant differences in odds of death after adjusting for other risk factors. This is consistent with studies which have shown more complex patterns of temporal variation in that there are some days/times that are different but not specifically ‘the weekend’.4 17 26 27
While findings from previous studies for stroke,11 14 28 29 AMI15 30 and COPD15 31 have been conflicting, our results are consistent with those that found no weekend effect (stroke,1 14 26 32 AMI,1 33 COPD.15 A recent meta-analysis found no weekend effect for COPD and pneumonia, although it did find significant effects for intracerebral haemorrhage, ischaemic stroke and myocardial infarction.34 However, on comparing effects between continents, Oceania was found to have the lowest overall increase in odds of death (OR=1.04; compared with South America, OR=1.47), suggesting that the weekend effect may be highly heterogeneous and dependent on clinical conditions and on hospital contexts, regional policy and other factors that may vary widely by geographical setting.
We observed that a number of admissions were lower at weekends in NSW, and that the number of deaths within 30 days are generally proportionate to the number of admissions. This is in contrast to the findings of previous studies.1 6 12 35 There are a number of differences between our study and some of the previously published work which may explain these differences. The use of 30-day mortality through linkage to the Deaths Register as opposed to in-hospital death1 3 6 12 13 35 allows the capture of patients who died in hospital, and those who died in the community due to variation in care or early discharge. This provides a more complete picture of mortality.
Further, our study has examined six specific clinical conditions, as opposed to all emergency conditions.3 4 12 35 Not all emergency admissions have the same urgency or acuity for treatment, and the conditions we have examined are useful indicators that encompass a range of time sensitivity, interventions, acuity and prognosis. The use of clinical cohorts of patients allows more precise adjustment for casemix than considering non-specific admissions. We found no effect on mortality of weekend presentation either in conditions expected to be less sensitive to reduced staffing and services, nor among the more severe, acute conditions, which confers confidence in the validity of our findings. Our analyses comprised 3 years’ complete population data for NSW with cohorts ranging from over 5000 to 44 000, which should provide sufficient power to detect statistically significant differences.
In contrast to other studies, the use of linked hospitalisation and ED data provides complete coverage of hospital admissions for the conditions of interest in NSW, and minimises several potential biases. While most studies use either hospital admission data1 6 35 or ED data,3 4 the use of linked data in this study minimises misclassification bias in day and time of presentation caused by time spent in ED prior to admission. Additionally, the use of hospitalisation data from the index and historical admissions of the patients allowed us to maximise the detail and quality of diagnoses and comorbidities. This increases our confidence in our finding of no evidence for increased mortality associated with weekend presentation.
We found significantly higher adjusted risk of death for patients with ischaemic and haemorrhagic stroke who presented at night compared with those who presented during the day. This is consistent with other studies of stroke.26 28 This finding may reflect factors specific to stroke, such as that strokes occurring at night may take longer to recognise due to reduced activity, and may result in delayed seeking of treatment and therefore higher mortality. That we only observed the night effect for patients with stroke suggests that this variation is probably not attributable to system-wide deficiencies. However, further research to explore reasons for the increase in mortality for patients with stroke admitted at night, and the observed variation in mortality for COPD by day of presentation, including potential contributions from poorer community care, will help to understand whether these excess deaths are preventable.
Our study is limited by a lack contextual information in our data about the differences in weekend and weekday or night-time and day time practice, such as the availability of clinical or laboratory staff. It would be interesting to consider the results on the level of individual hospitals, as hospital variation in quality of care on weekends may be masked in this type of global analysis.
Mortality is a useful indicator for health system performance and for evaluating unwarranted variation. However, it is an extreme outcome, and it may be a blunt tool that could mask some variation in patient outcomes. Further research is needed to determine whether lower staffing levels and resource access on weekends and out-of-hours may exhibit effects on other outcomes or processes, such as adverse events, delays in test results or care, or other quality indicators. Across healthcare systems, different models of care or availability of out-of-hours specialist services may affect any weekend effect seen locally.
Unlike many other studies, our findings do not suggest a threshold effect or differing propensity to admit patients across days of the week. This may be a reflection of the particular conditions that our study focused on or it may be the case that there is no weekend effect in NSW public hospitals. While our study does address both weekend effect and night-time effect, it is possible that more complex patterns of temporal variation exist that could not be observed using our models.’
Conclusion
By identifying patients admitted through ED, and taking out-of-hospital deaths into account, this study was able to investigate the weekend effect by following the patient journey from prior to admission to after discharge. We found no evidence for a strict weekend effect in 30-day mortality for patients admitted with ischaemic or haemorrhagic stroke, AMI, pneumonia, COPD or CHF. The finding of a night effect for stroke, and some variation between days for COPD, highlights that temporal variation in patient outcomes is complex and may have a variety of causes. Our findings increase the weight of evidence challenging the existence of the weekend effect.
Acknowledgments
We thank the NSW Ministry of Health for access to population health data and the NSW Centre for Health Record Linkage for linking the data sets. We thank Lisa Corscadden for helpful comments on the manuscript. HJB is supported by the NSW Biostatistics Training Program.
References
Footnotes
Contributors HJB, SM-P, H-YC, JK, KS and J-FL contributed to the study design. HJB and SM-P cleaned and analysed the data and HJB produced the figure and tables. All authors contributed to the interpretation of the results. HJB drafted the manuscript, and all authors contributed to revising the manuscript. All authors approved the final version of the manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval New South Wales Ministry of Health approves our use of these deidentified data for research purposes.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Privacy restrictions for the datasets used in this study prohibit free online availability. Access to these data may be sought from the data custodians, the New South Wales Ministry of Health.
Correction notice This article has been corrected since it first published. In the article title ‘A retrospective clinical analyses’ was corrected to ‘A retrospective clinical analysis’.