Article Text

Abstract
Purpose The objective of the current study was to explore the role of CHA2DS2-VASc score in predicting incidence of atrial fibrillation (AF) in patients with type 2 diabetes mellitus (DM). Furthermore, the use of the CHA2DS2-VASc score for stratifying new-onset AF risk in patients with DM and with/without hyperosmolar hyperglycaemic state (HHS) was also compared.
Methods The study subjects were identified from Longitudinal Health Insurance Database provided by the National Health Research Institutes. The patients with DM were divided into two groups based on a history of HHS or not. The predictive ability of CHA2DS2-VASc score for stratifying new-onset AF risk in the two groups was calculated using the area under the curve of receiver-operating characteristic (AUROC).
Results The present study involved a total of 69 530 patients with type 2 DM. Among them, 1558 patients had a history of HHS, whereas 67 972 patients did not. The AUROC of the CHA2DS2-VASc score as a predictor of incident AF in patients with DM and with/without HHS was 0.67 (95% CI 0.59 to 0.75) and 0.71 (95% CI 0.70 to 0.72), respectively.
Conclusions To conclude, we reported for the first time on the assessment of CHA2DS2-VASc score for incident AF risk discrimination in patients with type 2 DM. We further found that the predictive ability of the CHA2DS2-VASc score was attenuated in patients with type 2 DM and with HHS in comparison with those without HHS.
- atrial fibrillation
- CHA2DS2-VASc score
- diabetes mellitus
- hyperosmolar hyperglycemic state
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
We reported for the first time on the application of CHA2DS2-VASc score for stratifying incident atrial fibrillation risk among patients with type 2 diabetes mellitus (DM).
We found that the predictive ability of the CHA2DS2-VASc score was attenuated in patients with DM and hyperosmolar hyperglycaemic state (HHS) compared with those without HHS.
The use of International Classification of Disease Ninth Revision codes is a critical limitation in the current study.
However, the codes have been used in many epidemiological studies, and the results from this big dataset have been reported with high reliability.
Introduction
Type 2 diabetes mellitus (DM) is one of the major issues in public health worldwide due to its increasing incidence and prevalence.1 2 Indeed, hyperosmolar hyperglycaemic state (HHS) is a major acute complication in patients with DM.3–8 The common triggers for HHS include poor medication compliance, fluctuation of blood glucose or other stress responses.3–8 The prognostic impact of atrial fibrillation (AF) could not be overemphasised due to its associated high morbidity and mortality.9 10 In comparison to the therapeutic strategy for AF treatment, the prevention for incident AF gained relatively less attention.9–11
The link between DM and AF has been investigated; indeed, DM is an important risk factor for AF development and a crucial predictor of adverse cardiovascular outcomes in patients with AF.12–16 Several pathogenesis mechanisms underlying the link between DM and AF were proposed, including structure and electric remodelling, oxidative stress reaction, inflammatory response and autonomic dysfunction.12–16
CHA2DS2-VASc score, a simple, practical and user-friendly scoring scheme which was initially used for stroke risk discrimination among patients with AF has gained widely use for predicting different cardiovascular outcomes in different population recently.17–19 Hence, using a large nationwide dataset, the objective of the current study was to explore the role of CHA2DS2-VASc score in predicting incidence of AF in patients with DM. Furthermore, the use of the CHA2DS2-VASc score for discriminating new-onset AF risk in patients with DM and with/without hyperosmolar hyperglycaemic state (HHS) was also compared.
Methods
Data source
This retrospective cohort study was assembled using data from Longitudinal Health Insurance Database (LHID) of 2000 provided by the National Health Research Institutes (NHRI). The National Health Insurance (NHI) programme in Taiwan, which started from 1 March 1995, includes approximately 99% of Taiwan’s population.20 The LHID includes longitudinal data and comprises a total of 1 000 000 people randomly selected from the NHI Registry for Beneficiaries of 2000. More details on the LHID have been described elsewhere.21 22 Disease was operationalised using the International Classification of Disease, Ninth revision (ICD-9) codes. The Ethics Review Board of China Medical University and Hospital in Taiwan approved this study (CMUH-104-REC2-115).
Sampled participants
The study subjects were defined as those over 20 years old with a new diagnosis of type 2 DM (ICD-9-CM codes 250.x0 or 250.x2) between 1 January 2000 and 31 December 2011. The patients with DM were divided into two groups based on a history of hyperosmolar hyperglycaemic state (HHS) (ICD-9-CM codes 250.20 or 250.22) or not. The index date was assigned as the first DM diagnosis date. We excluded patients who had a diagnosis of AF (ICD-9-CM code 427.31) before the index date. All study subjects received follow-up from the index date and terminated while they were removed from the health insurance programme, death, AF occurrence or the end of the study (31 December 2011). We used the CHA2DS2-VASc score to measure incident AF risk among patients with type 2 DM and with and without HHS.23 24 The CHA2DS2-VASc score was calculated for each patient by assigning one point for heart failure, type 2 DM, hypertension, vascular disease, sex category (female) and an age between 65 and 74 years; and two points for a history of ischaemic stroke/transient ischaemia attack (TIA) or an age 75 years or older.
Baseline comorbid medical illness, such as hyperlipidaemia (ICD-9-CM code 272), chronic obstructive pulmonary disease (COPD) (ICD-9-CM code 491, 492, 496), chronic kidney disease (CKD) (ICD-9-CM codes 585, 586, 588.8, 588.9), hyperthyroidism (ICD-9-CM code 242), sleep disorders (ICD-9-CM codes 307.4, 780.5), gout (ICD-9-CM code 274) and Charlson Comorbidity Index (CCI) score were identified and included in the current study.
Statistical analysis
To display the distribution of baseline characteristics of study population, the age, sex, underlying disease whether captured in the CHA2DS2-VASc score or not between patients with DM and with/without HHS were shown as number and percentage or mean and SD. The χ2 test and t-test were applied to examine the distribution difference for category variables and for continuous variables, respectively. The CHA2DS2-VASc score-specific incidence density rate of new-onset AF per 1000 person-years (PYs) was calculated in each group. The cumulative incidences of new-onset AF among patients with type 2 DM and with or without HHS stratified by CHA2DS2-VASc score were assessed using the Kaplan-Meier method. The differences between the cumulative incidence curves were evaluated using a log-rank test. Univariable and multivariable Cox proportional hazards models were adopted to estimate the HRs and the 95% CIs for incident AF associated with the CHA2DS2-VASc score in the two groups. CCI score and comorbidities which were not captured in the CHA2DS2-VASc score were included in the multivariable models for adjustment, including hyperlipidaemia, COPD, CKD, hyperthyroidism, sleep disorders and gout. The predictive ability of CHA2DS2-VASc score for stratifying AF risk in the two groups was calculated using the area under the curve of receiver-operating characteristic (AUROC). The AUROC integrated measures of sensitivity and specificity of the variable range from 0 to 1. The statistical significance was accepted at a two-tailed p value lower than 0.05.
Results
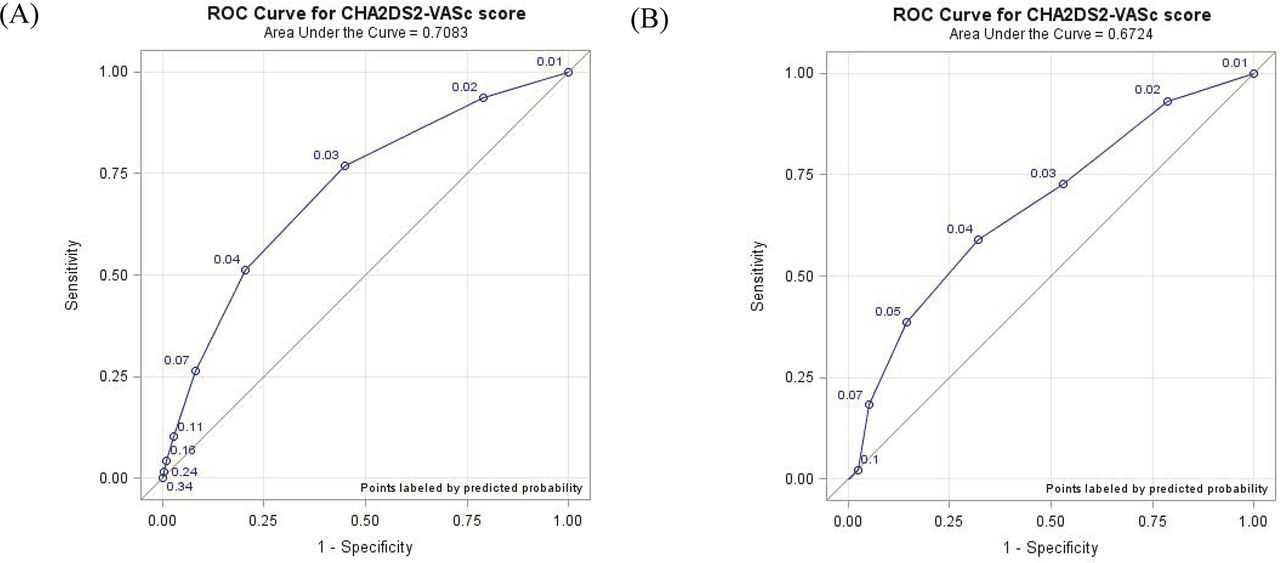
The study involved a total of 69 530 patients with type 2 DM. Among them, 1558 patients had a history of HHS, whereas 67 972 patients did not (table 1). The mean age of the HHS group and the non-HHS group were 60.8 and 57.0 years, respectively (p<0.001). The percentage of male gender in the HHS group was significantly higher than the non-HHS group (57.5% vs 52.2%, p<0.001). Compared with the non-HHS group, the HHS group significantly had more comorbid congestive heart failure (CHF), cerebrovascular accident (CVA) or TIA, COPD and CKD. Most study participants had a CCI score of 0 (61.8% vs 81.3%). The mean CHA2DS2-VASc score of the HHS group and the non-HHS group were 2.89 (SD=1.53) and 2.60 (SD=1.31), respectively (p<0.001). The mean follow-up period for the HHS group and for the non-HHS group were 6.64 (SD=3.51) years and 6.20 (SD=3.49) years, respectively. Among patients with type 2 DM and without HHS, the incidence of new-onset AF increased from 0.88% for those with a CHA2DS2-VASc score of 1 to 9.55% for those with a score of 6 or greater (figure 1A). The incidence of AF increased from 1.42 per 1000 PYs for patients with DM and without HHS with a CHA2DS2-VASc score of 1 to 22.6 per 1000 PYs for those with a CHA2DS2-VASc score of ≧6 (table 2). After adjusting for the comorbidities of hyperlipidaemia, COPD, CKD, hyperthyroidism, sleep disorders, gout and CCI score, the risk of incidence of AF among patients with DM and without HHS increased with increasing CHA2DS2-VASc score. The incidence of new-onset AF increased from 0.93% to 9.41% when the CHA2DS2-VASc score increased from 1 to 6 or greater among patients with DM and HHS (figure 1B). Among patients with DM and HHS, in comparison with patients with a CHA2DS2-VASc score of 1, the corresponding adjusted HRs of new-onset AF for those with a CHA2DS2-VASc score of 5 and ≧6 were 8.59 (95% CI 2.26 to 32.6) and 16.1 (95% CI 3.79 to 68.8), respectively. The cumulative incidence curves of new-onset AF stratified by CHA2DS2-VASc score in patients with DM without and with HHS were shown in figure 2A,B (log-rank test p<0.001). Table 3 reports the sensitivity, specificity and AUROC for the CHA2DS2-VASc score in relation to new-onset AF in the two study groups. Among the non-HHS group, discrimination value of the CHA2DS2-VASc score for incident AF results in AUROC of 0.71 (95% CI 0.70 to 0.72) (table 3 and figure 3A).The cut-off value of the CHA2DS2-VASc score for incident AF was 3 (sensitivity: 76.8%; specificity: 55.0%). Among HHS group, the AUROC of the CHA2DS2-VASc score as a predictor of AF was 0.67 (95% CI 0.59 to 0.75) (table 3 and figure 3B). The cut-off value of the CHA2DS2-VASc for incident AF was 4 (sensitivity: 59.1%; specificity: 68.0%).

Incidence of new-onset atrial fibrillation in patients with type 2 diabetes mellitus without hyperosmolar hyperglycaemic state (A) and with hyperosmolar hyperglycaemic state (B) with different CHA2DS2-VAS scores.

Cumulative incidence curves of new-onset atrial fibrillation stratified by CHA2DS2-VASc score in patients with type 2 diabetes mellitus without hyperosmolar hyperglycaemic state (A) and with hyperosmolar hyperglycaemic state (B).

{kind=link}
{kind=link}
{kind=link}
ROC curve for CHA2DS2-VASc score in predicting new-onset atrial fibrillation in patients with type 2 diabetes mellitus without hyperosmolar hyperglycaemic state (A) and with hyperosmolar hyperglycaemic state (B). ROC, receiver operating characteristic.
Baseline characteristics of patients with DM and with/without HHS
Incidence and HRs of AF in DM patients with or without HHS stratified by CHA2DS2-VASc score
Sensitivity, specificity and predictive ability (AUROC and the 95% CI) for CHA2DS2-VASc score in relation to AF in DM patients with and without HHS
Discussion
To date, we reported for the first time on the application of CHA2DS2-VASc score for stratifying incident AF risk among patients with type 2 DM. Furthermore, we found that the predictive ability of the CHA2DS2-VASc score was attenuated in patients with DM and HHS compared with those without HHS.
The association between DM and AF has been addressed previously.12–16 Early studies have discussed the prognostic impact of DM among patients with AF; indeed, one of the major players of CHA2DS2-VASc score, an important risk scoring scheme for predicting stroke in patients with AF, is DM.12–19 Furthermore, the causal relationship between DM and AF has also been investigated; and currently proposed molecular mechanisms underlying the link include atrial mechanical and electrical remodelling triggered by high glucose environment, the fluctuation of the blood sugar, inflammatory response, dysregulation of autonomic system and oxidative stress reaction.12–16
Compared with the management strategies for AF intervention, identification and detection for new-onset AF gained relatively less attraction.9–11 Although prediction models for incident AF were currently available, the major limitations of the scoring system were user unfriendly and relatively complicated for clinical use.25 26 Thus, using a large-scale nationwide dataset, we sought to identify the predictive role of CHA2DS2-VASc score in this population. Although patients with DM and HHS tend to have more comorbidity; after adjustment for several risk factors for AF development other than the components of the CHA2DS2-VASc score, the ability of the score for discriminating new-onset AF risk in patients with DM and HHS was attenuated as opposed to those without HHS. Furthermore, patients with DM and who had a history of HHS tend to be at a significantly increased risk for incident AF at a relative higher threshold. Possible explanation for our observations is that a previous exposure of HHS in patients with DM might enhance the phenomenon of oxidative injury, endothelial damage and stress response, which in turn could probably attenuate the ability of the CHA2DS2-VASc score for incident AF risk stratification in this population.12–16 The results presented here should still be verified by other large prospective investigations.
Limitations
First, the use of ICD-9 codes is a critical limitation in the current study. However, the codes have been used in many epidemiological studies and the results from this big dataset have been reported with high reliability.27 28 Second, this study lacks considerations of smoking, nutrition, obesity, family history and physical activity. Finally, the use of the therapeutic procedures, such as atrial fibrillation ablation, pacemaker implantation, cardiac catheterisation, and the severity of the diseases were not included in the current study.
Conclusions
To conclude, we reported for the first time on the assessment of CHA2DS2-VASc score for incident AF risk discrimination in patients with type 2 DM. We further found that the predictive ability of the CHA2DS2-VASc score was attenuated in patients with type 2 DM and HHS in comparison with those without HHS. The findings presented here should still be confirmed by further large prospective studies.
References
Footnotes
Contributors Wei-Syun Hu: conceptualisation, methodology, software, validation; formal analysis, investigation, resources, data curation, writing (original draft preparation), writing (review and editing), visualisation, supervision, project administration and funding acquisition.Cheng-Li Lin: formal analysis, investigation, resources and data curation.
Funding This study was supported in part by Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW106-TDU-B-212-113004).
Disclaimer The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Patient consent Not required.
Ethics approval Institutional Review Board (IRB) of China Medical University and Hospital in Taiwan (CMUH104-REC2-115).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.