Article Text

Abstract
Objectives To determine incidence, associated factors, outcomes and geographical occurrence of born before arrival (BBA) in New South Wales, Australia.
Design A linked population data study involving population-based surveillance systems was undertaken for the years 2000–2011.
Setting New South Wales, Australia.
Participants All women who underwent BBA compared with women who birthed in hospital/birth centre settings.
Results During the time period, there were 1 097 653 births and a BBA rate of 4.6 per 1000 births. The BBA rate changed from 4.2 to 4.8 per 1000 births over time (p=0.06). Neonates BBA were more likely to be premature (12.5% compared with 7.3%), of lower birth weight (209.8 g mean difference) and/or be admitted to a special care nursery or neonatal intensive care unit (20.6% compared with 15.6%). The perinatal mortality rate was significantly higher in the BBA cohort (34.6 compared with 9.3 per 1000 births). Women in the BBA cohort were more likely to be in the lowest socioeconomic decile, multiparous, have higher rates of smoking (30.5% compared with 13.8%) and more likely to suffer a postpartum haemorrhage requiring transfusion than the non-BBA cohort (1.5% compared with 0.7%). The most commonly occurring complications for neonates were suspected infection (6.9%), hypothermia (6.9%), respiratory distress (5.4%), congenital abnormality (4.0%) and neonatal withdrawal symptoms (2.4%). BBA more commonly occurred in geographical areas where the distance to a maternity unit is >2 hours drive and in coastal regions where there is also a high rate of homebirth.
Conclusion BBA occurs more frequently in multiparous women of lower socioeconomic status. There potentially is an effect of geography on the occurrence of BBA, as geographical area of high homebirth and BBA coexists, indicating that freebirth followed by an unplanned transfer to hospital may be occurring.
- neonatal mortality
- birth
- homebirth
- data linkage
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The uniqueness of this study in establishing incidence data with regard to born before arrival (BBA) due to the size and detailed variables within the datasets used.
The associations made between geographical area of high homebirth and high BBA rates, suggesting a potential marker of freebirth in these areas.
Lack of maternal body mass index data which would enable further examination of associated factors.
The combining of neonatal intensive care unit/special care nursery data in the datasets which may not always be indicative of the degree of neonatal morbidity.
This paper uses a definition of viability of ≥20 weeks gestation for inclusion, whereas the WHO definition is ≥22 weeks gestation. The former definition is standard in Australia and allows for increased generalisability of results in this setting.
Introduction
The term born before arrival (BBA) encompasses the birth of any infant ≥20 weeks gestation and >400 g birth weight which occurs outside of the hospital/birth centre setting, excluding planned home births attended by a health professional.1 These births occur within women’s homes, en route to the hospital or in ambulances and are not attended by a midwife or medical officer. The incidence of BBA occurring is usually low with rates varying between 1 per 1000 births in Finland,2 5.2 per 1000 births in UK3 to 19.9 per 1000 births in the USA.4 The average Australian rate for the years 1992–2011 was 4.2 per 1000 births.5 There is some evidence that rates are increasing across Australia, with one Australian state (Queensland) reporting an increase in the rate of BBA between 1999 and 2008 (2.4–3.7 per 1000 births).6 In Ireland,7 an increase in BBA was seen from 2006 to 2009 (2.6–5.0 per 1000 births).
Geographical analysis of where these births occur in both the Australian and international setting concluded that a BBA was more likely to occur in settings where there were large distances from maternity units, or in urban areas in close proximity to maternity units,8 9 and this has been supported recently within the Queensland setting.6 These births, when compared with births which occur in hospitals are associated with higher rates of perinatal mortality, postpartum haemorrhage (PPH), neonatal hypothermia, neonatal intensive care admission and occur more commonly in the birth of preterm babies2 9–12 and babies with lower birth weights (−452 g mean weight difference, 95% CI −645 to 260).13 Associated maternal factors with BBA, as compared with babies born in hospital include higher ORs of being multiparous (OR 3.23, 95% CI 1.61 to 6.67),13 with 94.4% being public patients.7 It is also suspected that a proportion of these ‘accidental’ births may be freebirths (an intentional homebirth without a health professional in attendance),14 with transfer to hospital following the birth being due to maternal and/or neonatal complications. There is evidence in the Australian setting that when women are not offered choice in birth settings, they will choose to birth outside of the system.
Aim
The aim of this study was to examine whether the incidence of BBA in New South Wales (NSW) has increased over time, determine demographic and socioeconomic factors associated with BBA; to examine the data for geographical clustering of events and to determine associated maternal and neonatal health outcomes following this occurrence. This study also aims to examine if there is any similarities between geographical areas with higher rates of BBA and higher rates of homebirth that may be freebirths.
Methods
Data sources
A detailed analysis of the Perinatal Data Collection (PDC), the Admitted Patient Data Collection, the NSW Registry of Births, Deaths and Marriages (RBDM) and Australian Bureau of Statistics mortality data (ABS) was undertaken. Pregnancy and birth data for the time period from 1 January 2000 to 31 December 2011 of all births were provided by New South Wales (NSW), Ministry of Health as recorded in the NSW PDC. This population-based surveillance system contains maternal and infant data on all births where babies were >400 g birth weight and/or completed 20 weeks gestation. The NSW PDC contains statistics on all births in NSW, which amounts to one-third of all births which occur in Australia annually. The admitted patient data collection (APDC) is a collection of records of all services to admitted patients provided by NSW public hospitals, public psychiatric hospitals, public multipurpose services, private hospitals and private day procedures centres. The NSW RBDM and ABS contain mortality information for deaths occurring in NSW and Australia. The linked datasets were provided by the NSW Centre for Health Record Linkage (CHeReL) following approval by the data custodian (NSW Health). Probabilistic data linkage techniques were used for these purposes and deidentified datasets were provided for analysis. Probabilistic record linkage software works by assigning a ‘linkage weight’ to pairs of records. For example, records that match perfectly or nearly perfectly on first name, surname, date of birth and address have a high linkage weight, and records that match only on date of birth have a low linkage weight. If the linkage weight is high, it is likely that the records truly match, and if the linkage weight is low, it is likely that the records are not truly a match. This technique has been shown to have a false positive rate of 0.3% of records.15 Socioeconomic factors were determined through the application of the Socio-Economic Indexes for Areas (SEIFA). These indexes are calculated by the ABS16 and are a system whereby geographical areas are mapped according to relative advantage and disadvantage.
Subjects
The variable ‘Place of birth’ on the PDC was used to determine the cohort of women who underwent a BBA in comparison to those who delivered within a hospital or birth centre or had a planned homebirth attended by a health professional. This variable is categorical and other options include hospital theatre/delivery suite, birth centre, planned birth centre/delivery suite, planned home birth, planned homebirth/hospital admission and BBA. Maternal age, parity, postcode, birth details and birth outcomes were obtained from the PDC. Perinatal deaths were calculated from multiple sources but were limited to those that occurred within 28 days of birth and they were only counted once. Death may have been detected on any one of the following four datasets. The PDC ‘Discharge status’ variable or admissions in the APDC where the case mode separation was coded as ‘Died’ or the NSW RBDM or ABS death data where a death had been recorded. The maternal admission data for any admission that occurred during the pregnancy, as well as the birth admission for all cases of stillbirth or neonatal death were examined to determine any maternal medical or pregnancy-related condition. This methodology of using multiple data sources to identify cases has been shown by Lain et al 17 to be the most reliable way to increase ascertainment of cases. For previous delivery events and outcomes, only those cases for multiparous women for whom their previous birth details were in the dataset were included. Analyses of socioeconomic advantage and disadvantage were undertaken using the ABS indices. Missing data ≥5% of any data item for either BBA or non-BBA cohorts will be reported in the results section. One hundred and nine cases (0.01%) where excluded from the cohort where place of birth was not stated.
Data analysis
Demographic data is reported between the comparison groups according to BBA status using χ2 for dichotomous variables and mean or median comparison for continuous data. Missing data at ≥1.0% was reported. Taking into account the size of the cohort and the number of analyses undertaken, results were considered significant at the level p<0.01. Analysis was undertaken with IBM SPSS V.23.
Results
During the time period 2000–2011, there were 1 097 762 births able to be included in this study as recorded in the PDC. Of these, 4945 were recorded as BBA, equating to a rate of 4.6 per 1000 births. For the data items relating to smoking and gestation at booking visit there were significant levels of missing data. For smoking, there was 62.0% in the BBA cohort and 8.8% in the non-BBA cohort. For gestation at booking visit, there was 8.5% and 0.12%, respectively. For all other data items reported in the tables, there was <1.0% missing data in both cohorts. The BBA rate from the first year of the study (2000) when compared with the final year of the study (2011) changed from 4.2 per 1000 births in 2000 (369 births) to 4.8 per 1000 births in 2011 (464 births) (p=0.06). The range of BBA births for each woman was from 1 to 4, although in 95.6% of cases only one birth occurred per woman. The demographics and medical/obstetric history of these women are displayed in table 1.
Demographics and pregnancy/birth events
Maternal and neonatal morbidity and perinatal mortality are displayed in table 2.
Neonatal and maternal outcomes
For multiparous women (4289, 86.7%), previous adverse birth events for those in the dataset (3516, 81.9%) are recorded in table 3.
Previous birth outcomes for multiparous women
Women who had a BBA were most likely to be having their second baby (41.8% of cases) as displayed in figure 1. Women who had a BBA and were multiparous were more likely to have had a vaginal birth for their previous birth (2.1% compared with 21.6%), and were more likely to have had a baby previously who went to special care nursery/neonatal intensive care unit (SCN/NICU) (16.9% compared with 15.5%).

Percentage of BBA events according to maternal parity. BBA, born before arrival.
An analysis of socioeconomic advantage and disadvantage was undertaken according to maternal postcode. When divided into socioeconomic deciles, with 10 being the most affluent, BBA most commonly occurred in women of the lowest decile (no.1) as seen in figures 2 and 3 and homebirth occurred most frequently in decile 10. The median day for admission of the baby following birth was day 0 (the day of birth) occurring in 97.7% of cases with a range between 0 and 23 days of age. The most commonly occurring complications recorded on the neonatal hospital records was suspected infection (6.9%), hypothermia (6.9%), respiratory distress (5.4%), congenital abnormality (4.0%) and neonatal withdrawal symptoms (2.4%).

Index of relative socioeconomic advantage and disadvantage comparing BBA events, non-BBA births and homebirth with trend lines. BBA, born before arrival; SEIFA, Socio-Economic Indexes for Areas.
{kind=link}
{kind=link}
{kind=link}
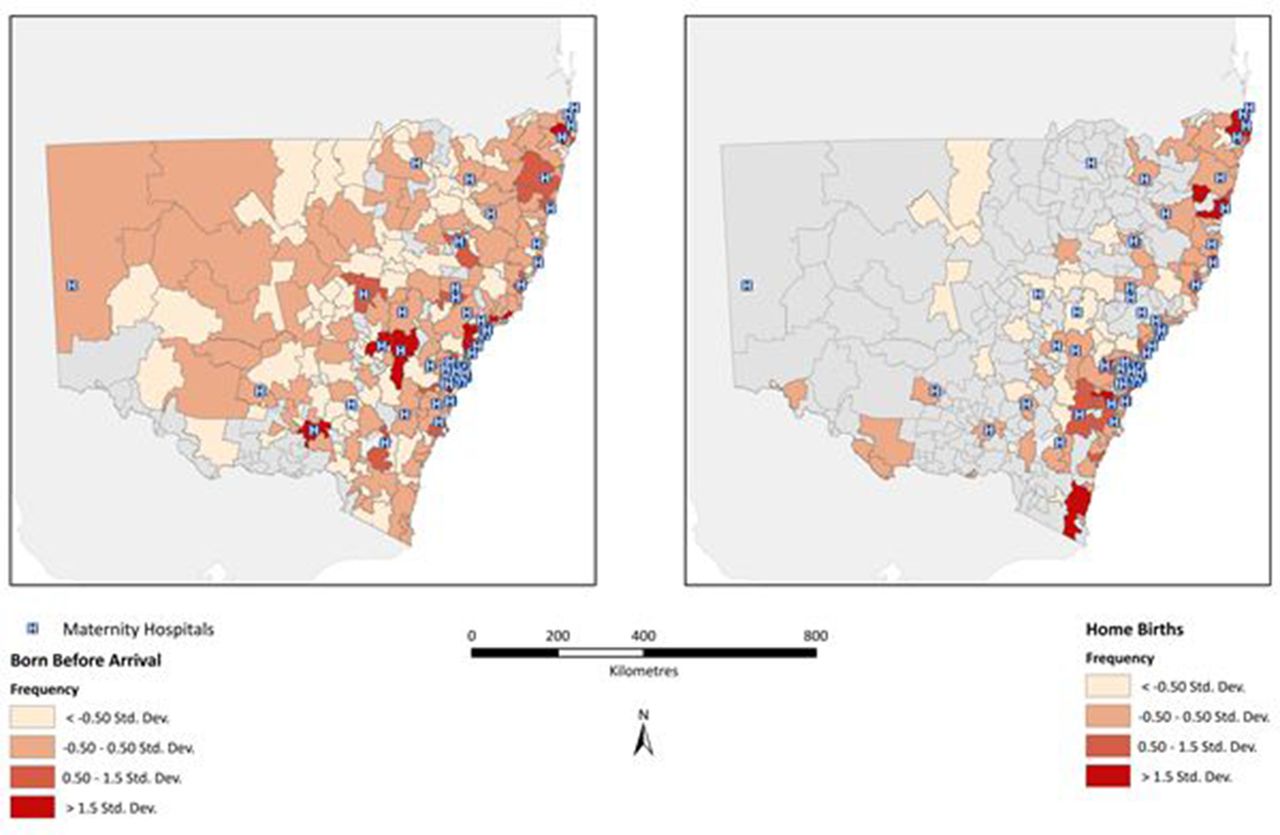
Visual representation of BBA events and homebirth events in NSW. BBA, born before arrival; NSW, New South Wales.
For BBA events which occurred at term a similar difference were seen in regard to maternal profile and outcomes except that the perinatal mortality rate (PMR) was much lower in both groups (6.7/1000 births in the BBA group compared with 2.2/1000 births in the non-BBA group). PPH requiring transfusion was the same in both groups at term (0.7%). These results are displayed in table 4.
Demographic details and outcomes for mothers and babies for BBA at ≥37 weeks gestation
Two hundred and nineteen women had multiple BBA events (table 5). These women were more likely to smoke (46.1%), be Australian born (85.8%) and their babies were more likely to be admitted to SCN/NICU (28.8%) when compared with the non-BBA cohort.
Demographic details and outcomes for mothers and babies for BBA for those women who had multiple BBA events
The illustrated geographical distribution of the incidence of BBA and homebirth is displayed in figure 3. The areas of highest BBA were rural areas, areas of socioeconomic disadvantage and coastal areas. Homebirth occurred at the highest rates in coastal areas and in the Southern Highlands.
Discussion
Neonatal outcomes
We found a higher proportion of adverse outcomes for neonates who were BBA in comparison to neonates born within hospital settings or born at home during a planned homebirth. These include; a higher rate of prematurity (12.5% compared with 7.3%), lower birth weights (3160.6 g compared with 3370.4 g) and a higher rate of admission to a SCN/NICU (20.6% compared with 15.5%). These findings replicated those found in previous studies including the large Finnish population study (>320 000 births).2 The crude PMR OR in this BBA cohort compared with the non-BBA cohort was 3.6 (95% CI 3.07 to 4.14). The adverse event rate decreased significantly when only including women who were term but were still higher than planned hospital/birth centre and homebirth. PMR rates for neonates BBA in the literature are quoted as being 3–11 times higher than the non-BBA.2 8 10
Maternal profile
The maternal profile of higher rates of smoking (30.5% compared with 13.8%), small percentage of private insurance status (5.6% compared with 23.8%) and the overall SEIFA relative indices of socio/economic disadvantage (76.0% of BBA births occurring in postcodes where the indices were in the lowest three deciles) displays a profile of socioeconomic disadvantage among these women. This finding has been shown previously by Unterscheider et al 7 in a large study of >39 000 births in Ireland. This study also found a high rate of smoking among mothers who had a BBA (31%).
Maternal outcomes
Women, who have a BBA, have a significantly increased risk of experiencing a PPH requiring transfusion of (OR 2.2; 95% CI 1.71 to 2.71) compared with the non-BBA cohort. Severe perineal trauma (SPT) was lower in the BBA cohort (0.8% compared with 1.8%). Even when taking into consideration the higher premature rate this finding does support the positive correlation between lower rates of birth intervention and lower rates of SPT found in other studies. Women who give birth in non-medicalised settings such as in birth centres and homebirth have significantly lower SPT.18 19 The lower number of male infants born to mothers who have a BBA may also play a role in this with previous research we have undertaken showing a higher rate of SPT with male infants.20
Gender
The higher rate of girls to boys in this study is also interesting and we have written before about why the birth of a male infant may be more difficult and lead to more birth trauma compared with a female. Male infants have larger head circumferences and wider shoulder diameters.21 22 Shoulder dystocia is higher when the baby is male regardless of birth weight.21 Women carrying male infants are at increased risk of operative deliveries for non-reassuring fetal heart rate during labour and failed instrumental births.23 Other studies have shown more medical complications, such as gestational diabetes, caesarean delivery and meconium stained liquor,24 while others show equivocal outcomes.25 It is possible the smaller size of female infants leads to faster labours and births and hence women are more likely to be caught out in these situations.
Geographical issues
Distance to maternity units is clearly playing a contributing part in the incidence of BBA, with higher rates than average being seen is the least populated regions in NSW, such as the Far West (13.1 per 1000 births). In this area, there are great distances to the maternity unit.1 While other regional areas such as the Snowy Mountains (11.1 per 1000 births) and Central West Slopes (8.9 per 1000 births) are better serviced than the Far West region, but distances between maternity units can still exceed 2 hours by car. The disparities in the geographical distribution of maternity services in Australia have been previously identified showing that they do not meet population need, nor do they factor in population vulnerability or isolation.26 Distance as a contributing factor in the incidence of BBA has been explored previously in Queensland Australia,6 where it was found that the increase in the incidence of BBA in that state was associated with the closure of rural and remote maternity units, thereby increasing the distance women were required to travel to birth. This factor is further supported by the low incidence of BBA within the Sydney region. The lowest eight rates of BBAs (all ≤3 per 1000 births) occurred in the Sydney suburbs which are well supplied with maternity units. Conversely, high rates of BBA are seen in areas of NSW where distance to maternity units is not a mitigating factor, such as the Blue Mountains (9.7 per 1000), Tuggeranong (9.7 per 1000) and Port Stephens (11.6 per 1000). These areas all have maternity units within 1-hour drive. Although Tuggeranong only had a birth rate of 207 births during the time of the study compared with 80 052 births in the Parramatta region of Sydney—the geographical centre of the Sydney region.
Lower indices of maternal socioeconomic status and thereby education levels are associated in our study with a higher incidence of BBA, yet this was not without exceptions. Of the six regions which had the highest rates of BBA, the SEIFA indices were; Far West (2), Port Stephens (4), Snowy Mountains (5), Tuggeranong (9) and the Blue Mountains (7). A range from 2 to 7 (not including the Tuggeranong region which only had 207 births). This clearly supports the argument that there are other forces at play in relation to BBA.
Association between homebirth, BBA and freebirth
There is evidence that areas where homebirth occurs more commonly are also area of high BBA in this study. The Tweed Coast region and the Northern Rivers region have higher rates of homebirth than BBA. The Tweed Coast has a homebirth rate of 8.0 per 1000 births and a BBA rate of 6.4 per 1000 births. The Northern Rivers has a rate of homebirth rate of 7.7 per 1000 births and has a BBA rate of 7.5 per 1000 births. The highest rate of homebirth occurred in the Mid-North Coast region (11.6 per 1000 births) which had a BBA rate of 5.3 per 1000 births. The occurrence of freebirth could be influencing the association between high rates of homebirth and BBA in some regions. The coastal areas of NSW and the Blue Mountains of NSW are known to be areas with higher than state average rates of planned homebirth.1
Homebirth is an option for only a few women in Australia through publicly funded models (11 in total nationwide) and for women who choose to hire a privately practising midwife (around 200 in total). In Australia private models of homebirth remain largely unfunded and uninsured.27 This is out of step with maternity service reforms in comparable countries such as New Zealand, the UK and Canada where home birth is supported as a mainstream option with public funding and affordable insurance available. These factors contribute to the fact that a small number of women (0.3%) choose to have a planned homebirth in Australia.1 Of note is the finding that homebirth occurs more frequently in the most socioeconomically advantaged women in accordance with SEIFA codes of advantage and disadvantage. Freebirth appears to be rising in Australia and currently there are no data available to determine where these births are happening.27 28 We have undertaken research into why women are making this choice and past birth trauma, a distrust of mainstream services and a physiological paradigm around birth tend to be drivers.14 29 30 Evidence from Australian research conducted in the Northern Territory supports the fact that ‘freebirth’ will occur more frequently in indigenous communities where birthing on country options are not provided to women and birth is routinely expected to occur at hospital settings as far away as 500 km from their homes.31 In NSW there is currently no facility within the RBDM for the recording of a freebirth and accurate rates are not able to be determined. It would appear this should be rectified in order to determine changes, trends and service needs for certain populations including women who have multiple BBAs and, therefore, may be in fact free birthing.
Limitations
This study is limited by the lack of maternal body mass index data which would enable further examination of associated factors. These data are not currently obtained in the PDC or the APDC. The addition of the variable regarding indigenous status would have provided greater depth of understanding of the social determinants inherent with the occurrence of BBA. This variable is not one currently available under the ethics approval of this dataset. This study would have been further enhanced by the recording of freebirth within the RBDM as this would enable accurate incidence to be calculated. Further, limitations include the combining of NICU/SCN data in the PDC which may not always be indicative of the degree of neonatal morbidity. As this dataset contains data pertaining to NSW only the generalisability of results may vary across other Australian states where geographical distance between units may be greater. Definitions used within this study are those pertaining to the Australian context and may vary within international settings.
Conclusion
The BBA rate within NSW was 4.6 per 1000 births over the time period and did increase from 4.2 per 1000 births in 2000 to 4.8 per 1000 births in 2011. The great majority of BBAs occur in multiparous women having their second baby. We have identified three potential influencing factors: (1) geographical distance to maternity units, (2) low maternal socioeconomic status and (3) ‘hidden’ freebirths requiring or resulting in transfer to hospital. Factors 1 and 2 are closely related while factor 3 is one that previously may have been overlooked. This knowledge may assist healthcare providers and policy-makers in providing appropriate information and services to childbearing women in NSW. Increased attendance at relevant antenatal education as to the signs of impending birth and the need for a plan with regard to getting to hospital may also help reduce the incidence of BBA. Having functional and affordable homebirth attended by professional midwives could also have a positive impact on the women who are currently freebirthing and may be contributing to these BBA numbers. Finally, there needs to be a recording of freebirths through the births deaths and marriages in order to determine trends and geographical locations where freebirth may be increasing.
Acknowledgments
The authors are grateful to the Centre for Health Data Linkage NSW Health (CHeReL) for their assistance in providing linked population datasets. Ellen Carter Flinders University for her assistance with geo mapping techniques.
References
Footnotes
Contributors CET formulated the study, analysed the data and wrote for publication. HGD formulated the study and wrote for publication.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Ethical approval was obtained from the NSW Population and Health Services Research Ethics Committee, Protocol No.2010/12/291.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We do not have ethics approval to share data.