Article Text

Abstract
Objective To assess patient perspectives on secondary lifestyle modification and knowledge of ‘heart attack’ after percutaneous coronary intervention (PCI) for coronary artery disease (CAD).
Design Observational cross-sectional study.
Setting A single university-based hospital centre in Japan.
Participants In total, 236 consecutive patients with CAD who underwent PCI completed a questionnaire (age, 67.4±10.1 years; women, 14.8%; elective PCI, 75.4%). The survey questionnaire included questions related to confidence levels about (1) lifestyle modification at the time of discharge and (2) appropriate recognition of heart attack symptoms and reactions to these symptoms on a four-point Likert scale (1=not confident to 4=completely confident).
Primary outcome measure The primary outcome assessed was the patients’ confidence level regarding lifestyle modification and the recognition of heart attack symptoms.
Results Overall, patients had a high level of confidence (confident or completely confident,>75%) about smoking cessation, alcohol restriction and medication adherence. However, they had a relatively low level of confidence (<50%) about the maintenance of blood pressure control, healthy diet, body weight and routine exercise (≥3 times/week). After adjustment, male sex (OR 3.61, 95% CI 1.11 to 11.8) and lower educational level (OR 3.25; 95% CI 1.70 to 6.23) were identified as factors associated with lower confidence levels. In terms of confidence in the recognition of heart attack, almost all respondents answered ‘yes’ to the item ‘I should go to the hospital as soon as possible when I have a heart attack’; however, only 28% of the responders were confident in their ability to distinguish between heart attack symptoms and other conditions.
Conclusions There were substantial disparities in the confidence levels associated with lifestyle modification and recognition/response to heart attack. These gaps need to be studied further and disseminated to improve cardiovascular care.
- coronary artery disease
- patient perspective
- confidence
- lifestyle
- patient education
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
To date, many trials have focused on improving clinical outcomes in patients with coronary artery disease via various interventions; however, few studies have investigated the patients’ perspectives, which this survey unveils.
This study enables medical providers to address the needs of the patient through a more comprehensive understanding of the latter’s perspectives, resulting in improvement of clinical outcomes.
This is a small study conducted in a single centre and the data were based on the subjective perceptions of patients.
The cross-sectional design of this study limits its ability to clarify the impact of a patient’s confidence level on their long-term clinical outcome.
Introduction
Lifestyle modifications, including a balanced diet, smoking cessation, limited alcohol consumption and increased physical activity, are recommended for the first-line management for coronary artery disease (CAD). The American Heart Association/American College of Cardiology guidelines recommend a healthy diet with an emphasis on vegetables, fruits and whole grains along with vigorous physical activity (3–4 aerobic sessions per week).1 2 Adhering to lifestyle modifications, including higher quality diets or exercise rehabilitation, has been associated with a lower risk of all-cause mortality among patients with CAD.3 4
The recognition and confidence levels of patients with respect to symptoms and reactions to ‘heart attack’ are also important patient-related factors influencing clinical outcomes. A previous nurse-led study revealed that education and counselling intervention led to increasingly positive attitudes in terms of patient response to heart attack,5 suggesting that knowledge of heart attack could also represent a modifiable factor in the optimisation of CAD management. Furthermore, inappropriate understanding of the symptoms of CAD could directly affect the action of patients in seeking prompt emergency care,6–9 which is known to contribute to timely reperfusion therapy.
In recent years, patient perspectives on lifestyle modification or disease recognition have been the subject of much research in the field of cardiovascular diseases.10 11 Understanding patient perspectives on these modifiable factors is essential to close the perception gap between healthcare providers and patients in terms of patients’ confidence levels regarding lifestyle modification or disease recognition. These approaches could also help to identify imbalances in the composition of patient education programmes and assess the appropriateness of such programmes. In this study, our primary goal was to elucidate the perspectives on secondary lifestyle modification and precise knowledge of heart attack in patients treated with percutaneous coronary intervention (PCI) in Japan.
Methods
Study population and data collection
We performed an observational cross-sectional study. The study population consisted of 237 consecutive patients who underwent PCI between October 2011 and September 2012 at a single university-based hospital centre (Keio University Hospital, Tokyo, Japan). Our nursing team obtained the completed survey questionnaires immediately after a group educational programme and the provision of discharge instructions, which are typically conducted 24–48 hour before discharge. Patient education was conducted by nurses and nutritionists using video and literature materials for lifestyle modification and nutritional guidance, which was followed by face-to-face counselling by a nurse. At this time, the nurses answered several questions related to the survey questionnaire from the patients.
The response rate to the survey questionnaire was 99.6% and we excluded one patient (0.4%) due to missing questionnaire data. Thus, our analysis included a total of 236 patients who answered all the survey questions. Within this final cohort of study patients, 55 patients (23.3%) were diagnosed with acute coronary syndrome (ACS) (ST-elevation myocardial infarction, n=28; non-ST-elevation myocardial infarction and unstable angina, n=27) and 181 patients (76.7%) were diagnosed with stable angina or silent ischaemia. More patients hospitalised for stable angina had a history of previous PCI than those hospitalised for ACS (n=90 (49.7%) vs n=6 (10.9%), P<0.001). All patients provided written informed consent to participate in the study. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki.
Survey questionnaire
The survey included questions covering a wide range of variables (table 1).
Questionnaire for patients treated with percutaneous coronary intervention
The questions were grouped into three domains
usefulness of the hospital educational programme;
self-confidence level in terms of lifestyle modification;
confidence level in terms of the awareness of heart attack.
The questionnaire was originally designed after an in-depth discussion among board-certified cardiologists and nurses at our institute for this study and was largely based on the recommendations of the Japanese Circulation Society (JCS) guidelines.12 We first generated two major domains: (1) lifestyle modification and (2) action and recognition regarding heart attack. The components of lifestyle modification were initially chosen from the JCS guidelines class-I recommendations (plus class IIa if no class-I recommendations were available). The latter questionnaires for action and recognition regarding heart attack were specifically developed by the investigators of the present study. We chose the term ‘heart attack’, which is commonly used in clinical practice, rather than medical jargon (eg, myocardial infarction). This was to help the patients to understand the questionnaire more easily.13 To evaluate and validate the preliminary questionnaire, we then conducted a pilot study with 17 patients (not included in the final analysis). On reviewing the responses to the pilot study, some adjustments were made, including the addition of questions related to the usefulness of our hospital education programme. For domain 1, patients were asked to rate the usefulness of lifestyle and nutrition guidance using a five-point Likert scale (1=never useful, 2=not useful, 3=little useful, 4=useful, 5=very useful or not provided with an educational programme) and patients were divided into the useful group (4 or 5) and not useful group (1, 2 or 3). For domain 2, the questionnaire concerning self-confidence level about lifestyle modification contained 12 questions that were scored based on a four-point Likert scale (1=not confident, 2=less confident, 3=confident, 4=completely confident) and the patients were divided into the high confidence group (3 or 4) and low confidence group (1 or 2). These self-confidence questions consisted of nine behaviour-based confidence levels (drug adherence, alcohol restriction, smoking cessation, exercise >30 min, regular exercise, keeping body weight, keeping blood pressure, avoiding salty food and avoiding fatty food) and three knowledge-based confidence levels (danger of smoking, alcohol, depression/anxiety or insomnia). The sum of each confidence level in the nine behaviour-based questions on lifestyle modification was calculated as the overall confidence level in lifestyle modification and we defined the lower tertile for this overall confidence level as the ‘low confidence group’ and surveyed the characteristics associated with this group. For the final domain (domain 3), patients were asked to rate their recognition and action towards heart attack using a four-point Likert scale.
Statistical analysis
Continuous variables were summarised as means and SD and categorical variables as percentages. Logistic regression analyses were conducted to assess the association of the patients’ confidence in behaviour-based lifestyle modification as well as their precise recognition of heart attack with various patient characteristics. For multivariate analysis, the variables entered in the model included age, male sex, obesity, high school graduation or less, hypertension, diabetes mellitus, dyslipidaemia and previous myocardial infarction (MI) or PCI. Before multiple logistic regression analyses were performed, multicollinearity was assessed and factors indicating serious multicollinearity were accordingly eliminated from the model. C-statistics were used to evaluate the predictability of the models used for multivariate regression analysis. For all statistical analyses, statistical significance was accepted at P<0.05. Data analysis was performed using SPSS V.23.0 for Windows.
Results
Demographic data and usefulness ratings of the educational programme by participants are shown in table 2 (domain 1). Most of the participants were men and approximately half of them had received university education or higher. Approximately, 70% of patients considered their lifestyle modification programme as useful (very useful, 26%; useful, 45%). Nutritional guidance was also considered useful by approximately 70% of the patients (very useful, 28%; useful, 44%).
Demographic data of the study participants
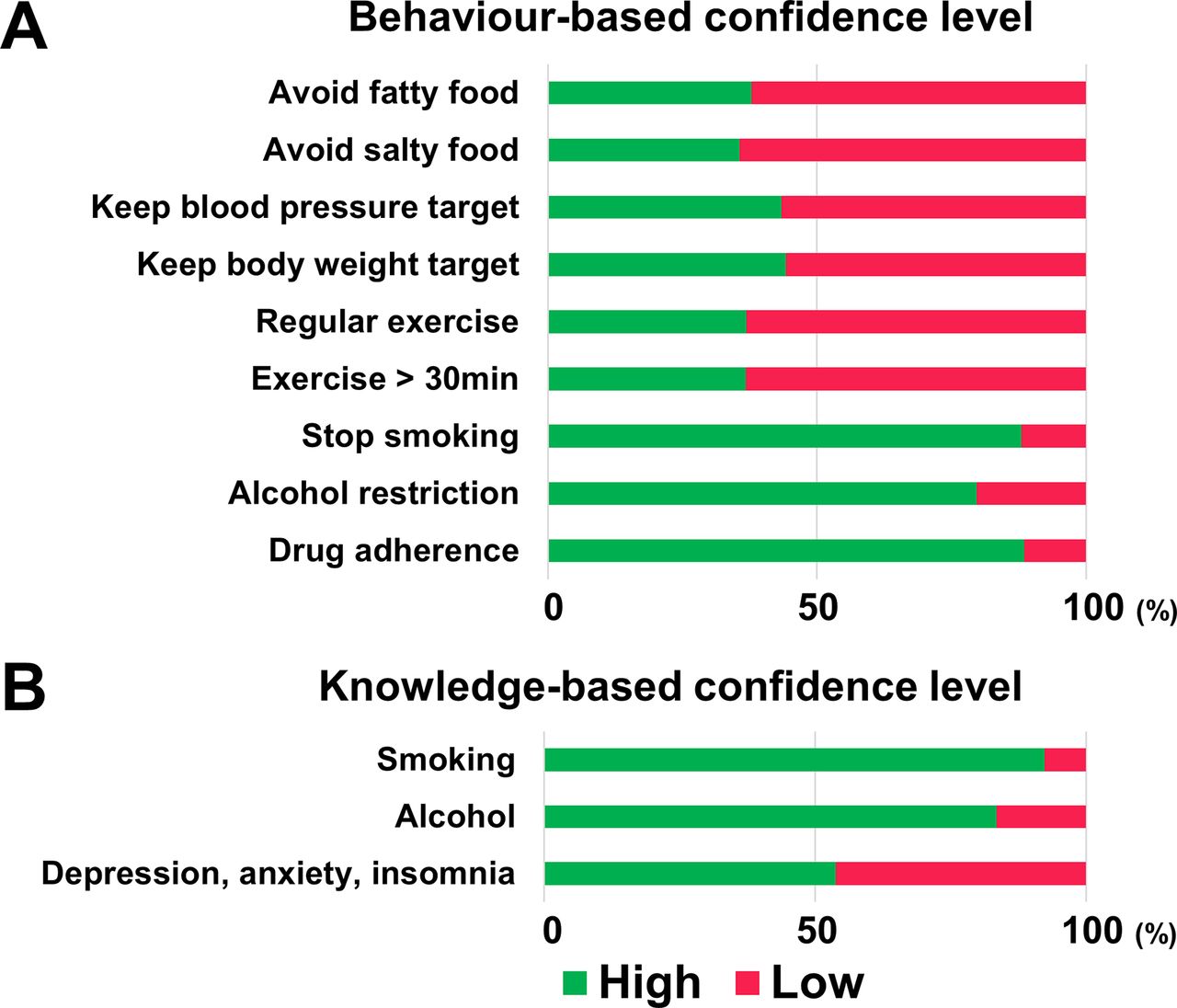
Figure 1 shows the behaviour-based and knowledge-based confidence levels associated with lifestyle modification (domain 2). Most of the participants were highly confident (confident or completely confident, >75%) in smoking cessation, alcohol restriction and adherence to medication. However, they had low levels of confidence (confident or completely confident, <50%) in blood pressure and cholesterol control, diet regulation, body weight maintenance and routine exercise (figure 1A). In terms of knowledge-based confidence level of lifestyle modification, most of the patients were confident in their understanding of the danger of smoking or alcohol but were not confident in their understanding of the risk of depression, anxiety and insomnia (figure 1B).

Self-confidence level regarding lifestyle modification. (A) Behaviour-based and (B) knowledge-based confidence level.
The total confidence score was calculated from the sum of the previously described nine behaviour-based confidence levels in lifestyle modification (maximum score, 36 points). Patients scoring lower than the first tertile for total confidence (<23 points) were defined as the low confidence group. Univariate regression analysis showed that male sex, obesity and lower education level were associated with the low confidence group with respect to lifestyle modification. In multivariate regression analysis adjusted for age, sex, obesity, educational level, coronary risk factors and previous MI or previous PCI, we found that male sex (OR 3.61, 95% CI 1.11 to 11.8) and lower education level (OR 3.25, 95% CI 1.70 to 6.23) were independent determinants of inclusion in the low confidence group (table 3A). The significant association between obesity and low confidence level in lifestyle modification disappeared after adjustment for covariates (OR 1.73, 95% CI 0.90 to 3.33). The C-statistics of models 1 and 2 were 0.72 (95% CI 0.65 to 0.80) and 0.72 (95% CI 0.64 to 0.79), respectively.
Determinants of low confidence level in lifestyle modification
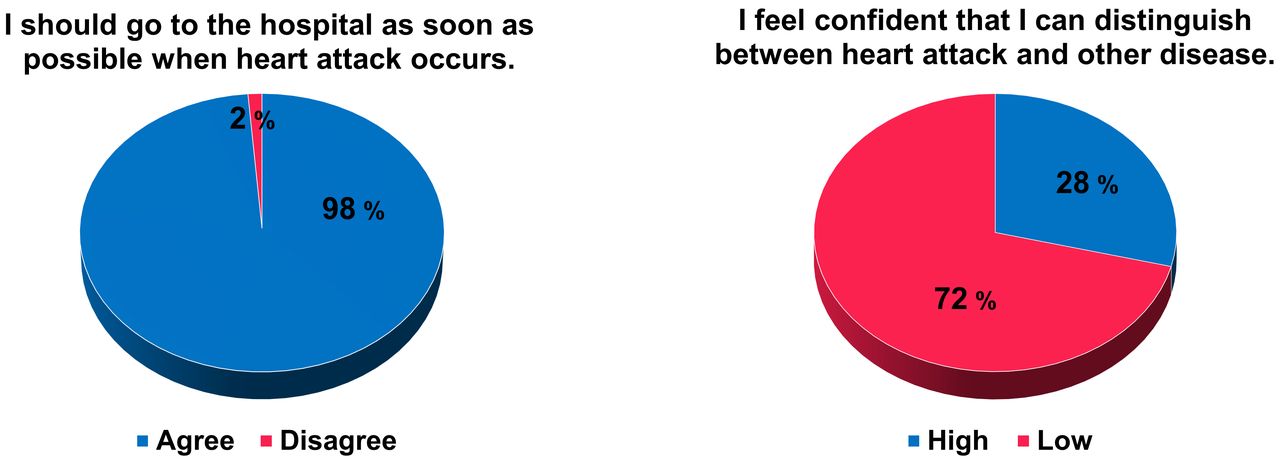
The data concerning patients’ recognition of heart attack are shown in figure 2 (domain 3). When questioned about whether they agreed with the idea of promptly going to the hospital after a heart attack, 233 patients (98%) agreed (completely agree, 50%; agree, 48%), whereas one and two patients disagreed and completely disagreed with the idea, respectively. In contrast, only 28% were confident in distinguishing between heart attack and other diseases (completely confident, 5%; confident, 23%), whereas 100 patients (42%) were less confident and 67 (28%) patients were not confident. Within this domain, univariate logistic regression analysis revealed that patients who had high confidence in their awareness of heart attack were associated with a previous MI or PCI and this association remained significant after adjustment for age, sex and coronary risk factors (previous MI: OR 2.51, 95% CI 1.29 to 4.91; previous PCI: OR 2.04, 95% CI 1.09 to 3.80; table 3B). The C-statistics of models 1 and 2 were 0.67 (CI 0.59 to 0.75) and 0.65 (95% CI 0.57 to 0.73), respectively.
Determinants of high confidence in precise recognition of heart attack

{kind=link}
{kind=link}
Patient’s perception and recognition of heart attack.
Discussion
The present study demonstrated the following key points: (1) confidence levels in lifestyle modification were different across the various risk factors for patients with CAD and patients had low confidence in their blood pressure and cholesterol control, diet regulation, body weight maintenance and routine exercise; (2) low confidence in overall lifestyle modification was associated with male sex and lower education level and (3) there was a substantial gap between recognition of and action towards heart attack.
Much of the existing research on lifestyle modification has focused on single behaviours, for example, smoking cessation. However, the level of accomplishment regarding lifestyle modification can vary among the main modifiable risk factors, including alcohol restriction, dyslipidaemia, obesity, physical inactivity, hypertension and diabetes. The strength of this study is that we quantified patient confidence levels based on patient behaviour towards several risk factors for CAD that could be related to adherence to lifestyle modification. Although patient education is known to be an important intervention in enhancing the adherence to lifestyle modification,14 the challenge is how to effectively deliver education programmes to patients with CAD given limited human resources and limited duration of hospitalisation or outpatient consultation. We demonstrated that patients with CAD were not confident in adhering to regular and sufficient exercise after discharge. The adherence to exercise training has been reported as low in previous studies, that is, approximately <60% in patients with heart failure (HF),15 16 which is consistent with our data. Cardiologists need to emphasise the importance of exercise training and pursue strategies to promote regular exercise, such as more extensive referral for cardiac rehabilitation and structured nurse-led or therapist-led contact.17 Our patients were also less confident about factors related to dietary and nutritional factors. Several previous studies reported poor adherence to salt restriction or diet restriction in general among patients with chronic diseases such as HF or diabetes mellitus,18–20 suggesting that the difficulties in adhering to dietary modification could be universal. Despite its powerful opportunities to reduce adverse health, confusion surrounding nutritional guidance sometimes emerges because of the rapid advances in dietary and nutrition science.21 Continuous education performed by multidisciplinary teams, especially nutritionists and diabetologists, could be essential in improving lifestyle modification.
Knowledge of predisposing risk factors is an important step in the modification of lifestyle behaviours. Our study demonstrated that most responders understood the risk of smoking or excessive alcohol intake and were confident in restricting these activities. This robust patient knowledge was most likely due to repeated public health promotion, leading to patient motivation to adhere to smoking cessation and alcohol restriction with relative ease.22 23 In fact, the prevalence of smoking and alcohol consumption in Japan has declined during the last 10 years.24 25 Considering these results, the importance of promoting smoking cessation and alcohol restriction through educational programmes might be low relative to several other modifiable risk factors. However, psychological and sleep disturbances are known to be under-recognised and under-treated in patients with cardiovascular disease despite their significance in the development and progression of various cardiovascular conditions, including CAD.26 27 In parallel with these circumstances, patient knowledge relating to depression, anxiety and insomnia as risk factors for CAD was relatively poor in our study population. Educational campaigns directed at cardiologists and patients are needed to improve awareness of psychological and sleep disturbances as risk factors for CAD.
Several studies have been conducted to clarify sex differences in the achievement of the secondary prevention of cardiovascular disease, with mixed and inconsistent results.28–30 Interestingly, there were regional variations in the sex differences in the achievement of lifestyle modification.31 32 Although lifestyle modification for the secondary prevention of CAD is generally worse in women than in men, women in Asia are more likely than men to be adherent to lifestyle modification, especially in terms of adequate physical activity, with opposite results in Europe and the Middle East.32 Consistent with these regional variations, patient perspectives concerning secondary prevention could differ. While our study revealed that the male sex was associated with low confidence in lifestyle modification for CAD in Japan, a nationwide survey from the USA demonstrated that women have less knowledge and awareness of cardiovascular disease than men.33 Although it remains unknown why regional variations occur in the sex differences in the attitude towards and achievement of lifestyle modification, this might be explained by the social background of women (eg, education level).34 These assessments are warranted to clarify which subpopulations should be targeted for education in each region. Moreover, regular surveys of patients’ perspectives will also be needed in the future.
It is common for patients to have limited knowledge of heart attack symptoms. The lack of awareness in this regard represents a significant barrier to patients taking action and seeking medical care.6 In our study, most of the participants had low confidence in distinguishing between heart attack and other diseases. Patients with a history of MI or PCI were relatively confident in their ability to precisely recognise a heart attack, possibly because of their previous experience of heart attack, PCI, or exposure to repeated education. It is difficult to conclude which factors affect the confidence level concerning heart attack from our data; however, education focusing on heart attack in patients with CAD without previous MI or PCI is recommended.
The present study has some limitations that should be considered when interpreting the results. First, this was a small study based on data from a single centre. Therefore, the study involved a small number of patients. No formal power analysis of the results of the pilot study to determine the optimal sample size was performed. Consequently, its statistical power may not have been sufficient to detect any negative outcomes. Second, the cross-sectional design of this study limits its ability to clarify the impact of a patient’s confidence level on lifestyle modification and awareness of heart attack on postdischarge behaviours and long-term clinical outcomes. Third, our study population included only patients who underwent PCI. Thus, patients who were not eligible for coronary revascularisation were excluded, which could have caused potential selection bias. Finally, our data were based on subjective patient perceptions rather than objective evaluations. Thus, the confidence levels are subject to individual bias.
Conclusions
There were substantial disparities in the confidence level concerning lifestyle modification and awareness of heart attack in patients treated with PCI. Male sex and lower educational level were associated with lower confidence levels concerning lifestyle modification. There was a substantial gap between recognition of and action towards heart attack. A history of MI and PCI were associated with higher confidence in the awareness of heart attack. Medical providers should bring these disparities to light with the aim to solve them with help of a multidisciplinary team to improve overall cardiovascular care.
References
Footnotes
Contributors HK and TK had full access to all data and were responsible for the integrity and accuracy of data analysis. HK, TK and SK were responsible for the study design and drafting of the manuscript. HK, TK, JF, NN and RF were involved in the acquisition and analysis of data. HK, TK, SK, SY and YM did the interpretation of data. SY, YM and KF critically revised the manuscript for intellectual content.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was approved by the Keio University School of Medicine Ethics Committee (approval no. 20110263).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The dataset analysed during this study are available from the corresponding author (TK, kohno.a2@keio.jp) on reasonable request.