Article Text

Abstract
Objective The aim of this study was to systematically review the literature to identify whether obesity or the regular practice of physical activity are predictors of clinical outcomes in patients undergoing elective hip and knee arthroplasty due to osteoarthritis.
Design Systematic review and meta-analysis.
Data source and eligibility criteria A systematic search was performed on the Medline, CINAHL, EMBASE and Web of Science electronic databases. Longitudinal cohort studies were included in the review. To be included, studies needed to have assessed the association between obesity or physical activity participation measured at baseline and clinical outcomes (ie, pain, disability and adverse events) following hip or knee arthroplasty.
Data extraction Two independent reviewers extracted data on pain, disability, quality of life, obesity, physical activity and any postsurgical complications.
Results 62 full papers were included in this systematic review. From these, 31 were included in the meta-analyses. Our meta-analysis showed that compared to obese participants, non-obese participants report less pain at both short term (standardised mean difference (SMD) −0.43; 95% CI −0.67 to −0.19; P<0.001) and long term post-surgery (SMD −0.36; 95% CI −0.47 to −0.24; P<0.001), as well as less disability at long term post-surgery (SMD −0.32; 95% CI −0.36 to −0.28; P<0.001). They also report fewer postsurgical complications at short term (OR 0.48; 95% CI 0.25 to 0.91; P<0.001) and long term (OR 0.55; 95% CI 0.41 to 0.74; P<0.001) along with less postsurgical infections after hip arthroplasty (OR 0.33; 95% CI 0.18 to 0.59; P<0.001), and knee arthroplasty (OR 0.42; 95% CI 0.23 to 0.78; P=0.006).
Conclusions Presurgical obesity is associated with worse clinical outcomes of hip or knee arthroplasty in terms of pain, disability and complications in patients with osteoarthritis. No impact of physical activity participation has been observed.
PROSPERO registration number CRD42016032711.
- rheumatology
- hip
- knee
- surgical pathology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
The current review is the most comprehensive systematic review on the topic to date.
The current review is the first review to use a quantitative approach to synthesise the results of pain, disability and surgical complications between non-obese and obese participants who underwent hip or knee arthroplasty due to osteoarthritis.
The methodological quality of the included studies was in general poor.
There was a substantial variability of follow-up duration across studies, ranging from 2 weeks to 11 years.
Introduction
Musculoskeletal pain, including pain from knee and hip osteoarthritis (OA), is the leading cause of physical disability in the world and responsible for an increasing burden to patients and society.1 This problem will increase over time, as the world population ages and physical disability resulting from declining health becomes increasingly prevalent.2 The global healthcare expenditure for knee and hip OA is substantial, and most of these costs are incurred by surgical management and associated hospital care.3 For instance, in the UK, the direct costs of OA were estimated at more than £1 billion in 2010, of which £850 million was spent just on surgical procedures.4
Although management of the early stages of this condition consists of a combination of non-pharmacological and pharmacological therapies (eg, anti-inflammatory and analgesic drugs), surgery has become the most common treatment option for severe cases, especially when non-surgical therapies fail to provide sufficient pain relief.5 Osteotomy, mosaicplasty and arthroplasty are some of the existing types of surgery used to manage OA of the hip and knee; with total or partial arthroplasty being the most commonly recommended.6
There are multiple risk factors for the development of knee OA. Among the most common of these are increased body weight and muscle weakness; often attributed to a sedentary lifestyle.7 Obesity and sedentary lifestyle behaviour have also been associated with serious health conditions such as: coronary heart disease, type 2 diabetes, breast and colon cancers and decreased life expectancy.8 Although there is evidence for the role of obesity and physical inactivity in health conditions and quality of life in general,9 10 the actual impact of these factors, together or in isolation, on the outcomes of elective surgery of the knee and hip is still controversial.11 12 Although previous attempts to systematically review the literature have been made, these studies13–15 have either failed to perform a quantitative summary of the evidence (ie, meta-analysis), have excluded patients undergoing knee arthroplasty16 or have excluded pain outcomes.13 No meta-analyses have been performed considering obesity and physical activity as predictors of surgical outcomes in terms of pain, disability, quality of life and complications after hip or knee arthroplasty for end-stage OA.
Identifying whether obesity and physical activity participation predict surgical outcomes in patients with knee and hip OA will inform clinical practice in terms of prognosis and safety of an increasingly prevalent treatment approach. We have conducted a meta-analysis of cohort studies aiming to quantify the role of obesity and physical activity participation as predictors of clinical outcomes in terms of pain, disability, quality of life and postsurgical complications. This review and meta-analysis focused on patients with knee and hip OA undergoing hip or knee arthroplasty.
Methods
Data sources and searches
We conducted a systematic review following the PRISMA statement.17 This review was prospectively registered on PROSPERO, registration number CRD42016032711. A systematic electronic search was performed in the following databases from inception to January 2017: MEDLINE, EMBASE, CINAHL and Web of Science. We used a combination of relevant keywords to construct the search strategy including obesity, physical activity, knee OA, hip OA, arthroplasty and elective surgery (online supplementary appendix 1). The first screening of potentially relevant records was conducted by one author (DP) based on titles and abstract, and two authors (DP and GCM) independently performed the final selection of included trials based on full-text evaluation. A third reviewer arbitrated in case of disagreement (MLF). Moreover, the reference lists of included studies were checked for potential studies. An additional 26 references were screened, but none met our inclusion criteria. No restriction was applied on language.
Supplementary file 1
Study selection
We included only longitudinal studies assessing the role of obesity or physical activity participation on the clinical outcomes following partial or total hip arthroplasty (THA) or partial or total knee arthroplasty (TKA) surgery. Clinical outcomes were defined in terms of pain, disability, quality of life and complications after arthroplasty. To be eligible, studies had to be full reports; include participants who underwent elective arthroplasty of the hip or knee due to OA; include data of presurgical and at least one postsurgical assessment of the clinical outcomes of interest; and assess the association between the predictors and outcomes of interest. Obesity and physical activity participation had to be assessed at baseline. Studies on revision surgery were excluded. Studies were not excluded based on intensity or duration of symptoms.
Data extraction
Using a standardised form, data on study characteristics, predictors and outcome measures of interest were independently extracted from the included studies by two reviewers (DP and GCM). A third author (MLF) resolved any disagreement. Estimates of association between predictors and outcomes of interest were extracted as presented in each study and included ORs, risk ratios (RR), correlations, mean differences (MD) or regression coefficients. When studies reported more than one tool regarding the same topic (eg, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Hip Disability and Osteoarthritis Outcome Score (HOOS), Oxford Hip Score (OHS), Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Society Score (KSS)), estimates were extracted from the group with the largest sample size.
We contacted the authors to provide further information when there were insufficient data reported in the manuscript. When authors were unavailable we estimated data using the recommendations in the Cochrane Handbook for Systematic Reviews of Interventions.18
Outcome measures
Data on pain intensity were extracted as visual analogue scale scores ranging from 0 to 10 and measured directly or as part of the following measurement tools: the WOMAC, the HOOS, the KOOS or the Harris Hip Score (HHS). If studies reported more than one measure of pain intensity or disability for the cohort, the most severe measure at baseline was included in the pooled analyses. Disability measures included the OHS ranging from 12 to 60, with 12 being the best result; Oxford Knee Score ranging from 0 to 60, with 60 being the best result; the HHS ranging from 0 to 100, with 100 being the best result; KSS ranging from 0 to 100, with 100 being the best result; WOMAC total score ranging from 0 to 96, with 0 being the best result; or WOMAC function subscale ranging from 0 to 10, with 10 being the best result; and were converted into a uniform 0–100 scale where 0 meant less disability. Extracted data on complications included any descriptive measure of the number of complications or number of patients with a complication reported during the study. Only two of the screened studies had reported specific raw data on quality of life among the participants after joint arthroplasty, but due to differences in follow-up length, any meta-analysis made by merging these data would result in an unreliable measure.
Methodological quality assessment
The methodological quality of included studies was assessed by two independent reviewers using the Newcastle-Ottawa Scale (NOS)19 recommended by the Cochrane Collaboration.18 The NOS consists of eight items grouped into three categories, namely: selection, comparability and outcome. A star system, ranging from zero to nine stars, is used to classify the quality of the study being reviewed (the more stars the study receives in each category, the higher its methodological quality). After the independent assessment of included studies by the leading author, each study received the following categorical scores representing its quality: good (three or four stars in selection domain AND one or two stars in comparability domain AND two or three stars in outcome domain), fair (two stars in selection domain AND one or two stars in comparability domain AND two or three stars in outcome domain) or poor (zero or one star in selection domain OR zero star in comparability domain OR zero or one star in outcome domain). A third reviewer (MLF) resolved any disagreement between independent assessors. Methodological quality scores for included studies are presented in table 1.
Data analysis
Data on baseline (ie, presurgical scores) and postoperative outcome scores were weighed by the inverse study variance and used in fractional polynomial regression modelling to build graphs depicting the course of pain and disability over time. STATA V.14 was used for the analyses (StataCorp, College Station, TX).20
Meta-analyses were performed to assess the differences in pain, disability and complications after surgery, between predictor groups (ie, obese and non-obese groups as defined by included studies), using a random effects model. When possible, different analyses were performed for knee and hip arthroplasty and also for different levels of obesity (ie, obesity and morbid obesity). When means and SD of outcomes of interest were presented for multiple predictor groups in the same study (ie, underweight (body mass index (BMI)<18), normal weight (BMI≥18<25), overweight (BMI≥25<30) and obese level I (BMI≥30<35), II (BMI≥35<40) or III (BMI≥40)) these were combined into two groups (non-obese: BMI<30 and obese: BMI≥30) as recommended in the Cochrane Handbook for Systematic Reviews of Interventions18 before inclusion in the pooled analyses. Results were reported as standardised mean differences (SMD) and 95% CIs. Between-study heterogeneity was calculated using I2 (I2<25%: small heterogeneity; 25%<I2<75%: moderate heterogeneity; I2>75%: large heterogeneity).21 We have defined an SMD of 0.2 as small difference, 0.5 as moderate difference and 0.8 as large difference.22
Assessment of publication bias was performed using funnel plots. The precision (ie, SE) of included studies was plotted against the difference in outcomes between groups (ie, obese or non-obese) and results visually analysed. In the absence of publication bias or small study bias, smaller studies should be evenly spread around the base of the funnel, while the larger studies should be concentrated around the top of the funnel. Plot asymmetry was also quantified using the Egger’s tests, for which a null hypothesis represents symmetry of plotted data.23
All meta-analyses were conducted using Comprehensive Meta-Analysis software (Comprehensive Meta-Analysis, Englewood, NJ). For studies not reporting enough data to be included in the meta-analyses, the reported individual associations were tabulated and qualitatively presented in tables 2–5.
Results
Our search strategy identified 11 990 studies. After removing 381 duplicates, 11 221 studies were screened and excluded based on keywords, titles and abstracts. All the remaining 388 studies were written in English and were assessed by reading the full text, of which 326 were then excluded, yielding 62 studies to be included in the systematic review.24–85 From these, 31 presented enough data to be included in at least one of the meta-analyses (figure 1).

Flow chart of search strategy and screening steps. Detailed steps of references screening process of results from database searches.
Included studies
Included studies reported data from 18 different countries: Australia,40 47 72 85 Canada,38 43 78 China,84 Denmark,60 England,27 30 Finland,49–52 France,65 73 Germany,55 75 81 Italy,28 29 Japan,83 Netherlands,57 76 Norway,45 Scotland,25 36 South Korea,56 Spain,41 80 Switzerland,61 62 69 UK26 35 37 46 48 53 63 67 68 71 74 and USA.24 31–34 39 42 44 54 58 59 64 66 70 77 79 82 Demographic data from each study are presented in table 1.
Included studies and characteristics
Methodological quality
An overall quality assessment of the studies showed that 50% (n=31) of the included studies were considered as being of good methodological quality, while 1.5% (n=1) were considered fair and 48.5% (n=30) were considered of poor methodological quality. Of the screened studies, 56 (90%) had a follow-up rate of 80% or greater, and only half (n=32 studies) assessed outcomes via retrospective analysis of medical records, conducted adjustment for potential confounders (eg, age or sex) or investigated a representative sample of the population (online supplementary appendix 2).
Supplementary file 2
Assessment of publication bias
Inspection of funnel plots and results of Egger’s test confirmed no evidence of small study bias for those studies included in our pooled analyses, with P values ranging from 0.07 to 0.43 (online supplementary appendices 3–5).
The course of pain and disability over time
The fractional polynomial regression model resulted in a pooled mean disability score and SD before hip arthroplasty of 59.42 (SD: 10.94; n=5250). At 12 months after surgery it had decreased to a mean of 31.31 (SD: 24.28; n=3017) and a further reduction was observed at 120 months, when the mean disability score after hip arthroplasty was 24.32 (SD: 19.53; n=210). For knee OA, a pooled mean disability score of 56.88 (SD: 10.74; n=17 225) was observed for patients undergoing arthroplasty. At 12 months after surgery this value decreased to 21.80 (SD: 13.51; n=2898), while at the 110-month follow-up, the mean disability score was 14.18 (SD: 0.77; n=485). The pooled mean pain score before hip arthroplasty was 54.86 (SD: 10.20; n=2517), decreasing to 13.76 (SD: 1.32; n=1058) 3 months after surgery, 10.8 (SD: 1.69; n=1212) at 6 months and slightly increasing to 13.45 (SD: 7.87; n=2173) at the 12-month follow-up. For patients undergoing knee arthroplasty, the pooled pain score at baseline was 57.78 (SD: 9.28; n=2211), which decreased to 25.67 (SD: 6.61; n=1222) at 6 months, and 14.18 (SD: 0.77; n=1820) at the 12-month follow-up (figure 2).

Fractional polynomial analysis for hip (A) and knee (B) disability scores and hip (C) and knee (D) pain scores over time. (A) Graphic representation of results from fractional polynomial analysis of disability scores evolution over time after hip surgeries. (B) Graphic representation of results from fractional polynomial analysis of disability scores evolution over time after knee surgeries. (C) Graphic representation of results from fractional polynomial analysis of pain scores evolution over time after hip surgeries. (D) Graphic representation of results from fractional polynomial analysis of pain scores evolution over time after knee surgeries.
Association between obesity and postsurgical pain outcomes
Fourteen studies investigated the association between obesity and pain intensity in a total of 5687 patients after hip or knee arthroplasty. Seven of the 14 studies presented enough data to be pooled in a meta-analysis. There was an overall moderate and statistically significant difference in postsurgical pain between obese and non-obese patients after arthroplasty, with non-obese patients having better outcomes at short-term timepoint (SMD −0.44; 95% CI −0.68 to −0.20; P<0.001) and long-term timepoint (SMD −0.36; 95% CI −0.47 to −0.25; P<0.001). The pooled results for separate joints suggest non-obese participants have significantly less short-term (ie, less than 6 months) postsurgical knee pain, compared with obese participants (SMD −0.55; 95% CI −0.90 to −0.20; P=0.002) and postsurgical hip pain (SMD −0.34; 95% CI −0.67 to −0.02; P=0.039). Obesity was defined as having a BMI over 30 kg/m2. At long term (ie, 6 months or longer), there was a significant moderate difference between obese and non-obese groups in terms of knee pain (SMD −0.36; 95% CI −0.48 to −0.25; P<0.001); however, there was no difference between groups for hip pain (SMD −0.32; 95% CI −0.84 to 0.20; P=0.222) (figure 3). The results of individual studies not included in the pooled analyses are presented in table 2.

Pooled standardised mean difference (SMD) in pain at short term and long term after surgery between obese and non-obese patients. Results from meta-analysis of included studies presented as SMD of pain scores at short-term (<6 months) and long-term (≥6 months) follow-ups between non-obese and obese groups.
Results of individual studies on the association between postsurgical pain and baseline obesity
Association between obesity and postsurgical disability outcomes
The impact of obesity on disability was investigated by 32 studies which compared postsurgery disability scores in 35 286 obese and non-obese participants. Of these, 19 studies presented complete data that were included in the pooled analysis. At short term, no statistically significant difference in overall disability between obese and non-obese participants was observed (SMD −0.16; 95% CI −0.42 to 0.10; P=0.231). Likewise, no statistically significant difference was observed between obese and non-obese participants for postsurgical knee or hip disability (SMD −0.42; 95% CI −1.0 to 0.16; P=0.159 and SMD −0.09; 95% CI −0.39 to 0.20; P=0.527, respectively).
At long-term follow-up, however, there was an overall moderate and statistically significant difference in postsurgical disability between obese and non-obese patients regardless of the joint affected (SMD −0.32; 95% CI −0.37 to −0.28; P<0.001). That difference was still statistically significant and of moderate magnitude when knee and hip joints were analysed separately (SMD −0.32; 95% CI −0.37 to −0.27; P<0.001 and SMD −0.35; 95% CI −0.44 to −0.26; P<0.001, respectively, and favouring non-obese patients) (figure 4). The results of individual studies not included in the pooled analyses are presented in table 3.

Pooled standardised mean difference (SMD) in disability at short term and long term after surgery between obese and non-obese patients. Results from meta-analysis of included studies presented as SMD of disability scores at short-term (<6 months) and long-term (≥6 months) follow-ups between non-obese and obese groups.
Results of individual studies on the association between postsurgical disability and baseline obesity
Association between obesity and postsurgical complications
The association between obesity and complications after joint arthroplasty was assessed by 40 studies including a total of 245 433 patients who underwent knee or hip arthroplasty. Of these, 17 presented enough data and were included in the meta-analyses.
The pooled results suggest that at short-term follow-up, non-obese participants are less likely to have postsurgical deep vein thrombosis (DVT) (OR 0.49; 95% CI 0.26 to 0.91; P=0.024) when compared with obese participants (figure 5). A total of 13 studies were pooled (n=22 782) showing non-obese patients are also less likely to present any long-term (ie, ≥6 months) dislocation (OR 0.50; 95% CI 0.31 to 0.80; P=0.003) and DVT (OR 0.58; 95% CI 0.36 to 0.94; P=0.043). A non-significant difference between groups was observed between non-obese and obese participants for long-term revision surgery (OR 0.66; 95% CI 0.34 to 1.28; P=0.217) (figure 5).

Pooled association between complications and obesity at short-term and long-term follow-ups. Results from meta-analysis of included studies presented as incidence of complications at short-term (<6 months) and long-term (≥6 months) follow-ups between non-obese and obese groups. DVT, deep vein thrombosis.
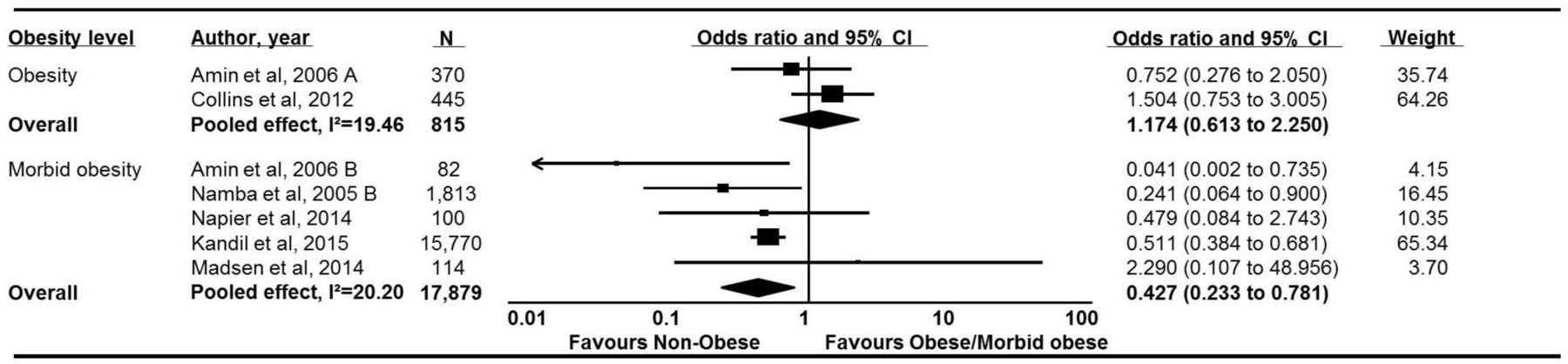
The pooled analysis on short-term postsurgical infection for hip replacement showed that non-obese patients are less likely to develop infections compared with obese participants (OR 0.33; 95% CI 0.19 to 0.59; P<0.001) (figure 6). For knee replacement, separate analyses were conducted for studies comparing obese with non-obese participants and those comparing morbidly obese with non-obese participants (figure 7). The results suggest that non-obese patients are less likely to develop infections when compared with morbidly obese patients (OR 0.43; 95% CI 0.23 to 0.78; P=0.006). No association with postsurgical infection was observed when obese and non-obese participants were compared.

Pooled association between postsurgical infections and obesity for hip surgery. Results from meta-analysis of included studies presented as incidence of infections after hip surgery between non-obese and obese groups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pooled association of postsurgical infections for knee surgery. Results from meta-analysis of included studies presented as incidence of infections after hip surgery comparing the non-obese group with obese group and the non-obese group with morbidly obese group.
The overall pooled analysis for incidence of complications suggests that non-obese participants are less likely to present any postsurgical complication at the long-term follow-up (OR 0.56; 95% CI 0.42 to 0.75; P<0.001, respectively). The results of individual studies not included in the pooled analyses are presented in table 4.
Results of individual studies investigating the association between obesity and postsurgical complications
Association between physical activity participation and disability
The association between physical activity and disability was investigated by four studies73 75 76 79 or 1033 participants undergoing hip or knee arthroplasty. Included studies have not provided enough data to be pooled. The overall results from these four papers suggest that participants who practise more physical activity before the surgeries were more likely to experience less pain after either hip or knee surgery; however, the evidence regarding disability scores is still unclear with studies presenting contradictory results. Table 5 presents the results of the individual studies.
Individual results on the association between physical activity and pain or disability
Discussion
Statement of principal findings
Our results suggest that following surgery, non-obese patients experience further reductions in both pain and disability after knee and hip arthroplasty when compared with obese patients, where obesity has been defined as having a BMI of 30 kg/m2 or over. These differences seemed to be more accentuated for knee pain outcomes following arthroplasty than for hip pain or disability outcomes. Non-obese participants also experienced significantly less postsurgical complications, including dislocation, DVT and infection especially following hip arthroplasty. Our analyses also demonstrate that obesity is a reliable predictor of complications after THA and TKA, in the short term after the procedure and at longer follow-ups. The evidence regarding preoperative physical activity remains unclear due to conflicting results of included studies, especially in terms of postoperative disability. The four included cohort studies, however, suggest that physical activity participation is associated with better pain outcomes following surgery.
Our results from the fractional polynomial analysis have also shown that all patients experienced an improvement in pain and disability after surgery. We also highlight that although non-obese patients experience further improvements in pain and disability compared with obese participants, both groups improved significantly following surgery as depicted in figure 2. The observed decrease in pain from baseline was approximately 70% at 6 months and 75% at 12 months, with decreases in disability of 55% at 12 months and 67% at 120 months. The interpretation of the postsurgical course of pain and disability, however, needs to be taken in the context of the inclusion criteria we have used in our review, given we have only included data from cohort studies that have assessed the role of obesity or physical activity participation on surgical outcomes.
Strengths and weaknesses in relation to other studies, discussing particularly any differences in results
Our meta-analysis results regarding the association between obesity and postsurgical complications found that obese patients present higher complication rates than non-obese patients. These results are consistent with the findings of previous systematic reviews of Hofstede et al,14 Samson et al 15 and Liu et al.16 Our meta-analysis results regarding the association between obesity and postsurgery disability also agreed with the findings of Buirs et al 13 and Samson et al,15 which found that obesity (defined as having BMI over 30 kg/m2) was associated with worst postsurgical functional score. The only previous review which has performed a meta-analysis on the association between obesity and postarthroplasty pain or disability limited its inclusion criteria to hip joint.16 That review included a total of 15 studies in their meta-analysis and found that obesity increases the risk of postsurgical complications (RR 1.68; 95% CI 1.23 to 2.30; P=0.0004) and is associated with worse disability scores following surgery (MD −2.75; 95% CI −4.77 to −0.6; P=0.07). Our study has included 33 cohorts of hip arthroplasty participants in the qualitative analysis, 16 in the meta-analyses, and confirms past findings that obesity is associated with worse outcomes in terms of disability and complications, and pain at both short-term and long-term periods following surgery. Hofstede et al 14 have also conducted a systematic review of the literature on preoperative predictors of surgical outcomes after hip replacement in patients with OA. Although those authors included 35 studies, only five studies investigated the effect of obesity on postsurgical pain, disability and quality of life.14 No meta-analysis was performed.
Implications for clinicians or policymakers
Our results have a direct impact on clinical practice as the results demonstrate that obese patients have a higher risk of complications and a poorer prognosis in terms of pain and disability postoperatively when compared with non-obese patients. These results also allude to the importance of identifying and implementing effective presurgical rehabilitation and weight loss approaches to optimise postsurgical outcomes and minimise harm to the patient. The importance of weight loss has been highlighted in international clinical guidelines on non-surgical management of knee OA, for instance, given the pain and disability reductions observed following weight loss regimes.86 Past research also suggests there is a dose–response relationship between weight loss and clinical outcome improvement. A recent completer-type analysis of 1383 participants with knee OA showed that a weight loss of 7.7% of body weight or more is associated with clinically important changes in pain and disability, as measured using the Knee Injury and Osteoarthritis Outcome Score (KOOS).87 This evidence reinforces the importance of presurgical weight loss programmes and strategies in order to optimise postsurgical recovery.
Strengths and weaknesses of the study
The current review has included 62 cohort studies and a total of 256 481 participants and is the most comprehensive systematic review on the topic to date. It is also the first review to use a quantitative approach to synthesise the results of pain, disability and surgical complications between non-obese and obese participants and consider the physical activity level of participants who underwent hip or knee arthroplasty due to OA. Our review has some limitations. The methodological quality of the included studies was in general poor. The most common methodological flaw among included cohorts was not controlling for confounding factors age, sex or BMI (32 studies, 51%) followed by not using a representative sample (n=30 studies, 48%). Moreover, we have observed great variability of follow-up duration across studies, ranging from 2 weeks to 11 years. We have used a cut-off of 6 months to define short-term follow-up (ie, <6 months) or long-term follow-up (ie, ≥6 months), but acknowledge that within each follow-up category there was substantial variation in the duration of follow-up across studies.
Between-study heterogeneity has also been observed in some of the pooled analysis for obesity presented in this review. A potential source of between-study heterogeneity includes the variability in the definition of obesity categories across studies. Although obesity was assessed using BMI scores in all studies, some studies have used only two obesity groups (ie, obese or non-obese) while others used several categories including underweight, normal or overweight, obese and morbidly obese. These needed to be combined for some of our pooled analyses.
Another potential source of between-study heterogeneity across is the difference in surgical procedures used across studies. For instance, in the pooled analysis of risk of postsurgical DVT and obesity, while Kandil et al 54 performed unicompartmental knee arthroplasties, Friedman et al 42 performed total arthroplasties on both hip and knee joints. That discrepancy might explain the different results reported by these two studies (figure 5). Likewise, the mean physical activity load reported by the included studies varied substantially, ranging from low to high frequency of participation in low and high-impact activities. This should be taken into consideration when interpreting the physical activity results.
Conclusion
Our results have shown that obese patients undergoing hip or knee arthroplasty due to OA have worse outcomes in terms of pain and complications when compared with non-obese patients, with differences more accentuated for patients with knee OA. Likewise, obese patients will have worse surgical outcomes in terms of disability, but only at long-term follow-ups. It is still unclear whether presurgical physical activity participation has an impact on surgical outcomes. However, we acknowledge that the health benefits of physical activity participation for patients with knee and hip OA are multiple and reach beyond those considered in this review.
Supplementary file 3
Supplementary file 4
Supplementary file 5
Acknowledgments
The authors would like to acknowledge the participation of Ms Giovana Visentini in the independent methodological quality assessment of the included studies.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
Footnotes
Contributors DP, GCM, PHF, FMB and MLF were involved in the conception and design of the review. DP, GCM and MLF developed the search strategy and performed study selection. DP and GCM extracted data from included studies. DP assessed the methodological quality of included studies. DP and MLF were involved in the data analysis. DP, GCM, PHF, FMB and MLF were involved in the interpretation and discussion of results. DP drafted the manuscript, and GCM, PHF, FMB and MLF contributed to the drafting of the review. GCM, PHF, FMB and MLF revised it critically for important intellectual content. All authors approved the final version of the article. All authors had access to all of the data in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis. Theauthors would like to acknowledge the participation of Ms Giovana Visentini inthe independent methodological quality assessment of the included studies.
Funding This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. This work was carried out with CNPq support, National Council for Scientific and Technological Development–Brazil. DP holds the Science Without Borders Scholarship from the Brazilian Government. MLF holds a Sydney Medical Foundation Fellowship and a National Health and Medical Research Council/Australia Fellowship.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data extracted from papers and used to write this paper are available to whoever ask. Contact the corresponding author for further information.
Presented at The abstract of this work has been published in the conference proceedings of the 2017 Osteoarthritis Research Society International.