Article Text

Abstract
Introduction The aim of this review is to answer the following question: Does assistive technology contribute to social inclusion for people with intellectual disability? Previous research on assistive technology has focused on socioeconomic impacts such as education, employment and access to healthcare by people with intellectual disability. There is a need to consolidate evidence on the interaction between intellectual disability, assistive technology, community living and social inclusion.
Methods and analysis The review will consider studies from all settings: geographical, socioeconomic and care (institutional and community care), published in English. Studies reported in other languages with abstracts in English will be included if they can be translated using Google Translate, otherwise such studies will be included in the appendix. The review will include both qualitative and quantitative studies. The intervention in this review refers to the use of assistive technology to promote community participation or interpersonal relationships (social inclusion) for people with intellectual disability. The outcomes will be behavioural and social benefits of using assistive technology by people with intellectual disability. Enhanced interpersonal relationships and community participation by people with intellectual disability. Data analysis will be in two phases. The first phase will involve analysis of individual study designs separately. The second phase will be narrative/thematic synthesis of all study groups.
Ethics The review will not create any ethical or safety concerns.
Dissemination At least one peer-reviewed article in a leading journal such as the BMJ is planned. The findings will also be disseminated through a seminar session involving internal audience at Trinity College Dublin and within the Assistive Technologies for people with Intellectual Disability and Autism research programme.
PROSPERO registration number CRD42017065447; Pre-results.
- assistive technology
- social inclusion
- intellectual disability
- interpersonal relationships
- community participation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- assistive technology
- social inclusion
- intellectual disability
- interpersonal relationships
- community participation
Strengths and limitations of this study
The eligibility criteria for the review are broad and exhaustive hence the review will consolidate the best available evidence on how assistive technology can support social inclusion for people with intellectual disability.
The use of social inclusion model (by Simplican et al) to assess reported social inclusion outcomes may exclude some relevant studies that do not report on the outcomes stipulated by the chosen model.
The review may overlook significant contributions from non-English language publications because only papers published in English will be included.
Introduction
Community living by people with intellectual disability
Intellectual disability (ID) in this protocol refers to an individual’s reduced ability to comprehend new or complex information, and to learn and apply new skills, beginning before the individual’s 18th birthday (ie, before adulthood). ID interacts with environmental factors to impact on an individual’s ability to independently cope with daily life circumstances,1 resulting in a lifelong need for care and/or support.
Individuals with ID are increasingly becoming part of community processes; living and accessing services in the community. In many countries, they are gradually being relocated from institutional care into community settings.2 3 The drive to relocate people with ID to community-based care settings, herein called deinstitutionalisation or decongregation of care, has been a policy priority for more than three decades in countries such as Australia, the UK, the USA and the Scandinavian nations.4 It is ongoing in other countries such as Ireland, Germany and Spain,5 6 where more people with ID are now living in community settings. Significant political and financial commitment to deinstitutionalisation of care has led to a noticeable decline in numbers of people in large institutional care facilities7 in countries like Ireland. This has involved closure of these larger facilities and relocating people with ID to small-scale community-based care, in some cases congregated care on a smaller scale.8
The national policy contexts highlighted above reflects international undertakings such as the Universal Declaration of Human Rights9 and the United Nations Convention on the Rights of Persons with Disabilities (CRPD).10 For example, Article 19 of the CRPD advocates for community living for people with disability. The ratification and subsequent implementation of such international guidelines underpins the individual countries’ drive for normalisation.11 By March 2017, there were 172 ratifications/accessions and 160 countries were signatories to the Convention,12 making it the world’s most-ratified human rights treaty.13 The CRPD states that people with all types of disabilities must enjoy all human rights and fundamental freedoms; everyone with a disability should have equal access to societal processes such as education, employment, housing and socialisation. Article 19 of the Convention emphasises the right to community living by all people with disabilities and a right to appropriate support to ensure inclusion.6 The current global development agenda through the Sustainable Development Goals,14 calls for no-one to be left behind; a call for inclusion of all, including people with ID. People with ID are the focus of this review because they are one of the groups most vulnerable to social exclusion.15
The global push for greater social inclusion of people with disabilities is taking place at a time of great technological advances. This presents an opportunity to enhance the envisaged community living and social inclusion of people with ID in practices already proven.16 17 It is also an opportunity to explore new approaches facilitated by these rapid technological advances. This review will examine the evidence of how assistive technology (AT), which draws on advances in technology, can enhance community living and social inclusion of people with ID. There is a need for concerted efforts to ensure that people with ID become part of community processes, and for members of such communities to also perceive people with ID as part of their own community. Unless community living for people with ID is enhanced by all means possible, including technological opportunities, there is a risk of ‘redistributing’ institutional isolation to the community rather than progressing genuine social inclusion into the community. Without technology that promotes access, connectivity and community participation, people with ID may not access services in the community like people without disability. This could lead to loneliness3 and dependence on care provided in devolved institutions.
Social inclusion
Cobigo and Stuart18 have noted that the benefits of the shift towards a rights-based approach to care, that should accompany deinstitutionalisation of care for people with ID, have not been achieved. People with ID still encounter stigmatisation, discrimination and rejection due to a variety of factors. For example, feelings or experiences of inclusion or exclusion are dependent on demographic characteristics, such as age, gender and environmental factors; older adults with mild ID, for instance, are more likely to report stigma than younger people.19 As Cobigo et al 20 observed, social inclusion is a product of complex interactions between environmental factors and the opportunities and personal competencies of an individual. The International Classification of Functioning, Disability and Health outlines the importance of recognising the interaction of environmental factors as a key requirement for understanding functioning and disability.21 Social inclusion is a multidimensional, dynamic relational process,22 which is not about assimilation (enabling people to fit into existing societal parameters23 such as being housed in the community), but rather is about self-determination.24 Combating exclusion involves mitigating disadvantages, whereas facilitating inclusion is about actively creating opportunities.
The role of socioeconomic factors such as education,25 employment26 27 and care28 29 on social inclusion are well documented. Social aspects such as interpersonal friendships and sharing of existing resources, as well as active determination of an individual’s or a marginalised group’s life chances, are also crucial.22 Thus as a two-way process social inclusion of people with ID should involve all stakeholders, including people with ID themselves and the general community.3
It has been argued that individuals make meaning of their life through a symbolic interactionism30; presenting an image of themselves which they believe their audience would approve of and accept.31 People with ID may feel part of the community based on how they think others around them perceive them and how much they are able to participate in community processes in terms of their experiences. This depends on what they make of the people they interact with, or are supposed to integrate with, in a community setting. On the other hand, people in the community are likely to accept or reject new members with ID from institutional settings depending on their personal attitudes towards people with ID.32
This review seeks to summarise the literature on how AT can facilitate the social inclusion of people with ID by focusing on the three broad tenets key to effective social inclusion: interpersonal relationships, community and policy.33 With regards to policy, a recent study in Ireland involving people with ID34 found that the participants felt left out of policy processes. There is a need for people with ID to be involved in the entire policy process.3 Including marginalised groups in processes that aim to promote their inclusion, both in policy and in practice, is of paramount importance.35 36
People with ID should also be involved in all initiatives aimed at improving their inclusion into the community through greater self-determination.24 But as Linehan et al 7 pointed out, although social inclusion is the key pillar of disability policies, vagueness about the meaning of the concept persists. This in itself is an obstacle to achieving the social inclusion goals33 of the United Nations CRPD and the Sustainable Development Goals. Different terms such as integration, participation and belonging3 20 are used interchangeably to imply social inclusion. This creates obstacles to inclusion such as communication challenges between different stakeholders. Simplican et al 33 proposed a general definition that could serve as a common meaning of social inclusion and possibly lead to standardisation of research and service provision,33 by enabling all relevant actors to imply a common goal and focus on this.
The working definition of social inclusion used in this review is therefore drawn from the work of Simplican et al,33 who define social inclusion as the interaction between interpersonal relationships and community participation. Simplican and colleagues reviewed literature on social inclusion and found that most research into social inclusion focused on interpersonal relationships or community participation, even though the wording used to express these concepts varied across different studies. Our review will use the social inclusion model (figure 1) proposed by Simplican et al 33 to evaluate how AT affects the various components of interpersonal relationships and community participation as umbrella themes of social inclusion.
Social inclusion model.33
The outcomes of social inclusion to be reviewed will be informed by Simplican et al’s33 ecological pathway, which views disability and social inclusion as products of sophisticated interactions between environmental factors, personal competencies and capability, as well as opportunities available to the individual.20 The ecological variables outlined in figure 2 33 individual, interpersonal, organisational and sociopolitical factors—influence social inclusion both positively and negatively. The present review will therefore look at how AT mediates or moderates,37 the effects of these broad variables on social inclusion of people with ID. Different outcomes of social inclusion will thus be evaluated as outlined in figure 2 and further discussed in the methodology section. The aim is to explore how the new way of conceptualising social inclusion proposed by Simplican et al 33 can be used to capture a more holistic understanding of social inclusion outcomes beyond the more-often reported socioeconomic outcomes such as integration, education38 and access to services.24 The ecological model was deemed relevant because it shifts conceptualisation of social inclusion beyond acceptance and performance of dominant societal values.20 It isolates the definition of social inclusion from the processes that lead to social inclusion and the resulting subjective feelings from social inclusion. Using this model, both positive and negative outcomes of social inclusion33 will be considered. Other potential alternative models may not be relevant for the present review because they focus on specific aspects of social inclusion such as recreation39 or positive relationships.40 We will explore the different levels and types of social inclusion indicators illustrated in figure 2.

Ecological pathway to and from social inclusion by Simplican et al.33 ID, intellectual disability.
Assistive technology
Just like social inclusion, AT implies different things to different people.41–44 AT may refer to the use of various technological resources to support people with different disabilities to obtain behavioural and social benefits and to reduce the negative impact of their disabilities on their well-being and community participation.45 AT may also refer to a wide spectrum of devices, technological aids, strategies, services and practices whose main objective is to improve the quality of life of people with disabilities.46 Irrespective of what the concept may mean to different people, AT can improve functioning and independence of people with disability, thereby promoting their well-being.42
AT in the context of this review refers to any product or service that can be used by a person with a disability to overcome challenges they may face in carrying out daily activities of their choice that would otherwise be limited by their disability. AT will also be understood through the broad classification offered by the International Organization for Standardization (ISO 999:2011 standards).44 ISO’s classification of AT is a useful benchmark because it is internationally recognised and used in many international systems including the European Assistive Technology Information Network (EASTIN). Thus, AT will be understood as a continuum of technological solutions.47 AT includes services and environmental adaptations through inclusive design.48 AT, in this review, is inclusive of mainstream technologies as well as those developed specifically for people with disability.49 50 AT encompasses what may be considered as normal technological solutions for the general population, such as Skype, pill organisers, wheelchairs, Twitter or Facebook, but we acknowledge that most of these solutions remain largely inaccessible to most people with ID. Furthermore, it could be argued that applications such as Skype do not qualify as AT because they do not constitute provision of immediate functionality for the person with ID.41 There is evidence suggesting that many people with ID desire to use mainstream social media, as distinct from some type of specially protected (restricted) platform.51 However, a recent systematic review on the use of social media by people with ID found that safeguarding concerns, literacy and communication challenges, cyber etiquette, cyber language and problems with accessibility such as inappropriate equipment were preventing people with ID from effectively using social media.52
Enhancing social inclusion using appropriate AT
Previous research has shown that effective use of appropriate AT can contribute to the ongoing deinstitutionalisation of care for people with ID, because they can enhance their independence and community participation by reducing the need for formal support services and long-term care.53 AT can transform what would otherwise be community care into community living (see figure 3) for people with ID.54

Framework for at enhanced social inclusion for people with ID.54 ID, intellectual disability.
However, the full potential of AT to enhance the social inclusion and well-being of people with ID is yet to be realised, despite years of evidence supporting such potential.16 17 25 55 By 2017, only about 10% of all people who require AT had access,56 57 implying that access to AT is still very low. In fact, the proportion of people with ID without access to AT is unknown.58 The extent to which social exclusion has been solved for the 10% with access to AT is also unknown. Furthermore, too much focus on AT may divert attention away from other barriers to social inclusion, which may need addressing on their own, or indeed as part of the context of AT. AT could also pose unintended risks to people with ID, thereby, hindering progress towards their social inclusion. For example, the use of digital AT may create risks such as confidentiality concerns or cyberbullying.59 The focus on AT should not compromise the overall quality of life of people with ID and their social inclusion goals.60
There is a need to review literature on how access to and use of AT supports social inclusion. As illustrated in figure 3, Owuor et al 54 pointed out that inadequate access to AT can disempower people with ID, hindering their capacity to participate in community processes and to form and maintain meaningful interpersonal relationships. The framework provides a simplified way of visualising how access to AT directly impacts on the inclusion–exclusion pathway. One possible cause of this lag between demand and supply could be the lack of consensus on the meaning of AT. The policy context in many settings also remain unclear,61 with most of the existing policies on AT positioning AT as an add-on to their main foci.41 Lack of consensus of the meaning of AT49 and how they should be provided, and to whom, makes it difficult to effectively evaluate the use of AT for social inclusion of people with ID. Access to AT does not eliminate the many barriers to social inclusion which vary with socioeconomic differences within and between countries. Furthermore, people with ID compared with the general population are highly vulnerable to multiple comorbidities.62 Thus access to and use of AT may minimise people’s risk of exclusion by moderating the impacts of their comorbidities as well as mediate their social inclusion.37 For example, a digital glucometer can support social inclusion of an individual with ID and diabetes by moderating their blood sugar.
Apart from the needs of the users, environmental factors are key determinants of effective use of AT. The current review will explore the reported barriers and facilitators to adoption and use of AT as well as how the use of AT can enhance the adaptation of the people with ID to their environment or adaptation of the environment to facilitate autonomy of people with ID. Some of the environmental factors to be explored in the review include social support, friendships, access to services, physical environment and availability of AT. The literature63 suggests that these may be key determinants of effective use of AT. The resultant information could be useful in informing the design and provision of AT, provide insights into facilitators or barriers to adoption of AT and inform policy and practice on environmental considerations for successful provision of AT. This knowledge, from other countries with diverse socioeconomic compositions and varying levels of access to AT, may also be useful for the potential scalability and sustainability of AT provision and use among people with ID in high income countries such as Ireland.
Justification
As far as we are aware, this will be the first review of literature focusing on the role of AT for advancing social inclusion for people with ID. We expect to identify important knowledge gaps on the supportive role of AT for social inclusion, building on previous (although limited) research which has focused on socioeconomic aspects of social inclusion, such as education,25 employment26 and access to healthcare28 for people with ID. There is a need to understand best practices for consolidating the interaction between ID, AT, community living and social inclusion. The ecosystem model of social inclusion proposed by Simplican et al 33 offers a framework for reflecting these interactions.
Aim and objectives
The broad question to be answered by consolidating evidence through the proposed review is: Does access to and use of AT promote the social inclusion of users with ID?
Methods
Eligibility criteria
The criteria outlined below will be used to select studies for inclusion in the proposed review.
Study designs
Both qualitative and quantitative studies.
Case studies. This will include blog posts, biographies and newspapers articles focusing on individual users of AT with ID.
Case control studies.
Observational studies.
Cross-sectional studies.
Longitudinal studies.
All forms of randomised trial.
Also to be included are:
studies that look at the use of AT to overcome stigma and low expectations that people with ID experience from their neighbours, professionals and general society as part of the wider social inclusion;
studies that consider other conceptual areas that are manifest of social inclusion such as education, employment and independent living.
The authors will also consider the fact that limited research into the role of AT in social inclusion may necessitate the inclusion of descriptive reports which may not necessarily meet the quality standards that can be effectively assessed using tools such as Critical Appraisal Skills Programme (CASP). Furthermore, most studies tend to focus on technology rather than the individual,64 a source of social exclusion, hence user voices are likely to be omitted in many studies: The present review will include non-peer-reviewed/published material such as blogs and other relevant grey literature. Although formal guidelines on undertaking a systematic review provide essential knowledge standards, they may lead to exclusion of vital knowledge sources which illuminate the topic area reviewed but do not qualify as rigorous publications. The review will also provide a platform for relevant AT user experts to inform the review. There is a need to enhance inclusion of people with ID by going beyond the expectations of a standard review protocol, to include the views of people with ID in a review focusing on their social inclusion.
Participants
All studies that focus on ID will be considered for inclusion. Studies that focus on participants with autism or other disabilities but without a link to ID, and studies that do not explore the link between AT and social inclusion of people with ID, will be excluded.
Assistive technology
AT in this review will encompass a wide range of solutions accessed and/or used by people with ID from diverse backgrounds. These solutions will include AT used for communication, mobility, personal safety, education, job performance, environmental adaptations and cognitive functions among others. In addition, they will comprise what may be considered mainstream technologies, technologies designed for people with disability, as well as technology adapted to suit the needs of people with disability. AT means different things to different people and different terminologies such as assistive products, aids or assistive devices are used to refer to AT. There are many types and forms of AT that are used to enhance the lives of people with ID. The types of AT to be included in the current review will thus be dependent on those reported in the literature retrieved.
Our selection for inclusion will be informed by a general definition of AT as any product, solution or service that can be used by or for persons with disability to overcome challenges they may face in carrying out daily activities of their choice that would otherwise be limited by their personal or environmental factors, but not necessarily due to their ID.
Intervention
As outlined above, the intervention in this review is access to and use of AT for promoting social inclusion or for enabling functional or behavioural accomplishments that lead to social inclusion for people with ID (community participation or interpersonal relationships). Our focus will be on the use of AT in a very broad sense, with a focus on social inclusion of people with ID. These will include, for example, studies exploring the role of information and communication technology on social inclusion of people with ID or studies exploring the role of inclusive design in social inclusion of people with ID.
Comparators
For studies that explore different interventions, at least one of them must be AT. The review will also explore the type of ID reported in the studies we retrieve to compare an outcome of AT in relation to this variable. For those studies comparing different groups of participants, at least one group should be people with ID (mild, medium, severe or profound) for the study to be included in our review. Additionally, we will also look for studies comparing settings (low, middle or high income settings or urban/rural comparisons)
Outcomes
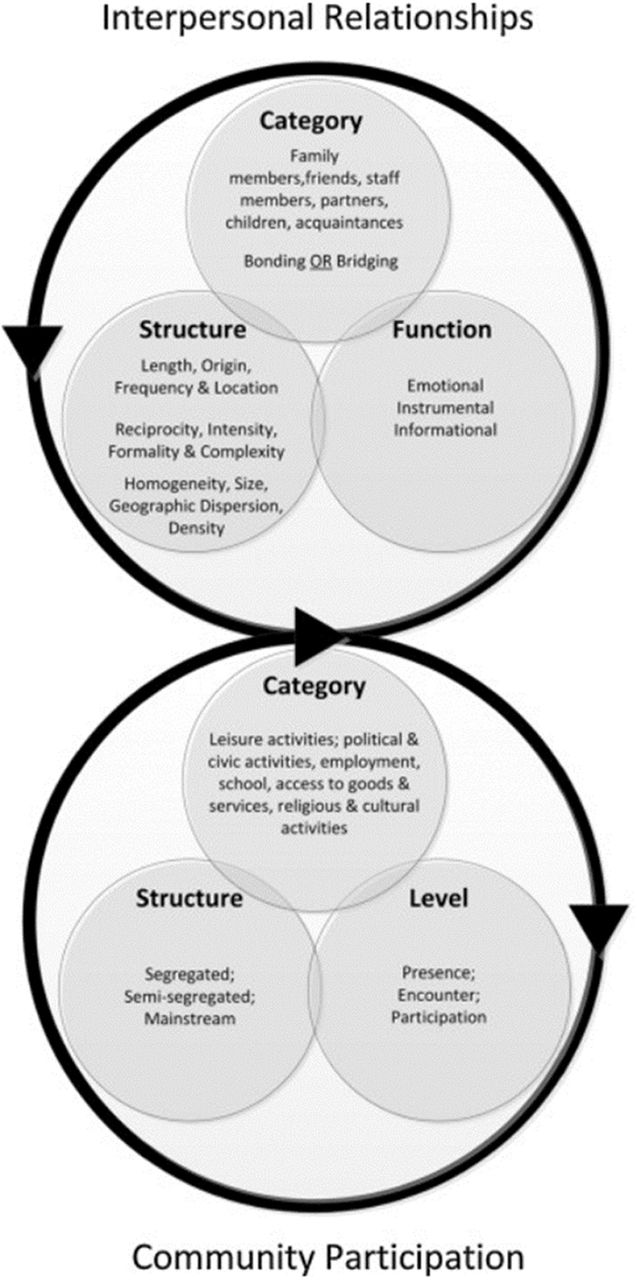
To assess social inclusion outcomes, such as behavioural and social benefits of using AT reported by the relevant studies, we will use the social inclusion model proposed by Simplican et al.33 This model looks at social inclusion from the interpersonal relationship and community participation domains, as illustrated in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Illustrating Simplican et al’s ecosystem social inclusion continuum.33
We will include any study that reports on the following:
Interpersonal relationships
Category: we will look at the people in the social network of a person with ID such as family members, friends, key workers/carers, acquaintances or intimate relationships. The focus here will be on how AT facilitates bonding (relationships between people with shared commonality) and bridging (bringing people with diverse background and experience together).65
Structure: we will explore studies reporting on interpersonal relationships that focus on issues, like the length of the relationships, location of social interactions and frequency of contacts. We will look for studies reporting on how AT can enhance reciprocity, intensity formality and complexity of interpersonal relationships. We will also consider studies investigating social networks in four broad dimensions: size, homogeneity, geographical location and density.
Function: we will therefore include studies that explore how AT enhances functional value of interpersonal relationships; emotional, informational and instrumental.
Community participation
We will consider studies reporting on three different aspects of community participation:
Category: those reporting on the types of community activities such as leisure, hobbies, civic activities, productive activities such as employment and education, consumption activities such as access to goods and services and religion and cultural activities and groups.
Structure: this review is done in the context of ongoing deinstitutionalisation of care for people with ID in many high-income nations such as Ireland, Germany and Spain. The review will provide evidence that can inform deinstitutionalisation practice and policy in these countries. In other high income countries, such as the USA and UK, deinstitutionalisation of care for people with ID is a long-established standard of care and may facilitate the use of evidence. In many low-income countries, institutionalised care has never been a standard care practice for people with ID and the evidence from this review may at least initiate the debate about the need to improve access to and use of AT. The review will evaluate papers reporting how AT affects the engagement of people with ID in community activities in independent community living, semi-independent community living and smaller institutional care in community settings. It is also important to cyber community settings in the review.
Level of involvement: we acknowledge that people generally have different levels of involvement in their communities which can be categorised as encounter, participation or presence. We will therefore review literature that reports on how AT facilitates different levels of involvement by people with ID.
We will also look for papers that report on a mixture of components of the two broad domains outlined above (interpersonal relationships and community participation), because in real life the two domains interact with each other.
Date range
We will include all studies carried out between 2006 and 2017; 2006 was chosen as the start date as it was the year when the CRPD was internationally adopted. This review will explore the potential impact of access to and use of AT for social inclusion of people with ID in the context of the global focus on the CRPD. Although the CRPD has not been ratified in countries such as Ireland, its principles are bound to impact on AT and social inclusion policies and practice. We will also include studies in press.
Language
We will retrieve studies reported in English. We will also include, as appendices, any papers which meet the inclusion criteria and are published in other languages. However, they should have abstracts or titles in English in order to be considered. We will include such studies with English abstracts into the analysis if they can be easily translated into English using Google Translate. Studies with English headings or abstracts, but that cannot be translated into English, will remain as appendices.
Setting
Studies from all settings, geographical and socioeconomic, will be included in the study. However, as studies published in languages other than English from non-English speaking countries will be excluded, such settings may be excluded based on language restriction.
Information sources
Different terms that are used to refer to AT, ID and social inclusion will be used to construct the search strategy. As outlined in the background, all three key concepts (AT, ID and social inclusion) can imply different meanings to different authors. Medical Subject Headings and other controlled vocabularies used by the different databases will be used, through thesaurus searches, to develop a comprehensive search strategy.
The following data sources will be used and more will be included through citation tracking as data is retrieved: MEDLINE, ERIC, PsycINFO, AMED, CINAHL, Scopus, Academic Search Complete, Web of Science, ASSIA, the Cochrane CENTRAL Register and the Campbell Collaboration Register. Prospective registers of research (review and trials registers) and institutional/organisational databases such as that of the WHO will also be searched. The authors will manually search the websites of various organisations with a stake in AT and blogs by expert users of AT with ID. Such organisations include the EASTIN, the Assistive Technology Industry Association, the British Assistive Technology Association, the Academic Network of European Disability Experts, Enable Ireland, Disability Federation Ireland, the Association for Advancement of Assistive Technology in Europe, OpenGrey, GreySource, the Grey Literature Report and many others. We will also search for publications from government or statutory departments and non-governmental organisations. All the literature will be restricted to English as outlined above, with a focus on AT, ID and social inclusion.
The reference lists of all articles retrieved for full text screening will be reviewed to check if there are any relevant sources that were not retrieved by the primary search. ‘Author tracking’ will also be carried out to find out if all the work of the authors whose work meet the inclusion criteria are captured through the prior electronic searches. Time permitting, we will share the list of the final articles for inclusion within the Global Cooperation on Assistive Technology (GATE) and Assistive Technologies for people with Intellectual Disability and Autism (ASSISTID)/Daughters of Charity-Technology Research into Disability Research Institute networks and with other experts in the field of ID and social inclusion or AT and ID.
Search strategy
All peer-reviewed studies as well as publicly accessible reports and PhD theses will be searched using keyword searches in the relevant databases. The keywords around which comprehensive search will be developed are social inclusion, AT and ID. The initial search strategies are attached as an online supplementary file. The final search strategy, to be developed with support from systematic review experts and information specialists, will be reviewed and approved by the project team and an expert in systematic reviews. The search strategies will be revised, if necessary, to include any subject heading or free text terms found in eligible articles.
Supplementary file 1
We will also hand-search individual journals from which at least two relevant studies have been selected for inclusion in the review, to check for other relevant articles that might have been missed, for example, due to the date of journal coverage in the databases. As well as checking the references of the included articles,66 we will also check for any relevant articles citing the selected studies, to try to identify additional relevant material.
Data management
JO and GF will independently search and retrieve all relevant data using the search terms and the final search strategy to be developed. All retrieved data will be imported into EndNote software for deduplication. JO will then export the data to the Covidence application for screening at title/abstract level and subsequent full text screening, risk of bias assessment and data extraction. JO will carry out data screening in Covidence. Some of the key information to be considered for data screening and extraction includes the citation in full, participants’ demographics (age, gender, ethnicity, socioeconomic status, level of ID etc), study setting (country, locality and urban/rural), study method, duration of intervention, type of intervention (assistive technology) and study quality.
Quality and risk of bias appraisal
We will use CASP tools67 as a basis to assess the quality of the literature retrieved. When appropriate, we will adapt the tools to fit our needs. Depending on the studies retrieved, a Mixed Methods Appraisal Tool68 may be used to assess the methodology of the studies. Content from theses, conferences presentations, blog posts, biographies and newspapers articles, if included in the final sample, will be assessed on an individual basis using, for example, audience measurement.68 All these rankings will be relative to the subject area of the source. The team will decide on the most appropriate tools to use for each type of study when the potentially eligible studies have been identified. JO will then rate the retrieved papers separately and compare the rankings with BK. FL will cross-check any differences between JO and BK’s assessments, to facilitate consensus.
Data selection
JO and GF will apply the inclusion criteria and search strategy outlined above, with data exported to Covidence for screening. Other members of the team will cross-check the data retrieved to ensure reliability and validity of the data retrieval and screening process. After the initial screening by JO at title/abstract level is complete, eligible full text articles will be shared with the rest of the team to review. Any articles that seem relevant but lacking some key information during full text screening will be complemented by seeking clarification from the authors. We will contact authors of the identified missing data by email; use of email has been shown to result in timely responses by the relevant authors when the requests are clear.69 Any lack of consensus between the authors during the data screening process will be resolved through deliberations and coming to a consensus on whether to include the paper in question. JO will document this process.
Data analyses
We will analyse studies depending on the methodology used for the study. For example, we will analyse qualitative studies separately from quantitative studies, survey studies, in-depth interview studies, quantitative group design versus single subject quantitative designs. After the separate analyses, a narrative or thematic synthesis will be done for each group of studies, and develop an overall theme from the review.
Subgroups analyses
We will carry out overall data analyses to explore the emerging themes and the findings will determine the ultimate categorisation. The following examples are some of the common categories reported in the literature:
Intellectual disability: low, medium, severe or profound.
Gender: males and females.
Geographical location (country, region etc) where possible.
Age: youth, adolescents and adults, generally young people versus adults (15–18, 18 and older).
Type of AT: (communication, mobility, educational etc).
Setting: community setting, institutional, work place, educational setting etc.
Dissemination plans
We aim to publish at least one peer-reviewed journal article, with the possibility to publish others depending on the findings we derive from the subgroup analyses outlined above. We will also present the findings at conferences and seminars, to the internal audience at Trinity College Dublin, within the ASSISTID research programme, and within the GATE community. We also aim to produce a briefing paper for service providers such as Daughters of Charity services and policy makers in Ireland.
References
Footnotes
Contributors JO is the guarantor of the review and drafted the manuscript. GF and GS led the technical development of the methodology. FL, BK, RM, JD, MC and MM provided a critical review of the protocol to ensure rigour and validity based on their extensive expertise in disability, systematic reviews, information management, and health and social care research. MC advised on how to keep the review manageable. JO, GF and GS designed and validated the search strategy and will retrieve and screen the data. GS will lead the data management and screening and editing of the manuscripts. All authors read and critiqued the draft and approved the final version of this manuscript.
Funding This research was supported by funding from the charity RESPECT and the People Programme (Marie Curie Actions) of the European Union’s Seventh Framework Programme (FP7/2007-2013) under REA grant agreement no. PCOFUND-GA-2013-608728. The Charity RESPECT and EU Marie Curie Actions cofund as outlined above. The funder provided the salary and all related research expenses incurred by Trinity College Dublin (TCD) in hosting JO during a two-year fellowship.
Disclaimer The funder was not involved in the design and implementation of the review.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Author note We will seek to minimise the risk of bias by trying to avoid any need to amend this protocol. However, should there be a need to revise the protocol, we will provide relevant details and the rationale for such changes. Any potential amendments will be documented and implemented by the first author, with the approval of all the contributing authors.