Article Text

Abstract
Purpose Little information is available on patients on antiretroviral treatment (ART) after a long-term period from sub-Saharan Africa, with the longest follow-up and related outcomes being after 10 years on ART. At the Infectious Diseases Institute (IDI) (Kampala, Uganda), we set up a cohort of patients already on ART for 10 years at the time of enrolment, who will be followed up for additional 10 years.
Participants A prospective observational cohort of 1000 adult patients previously on ART for 10 years was enrolled between May 2014 and September 2015. Patients were eligible for enrolment if they were in their consecutive 10th year of ART regardless of the combination of drugs for both first- and second-line ART. Data were collected at enrolment and all annual study visits. Follow-up visits are scheduled once a year for 10 years. Biological samples (packed cells, plasma and serum) are stored at enrolment and follow-up visits.
Findings to date Out of 1000 patients enrolled, 345 (34.5%) originate from a pre-existing research cohort at IDI, while 655 (65.5%) were enrolled from the routine clinic. Overall, 81% of the patients were on first line at the time of the enrolment in the ART long-term cohort, with the more frequent regimen being zidovudine plus lamivudine plus nevirapine (44% of the cohort), followed by zidovudine plus lamivudine plus efavirenz (22%) and tenofovir plus lamivudine or emtricitabine plus efavirenz (10%). At cohort enrolment, viral suppression was defined as HIV-RNA <400 copies/mL was 95.8%.
Future plans Through collaboration with other institutions, we are planning several substudies, including the evaluation of the risk for cardiovascular diseases, the assessment of bone mineral density, screening for liver cirrhosis using fibroscan technology and investigation of drug–drug interactions between ART and common drugs used for non-communicable diseases.
- cohort profile
- HIV
- antiretroviral treatment
- long tern outcomes
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
There is a rich range of clinical information collected and high quality of the generated data.
The cohort is a research platform for a wide range of substudies.
This cohort does not generally represent patients started on antiretroviral treatment (ART) but patients who after ART initiation have survived and been retained in care.
Introduction
The scale up and expansion of access to antiretroviral treatment (ART) have improved the clinical outcomes of HIV-positive patients in resource-limited settings. Overall, programmes have reported a decline in mortality1 2 and opportunistic infections,3 good immune-reconstitution in terms of CD4 count gain,4 high levels of adherence5 and acceptable rates of viral suppression.6 7
To our knowledge, only two analyses have reported outcomes of patients on ART up to 10 years of follow-up,8 9 and information on long-term complications of ART and non-HIV-related events is still limited. Although data are available from resource-rich settings, this information may not be applicable to sub-Saharan Africa due to the different ART drugs used10 and ART monitoring strategies,11 different HIV subtypes,12 as well as ethnicity and endemic diseases.
Concurrent with the second decade of ART delivery in sub-Saharan Africa, we set up a cohort of ART-experienced patients (on ART for 10 years at the time of enrolment), at the Infectious Diseases Institute (IDI), Kampala, Uganda, who will be followed up for additional 10 years. The main objectives of this cohort are to determine the incidence of long-term side effects and drug toxicity, ART durability and development of morbidities with the emphasis on non-communicable diseases.
The aim of this paper is to present the scope, the methods and the baseline clinical profile of the ART long-term (ALT) cohort.
Methods
Organisation and ethics
The team of investigators consists of five physicians, one statistician, one data manager and one quality assurance manager; in 2013, the investigators conceived the study and sought for institutional and ethical approval. The study preparation took place in the first quarter of 2014. The study was approved by the research ethics committee of the Joint Clinical Research Center. The study is registered with Clinical trials.org (https://clinicaltrials.gov/) as ‘Outcomes of HIV Infected Individuals after Ten Years on Antiretroviral Treatment’ Protocol Record ST/0113/15.
Our work adheres to the ‘Strengthening the Reporting of Observational Studies in Epidemiology’ (STROBE) recommendations that provide guidance on the reporting of cohort studies (see STROBE checklist).
Study site
The study patients were recruited in the adult HIV clinic at IDI. IDI is a centre of excellence13 for HIV treatment and prevention with over 30 000 patients ever registered in the clinic. Antiretroviral drugs have been provided by the Global Fund and the President’s Emergency Plan for AIDS Relief starting in 2004. ART is provided and monitored according to the prevailing WHO and/or Uganda Ministry of Health guidelines since 2004. First-line ART regimens include two nucleoside reverse inhibitors (NRTI) combined with a non-nucleoside reverse inhibitors; patients who fail first-line ART receive a second-line combination which includes two NRTIs and a protease inhibitor for second-line ART.10 14–16
Patients started on ART in the clinic are initially followed up monthly for the first year and then, if stable, are seen by a doctor every 3 months and in between come for monthly drug refill (pharmacy visit). Patients on ART were monitored with CD4 count measurement every 6 months up to December 2014 according to the national guidelines; however, ad hoc viral load (VL) testing was made available for patients suspected to have treatment failure based on WHO suggested immunological criteria. The roll out of routine VL monitoring was started in Uganda at the end of 2014.
In 2004, 559 consecutive adult patients starting ART were enrolled into the IDI research cohort and followed up for 10 years; these patients received study visits every 3 months and in between came monthly only for routine clinic visits in the first year and pharmacy visits thereafter. For this group of patients, resources were available for biannual prospective virological monitoring from study enrolment; details and outcomes of this cohort were previously described.8 9 17
The patients of the ALT cohort were recruited from both the adult HIV clinic and patients discharged from the IDI research cohort. This enrolment strategy was chosen to include patients whose prior ART had been monitored using CD4 counts, which was at the time the standard of care, and those monitored through prospective VL testing, which is considered the gold standard.
Systematic and quality-controlled data electronic capture was implemented in 2004, and information is collected and stored in the IDI electronic database, known as the Integrated Clinic Enterprise Application (ICEA). This is an in-house built system based on Microsoft.NET technologies, developed in order to ensure a high standard of data.18
Study design
A prospective closed observational cohort of 1000 patients previously on ART for 10 years was enrolled between May 2014 and September 2015 and will be followed up for 10 years. The sample size was conveniently chosen and guided by financial considerations; however, power calculations performed a priori showed sufficient power to detect potential outcomes of interest even at prevalence <5%. Patients were eligible to be enrolled in the study if they were at least 18 year old, were willing to participate in the study and comply with the study procedures, and were in their consecutive 10th year of ART regardless of the combination of drugs for both first- and second-line ART. Ten-year consecutive ART use was determined using the data collected in ICEA.
Subjects were excluded from the study if they had been previously enrolled in clinical trials requiring drugs or combinations different from those recommended by the WHO guidelines, had been on ART before enrolling for care at IDI (given the limited reliability or lack of information about their medical and ART history prior to registration at IDI) and if at any point were lost to follow-up, defined as not returning to the clinic for either doctor visit or pharmacy refill for more than 3 months.
Study procedures
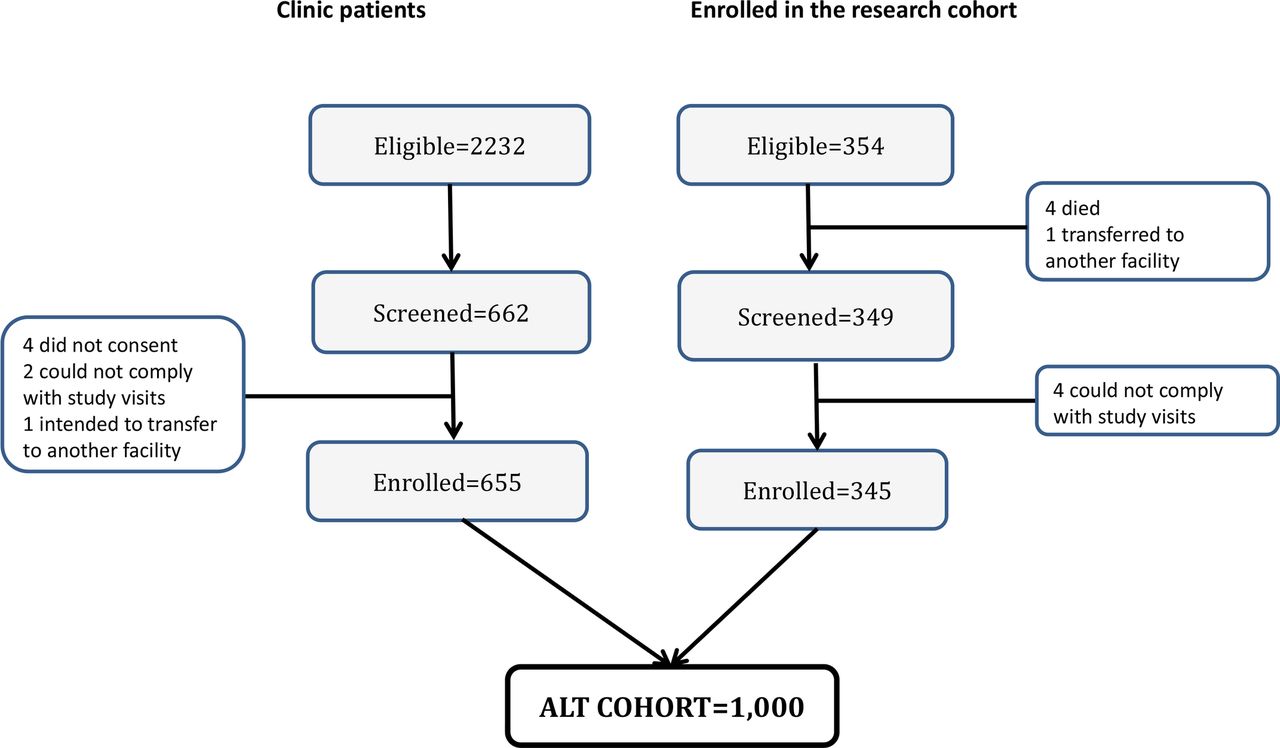
A list of all eligible patients by ART duration in the adult HIV clinic was generated from the database; 2232 patients were identified, and their clinic files were flagged using designated stickers. All patients (354) discharged from the IDI research cohort had accrued 10 years on ART, and they were therefore eligible for the study. All patients from the IDI research cohort and all consecutive eligible subjects who presented for their appointment at the clinic were offered screening to ascertain all inclusion criteria were met, and to rule out exclusion criteria. Eligible subjects who were willing to participate in the study provided written consent and were enrolled in the study on the same day.
General medical history, physical examination, adherence to ART and prescription of drugs are performed at enrolment and all study visits. Follow-up visit are scheduled once a year for 10 years; in addition to study visits, the participants attend the general clinic every 3 months to pick up their ART and concomitant medications. Antiretroviral drugs are prescribed according to the WHO guidelines; patients with two consecutive VL >1000 copies are consider to have treatment failure and deemed to be eligible for treatment switch.
Laboratory tests are performed at the Makerere University-John Hopkins University (MUJHU) Core Laboratory hosted at IDI and include urine analysis, haemoglobin, alanine aminotransferases, CD4 count and HIV VL. The following tests are performed only when required: full blood count if haemoglobin <10 g/dL, electrolytes and blood sugar if proteinuria or glucose is detected in the urine analysis and pregnancy test if the last menstrual period occurred more than 30 days prior to the study visit. Biological samples are processed and stored by the IDI research translational laboratory as follows: at enrolment packed cell pellets (five aliquots), plasma (four aliquots) and serum (four aliquots); during follow-up, plasma (one aliquot) and serum (three aliquots). Funds will be sought for additional procedures and laboratory testing on the stored samples such as, but not limited, to metabolic markers, resistance testing and drug levels.
Data collection
Real-time data entry into ICEA is performed by the respective providers. Laboratory results performed in the MUJHU Core Laboratory are entered into the laboratory electronic database and are automatically downloaded daily into the ICEA database.
The questionnaires were designed by the study investigators. Variables collected include basic demographic and epidemiological data, clinical history, present clinical information including vital signs and body weight, haematological and chemistry laboratory results, medications, ART regimen, adherence to ART, drug toxicities, quality of life and sexual behaviour. Details of these variables are presented in table 1.
Type and description of the variables collected in ART long-term cohort
All the data collected into ICEA are validated by a quality control officer who ensures that the data are complete and consistent.
Data availability and collaborations
Proposals for use of the ALT cohort data can be submitted to the investigators committee for review of the analysis plan and for scientific advice. Scientists intending to use data of the ALT cohort can access the data after signing a data sharing agreement and must conduct the analysis in collaboration with the investigators. The study is also open for external partnerships ranging from substudies within the parental ALT cohort to collaborations with other cohorts; full written proposals are submitted to the investigators committee, and on approval, a collaboration agreement must be signed by both parties.
Definitions and statistical methods
We described patients’ characteristics at the time of enrolment in the cohort and at the time of ART start. We compared the characteristics of the patients previously enrolled and those who were not enrolled in the IDI research cohort using χ2 test for proportions and Mann-Whitney U test for variables not normally distributed. Laboratory tests were considered done at time of enrolment at ART start if they were performed within 183 days before or within 14 days after the clinic visit.
Results
Cohort profile and follow-up
From May 2014 to September 2015, a total of 1000 patients were enrolled in the ALT cohort. Of the 354 of the 559 patients who completed 10 years of follow-up (with the others been lost, dead, withdrawn or transferred out8) and were discharged from the IDI research cohort (henceforth referred as IDI research cohort patients), four died and one was transferred out before enrolment in the ALT cohort started; of the remaining screened 349, 345 patients were enrolled in the ALT cohort. Of the 2232 eligible patients from the routine clinic who had not been part of the IDI research cohort (hereafter referred as clinic patients), 662 consecutive patients were screened, and 655 were enrolled. Reasons for declining to participate in the study are shown in figure 1.

Screening and enrolment of patients into the cohort.
Table 2 shows the patients characteristics of the ALT cohort patients at the time of ART initiation stratified by enrolment in the previous research cohort.
Patients’ characteristics of the ART long-term cohort patients at the time of ART initiation, stratified by enrolment in the previous research cohort
Generally, at the time of ART initiation compared with clinic patients, the IDI research cohort group had a higher proportion of female (70.1% vs 57.6%, p<0.001), a higher proportion of patients in WHO stage 3 or 4 (89.7% vs 72.9%; p<0.001) and a higher proportion of patients was started on efavirenz-based regimens (26.4% vs 16.2%; p=0.010). Additionally, the IDI research cohort patients were younger (median age 35 vs 36; p=0.008), had a higher haemoglobin (11.8 vs 11.4 g/dL; p=0026) and a higher CD4 count (102 vs 66 cells/µL, p=0.004) as compared with the clinic patients.
Table 3 shows the patients characteristics of the ALT cohort patients at the time of enrolment in the study stratified by enrolment in the previous research cohort.
Patients’ characteristics of the ART long-term cohort at cohort enrolment stratified by previous enrolment in the Infectious Diseases Institute research cohort
Generally, at the time of enrolment in the study, compared with clinic patients, the IDI research cohort group had a higher proportion of patients in WHO stage 3 or 4 (93.3% vs 84.2%; p<0.001), a lower haemoglobin (13.4 vs 14.5 g/dL; p<0.001) and a higher CD4 count (624 vs 450 cells/µL; p=0.004). We observed differences also in the history of opportunistic infections and drug substitution across the two groups. There were no differences in the proportion of patients on first and second lines between the IDI research cohort patients and the clinic patients, as well as in the proportion of patients with VL ≥400 copies/mL at time of enrolment.
Approximately one quarter of the patients had hypertension at the time of enrolment in the ALT cohort; hypertension was defined as more than three systolic measurements above 140 mm Hg or diastolic measurement above 90 mm Hg or being on antihypertensive drugs (as per ICEA) or patient-reported hypertension.
Overall, we did not observe a difference in the proportion of history on non-communicable diseases between the groups (hypertension, cardiovascular diseases or diabetes). Seventy-five per cent of the patients reported that alcohol consumption and tobacco use were more frequent in the clinic patients group as compared with the research cohort group (25.6% vs 19.2%; p=0.024).
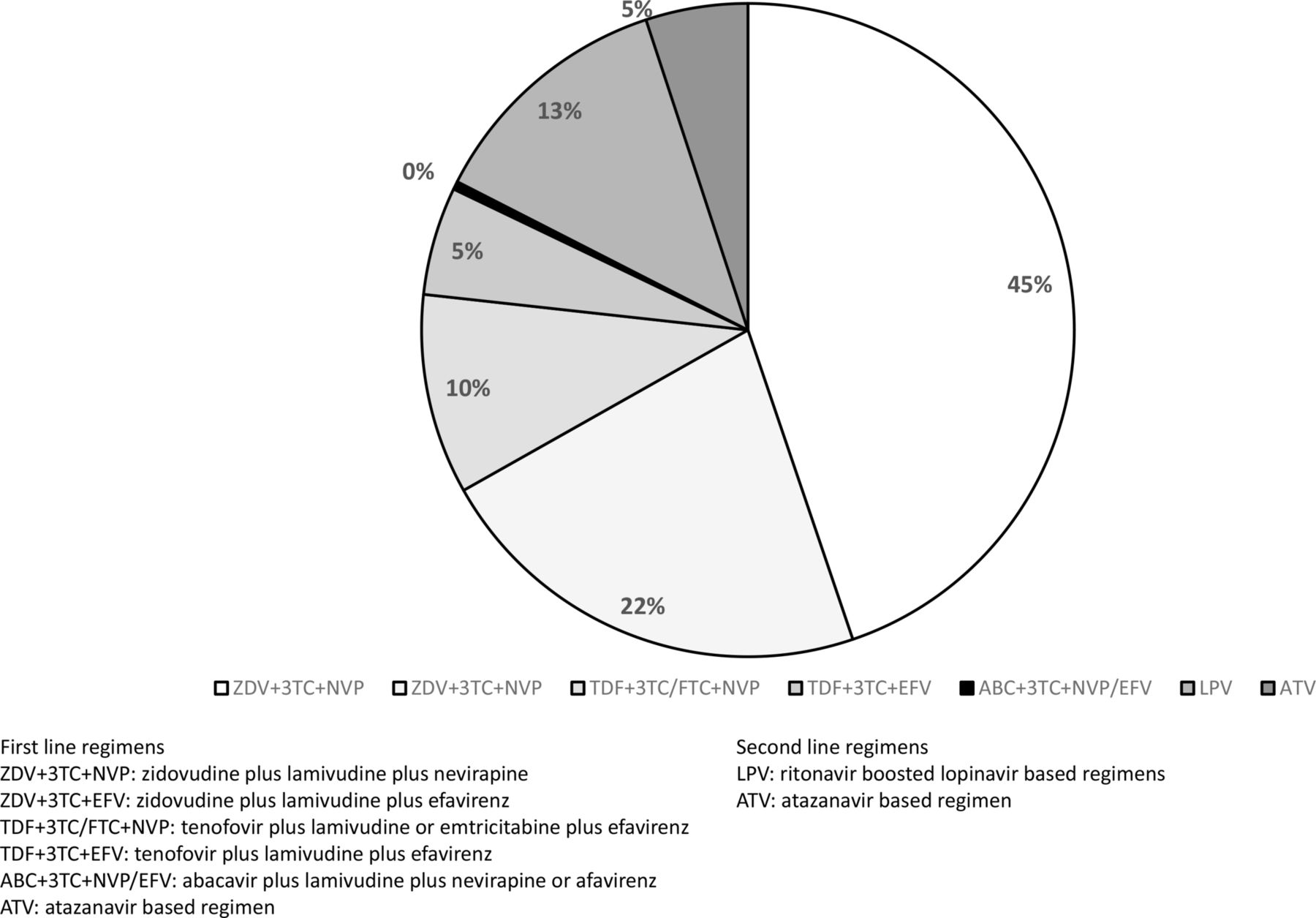
Figure 2 describes in detail the ART regimens at the time of enrolment in the ALT cohort. Overall, 81% of the patients were on first line, with the more frequent regimen being zidovudine plus lamivudine plus nevirapine (44% of the cohort), followed by zidovudine plus lamivudine plus efavirenz (22%) and tenofovir plus lamivudine or emtricitabine plus efavirenz (10%). Of the 19% of the patients on second-line ART, the majority received ritonavir-boosted, lopinavir-based regimens (14%), and the remaining ones ritonavir-boosted, atazanavir-based regimens (5%).

{kind=link}
{kind=link}
Antiretroviral treatment regimen at cohort enrolment.
After 1 year of follow-up, we observed 98.2% retention, with 10 patients dead, seven lost to follow-up and one transferred on request to another facility.
Discussion
We have presented the ALT cohort, a group of 1000 patients on ART for 10 years and with a planned long follow-up period (an additional 10 years). We believe that this will be an important clinical research platform to understand long-term ART outcomes such as durability of first and second lines and the emergence of non-communicable diseases among patients who have been on long-term ART. While there are published data from cohorts in other settings,19 20 there is need to start collecting detailed information, particularly on non-communicable diseases and other long-term complications from resource-limited settings and sub-Saharan Africa. The aim of this paper was to present the characteristics of this cohort as a forecast of its potential use for clinical research and potential substudies. The unique feature of our cohort is that the patients enrolled in this study have been exposed to a wide range of antiretroviral drugs for longer periods than most of the patients in sub-Saharan Africa. The analysis of data from the ALT cohort will provide evidence that is more generalisable to routine settings, as compared with that generated by clinical trials, with particular emphasis on long-term outcomes and toxicities of patients on ART, as well as non-communicable diseases and first- and second-line durability.
In summary, this is a cohort of patients, of whom the majority were female, who had severe immunosuppression at ART start, denoted by their low CD4 count and advanced WHO clinical stage; most of the patients were started on nevirapine-based regimens, combined with lamivudine and stavudine; of note, stavudine was phased out in Uganda in 2008 due to its toxicity, following a directive of the Ministry of Health. By the time of enrolment in the ALT cohort and after 10 years on ART, the patients demonstrated a robust immune recovery, notably with more than 80% of the patients being still on first-line drugs and with less than 5% experiencing virological failure.
The most common non-communicable disease reported was hypertension (21%), followed by diabetes (3%) and cardiovascular diseases (1%). One quarter of the participants reported tobacco use and three quarter alcohol consumption; unfortunately, we did not collect this information at the time of ART initiation.
Surprisingly, we did not find any difference in virological outcomes at cohort enrolment in patients who were previously monitored with exclusively CD4 count and with CD4 counts plus VL testing. This seems to be in contradiction with the extensive evidence in the literature of immunological monitoring not being enough sensitive or specific in identifying patients with virological failure.21–23 It is possible that these patients, who have been in the continuum of care for 10 years as opposed to patients who drop out of care, have had good adherence to ART regardless of the modality of monitoring.
One strength of this cohort is the rich range of clinical information collected and the high quality of the generated data that we anticipate, given the high standard of data collection that we demonstrated in the past18 using our database with real-time data entry by providers.
A study limitation of this cohort is the inherent survival bias, whereby only patients who survived and were retained in care after 10 years are enrolled. Consequently, these patients do not necessarily represent all patients started on ART in the earlier rollout of ART that was often characterised by severe immunological suppression and resulting high mortality. Survival bias is a common phenomenon in clinical epidemiology, and the study investigators will ensure that all outcomes from this cohort are evaluated with the correct methods, including but not limited to those that account for time-varying covariates at the time of any analysis.24 On the other hand, the patients in the ALT cohort are likely to be representative of the patients who started treatment during the initial roll out of ART, particularly with similar degrees of immunosuppression25 and history of drug substitutions, and are currently being seeing by healthcare providers in sub-Saharan Africa.
Through collaboration with other institutions, we are planning for several substudies, including evaluating the risk for cardiovascular diseases at cohort enrolment and follow-up, measuring bone mineral density, screening for liver cirrhosis using fibroscan technology and investigating drug–drug interactions between ART and common drugs used for non-communicable diseases.
In conclusion, we envisage that the data presented as well the future prospective data from this study could contribute to increasing knowledge and improving best clinical care practices in resource-limited settings, particularly sub-Saharan Africa, where the roll out of ART was successfully implemented. This will help us to best ensure beneficial and sustainable patients’ clinical outcomes.
References
Footnotes
Contributors BC wrote the first draft of the manuscript; FM and AKi extracted and analysed the data; RM, PG, OM, BC and RPR wrote the study protocol and implemented the cohort; BC, FM, AKi, OM, RM, PG, AK and RPR provided comments to the manuscript and approved the last draft.
Funding This research was partly funded through a grant from the Johnson & Johnson corporate citizenship trust.
Competing interests None declared.
Patient consent Obtained.
Ethics approval IRB of the Joit Clinical Research Center (JCRC) Uganda.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data is available and stored at the Infectious Diseases Institute. It is available upon request.