Article Text

Abstract
Objective Non-communicable diseases (NCDs) impose a significant health and economic burden. This study aimed to assess the differential attendance patterns of public to different healthcare professionals and gauge the opinions of key stakeholders towards screening of NCDs by allied healthcare professionals.
Design Questionnaires were designed piloted and subsequently completed by key stakeholders. The results were analysed descriptively.
Setting Public questionnaires were undertaken in a West Midlands transport station and Public Markets. High street dental and community pharmacy settings were selected via local clinical and research networks. Healthcare professionals were identified using professional networks and were emailed a web link to an online survey.
Participants 1371 members of the public, 1548 patients and 222 healthcare professionals (doctors general practitioner (GP), dentists general dental practitioner (GDP) and pharmacists) completed the questionnaires.
Outcome measures The outcome was to compare attendance patterns at GDP and GP practices to determine whether different populations were more likely to access different healthcare professionals, this included determining when patients were last screened for NCDs by their GP. Additionally, the willingness of patients to undergo the required intervention and the opinions of stakeholders regarding the concept of screening for the specified NCDs in general dental and community pharmacy settings were also explored.
Results 12% of patients who reported seeing a GDP biannually reported that they had not had contact with a GP in the last year. Over 61% of the public reported attending a GDP biannually, of this group 48% reported having never had a check-up at the GP. All stakeholders surveyed were in broad support of the concept of allied health professionals undertaking screening for specific general health conditions.
Conclusions This study has established that allied healthcare professionals may have access to different cohorts of the population to GPs. If GDPs and pharmacists have access to patients who are not using healthcare services elsewhere, they may be ideally placed to risk assess, and where appropriate offer preventative advice and test for NCDs.
- dental
- Pharmacy
- general practitioner
- allied healthcare professional
- non-communicable diseases
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The main strength of this study was the large sample size. In total 2919 questionnaires were returned by the public and patients with a further 222 healthcare professionals completing the questionnaires.
The results of this study align closely with the findings from studies in the UK and USA.
In the UK, screening is controversial, National Institute for Health and Care Excellence guidelines exist on risk assessing and screening for type 2 diabetes mellitus, however, the UK National Screening Committee does not currently advocate screening for non-communicable diseases.
Introduction
The prevalence of chronic, non-communicable diseases (NCDs) is increasing worldwide and their impact on the healthcare economy is substantial1–3 with 92% of older adults having at least one NCD and 77% having two NCDs.4 The increasing prevalence of NCDs is partly due to an ageing population, and partly due to an increase in prevalence of shared risk factors among multiple NCDs, such as sedentary lifestyles, diets high in refined carbohydrates, smoking and obesity. Furthermore, risk factors for NCDs contribute a significant economic burden, accounting for over 45% of total National Health Service (NHS) costs in the UK in 2006–2007, at approximately £43 billion.5
The National Institute for Health and Care Excellence (NICE) currently recommend that allied healthcare professionals, including community pharmacists and general dental practitioners (GDPs), should risk assess for type 2 diabetes mellitus (T2DM).6 For example, for T2DM data from the USA suggest that screening for T2DM in a dental setting is effective in identifying both prediabetes and diabetes.7–9 Early detection also led to the instigation of cost-effective lifestyle change measures, rendering a proportion of prediabetes patients normoglycaemic.10 A further survey from the USA showed that 24% of people did not have contact with a general healthcare provider in 2008, yet 23% of those sampled did see a dentist in that year.11 Furthermore, UK government policies have been set out, actively encouraging dental professionals in the provision of general health promotion12 13 as GDPs already deliver advice on diet and smoking cessation. It has been suggested that highly skilled primary healthcare professionals, such as pharmacists and dentists (GDPs), may develop new roles and work more closely with general practitioners (GPs) to create effective multidisciplinary teams and care pathways, and provide a wider range of services such as early detection of disease.14
The 2011 Pharmaceutical Group of the European Union survey showed that 98% of European patients can reach their nearest community pharmacy within 30 min, while 58% indicated that their closest community pharmacy was within 5 min of their home. In addition, over the past four decades, there has been a move in pharmacy practice away from the traditional focus on dispensing towards a more patient-centred clinical role.15 UK policy and pharmacists’ professional organisations have stressed the potential of community pharmacists to extend their roles in patient care services to include services such as screening for NCDs. This role has been emphasised in policy papers calling for a wider use of community pharmacists in primary patient care.16–18
The development of government policies and guidelines advocating the role of allied healthcare professionals in risk assessment, prevention programmes and risk identification for NCDs suggests that a collaborative approach to tackle the growing NCD burden is required. However, the opinions of members of the public, patients and relevant healthcare professionals in this matter remain poorly explored.
Thus, the aim of this study was to collect preliminary data to provide insight into the differential attendance patterns of public and patients to different healthcare providers, and the perceptions of key stakeholders including members of the public, patients and healthcare providers (GPs, GDPs and pharmacists), regarding risk-targeted screening programmes in dental and pharmacy settings for specific NCDs (T2DM, cardiovascular disease (CVD), chronic kidney disease (CKD) and respiratory chronic obstructive pulmonary disease, COPD) known to incur a significant health and economic burden.
The choice of targeting particular diseases for screening is supported by the fact that:
Strong evidence suggests that the majority of patients with objective COPD are not aware of their condition, and this leads to a significant delay in diagnosis and potential treatment.19
Both T2DM and hypertension tend to be asymptomatic and are usually not diagnosed until patients develop symptoms.20
Atrial fibrillation is a major treatable risk factor for stroke, but it may be hard for patients to self-detect, because it is frequently silent and intermittent21 22;
Early diagnosis of CKD and immediate referral are key steps in the management of CKD because this allows implementation of preventive measures that delay or even halt progression of CKD to end-stage renal disease.23
Materials and methods
Patient involvement
The development of the research question was informed by discussions with an advisory group comprising senior dental and medical academics working in the fields of NCDs. The research question was then taken to patient focus groups and refined following discussions with patient and public advocates at a health awareness engagement event (AGEWELL).
Patients were involved in the design of the study through feedback and discussions relating to the questionnaire design.
Results will be disseminated through publication, presentation at conferences and returning to the annual AGEWELL engagement event to present findings.
Surveys
Questionnaires were developed that explored the attitudes of the public, patients and registered healthcare professionals (GPs, GDPs and pharmacists). Data were collected on attendance with healthcare professionals, participant demographics and their opinions on having general health checks in the specified setting.
No personal identifiers were collected.
Public survey
To assess the views of members of the public, we conducted surveys in two different settings, Birmingham New Street Railway Station (n=909) and Birmingham Public Markets (n=462), between June and September 2016. There was no predefined target sample size; instead, 6 days were spent at each site with an aim to recruit as many participants as possible. Potential participants were informed about the study and offered a patient information sheet, information posters were displayed explaining the study. Participants who verbally consented to participate were then asked to complete the electronic questionnaire on a tablet computer (figure 1).
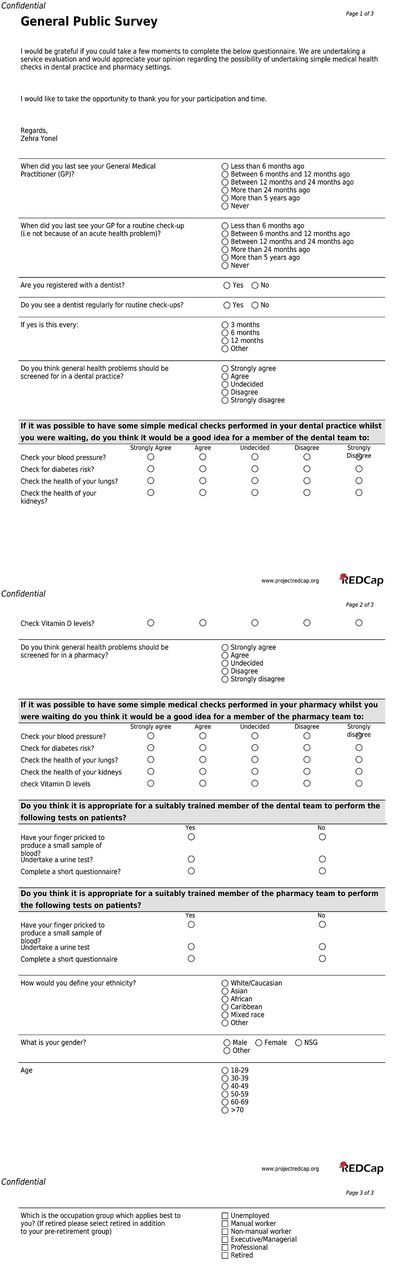
Public questionnaire. REDCap, Research Electronic Data Capture.
In addition to basic demographic data, including age, ethnicity, gender and occupational status, questions were asked regarding last attendance with a GP and last time a GP surgery was visited for a check-up (ie, not due to an acute health concern). Participants were also asked whether they are registered with a dentist, whether they see a dentist for a routine check-up and, if so, at what frequency. In addition, participants were also asked whether they felt general health problems should be ‘screened’ for in a dental or pharmacy setting. Participants were asked their opinions regarding screening for specific conditions including hypertension, diabetes, lung health and kidney health, on a 5-point Likert scale. Similarly, patients were asked to rate their willingness to undergo a finger-prick capillary blood test, urine test or complete a questionnaire for screening purposes. These questions were asked separately for screening in dental practice and for a community pharmacy setting.
Patient surveys
To assess the views of patients, surveys were conducted in dental practices and pharmacies. Patients were identified from 13 NHS dental practices in England (n=515) and a private dental practice in Scotland (n=500) and 25 community pharmacies in England (n=533). Similar to the public questionnaires, information posters were displayed explaining the study. Patients were told about the study and offered a patient information sheet. If patients verbally consented to participate, a paper questionnaire was made available for them to complete and return to the practice staff. Content and format of the patient questionnaire was similar to that of the public questionnaire.
Professional surveys
To determine the views of healthcare professionals, GPs (n=48), GDPs (n=129) and pharmacists (n=45) were contacted by email via known professional networks including the clinical research networks. The email contained a participant information sheet and electronic link to the online questionnaire. The questionnaire requested participants to disclose their occupation and whether they worked on a private, NHS or mixed (both private and NHS) basis. The respondent was also asked their opinion regarding dentists and pharmacists screening for specified NCDs (hypertension, diabetes, CKD, COPD). The survey also determined whether professionals felt it would be appropriate for a suitably trained member of the dental/pharmacy team to perform finger-prick capillary blood tests, questionnaires or urinalysis on patients to obtain the relevant biomarker information. Further to this, demographic data in terms of age, gender, location of practice were also recorded.
Analysis
Summary statistics were calculated using Stata/IC V.12.1 (StataCorp LP).
Data sharing statement
Pseudonymised individual participant data, used in preparation for this manuscript, will be available immediately following publication for a period of 36 months. This will be available to researchers providing a methodologically sound proposal and for the purposes of achieving the aims of that proposal only. Proposals should be directed to the corresponding author. To gain access, researchers will need to sign a data access agreement.
Results
In total, 2919 public and patient questionnaires were returned in this study: Birmingham New Street railway station, (n=909), Birmingham Public Markets (n=462). Patient questionnaires were completed in NHS dental (n=515), private dental (n=499) and pharmacy (n=533) settings (table 1).
Demographics of public and patient respondents (figures presented as percentage unless otherwise stated)
Public questionnaires
Attendance
Twenty-two per cent of respondents at New Street railway station and 26% at Birmingham Public Markets reported they had not had any contact with their GP within the preceding 12 months. Almost 10% of the public reported not having seen a GP in at least 5 years (table 2).
Comparison of attendance patterns to general practitioner (GP) practices for the public and those attending pharmacy and dental practices (figures presented as percentage unless otherwise stated)
Twenty-six per cent of respondents at New Street station and 31% at Birmingham Public Markets reported attending their GP surgery for a routine check-up and not due to an acute illness within the last 12 months. Respondents in public settings were less likely to attend a GP surgery for a routine check-up compared with those patients attending dental or pharmacy settings (table 2).
Seventy-seven per cent of respondents at Birmingham New Street railway station and 61% at the Birmingham Public Markets reported being registered with a dentist. When asked about attendance pattern with a dentist, the most frequently reported appointment interval for both public settings was 6 monthly (table 3).
Comparison of the reported frequency of dental check-ups, for those members of the public who reported that they attended a dentist (general dental practitioner) regularly
When comparing attendance of members of the public at their GP or their GDP, 12% of patients who reported seeing a GDP every 6 months reported that they had not had contact with a GP in the last year. Furthermore, of the public respondents that reported being regular dental attenders 48% reported having never had a health check at their GP surgery. An additional 20% of the public who reported being regular dental attenders claimed to have not attended a GP practice for a routine check-up in the last 12 months and of the 48% that reported having never had a check-up at the GP surgery 61% reported attending a dental practice biannually.
Opinions
Public support for screening for medical conditions in both dental and pharmacy settings was strong, with 74% in favour of screening in dental settings and 70% in favour of screening in pharmacy settings. The conditions that most public respondents were in support of screening for were T2DM and hypertension in both dental and pharmacy settings. The public expressed willingness to undergo each of the proposed interventions (urinalysis, finger-prick capillary blood) in both settings with a slight preference for the dental setting.
Patient questionnaires
Attendance
Twenty-eight per cent of respondents at NHS GDP settings, 25% of respondents at private GDP settings and 17% of patients at pharmacies reported they have not had any contact with their GP within the last 12 months. Seven per cent of respondents at NHS GDP settings, 5% of respondents at private GDP settings and 3% at pharmacies reported having not seen a GP in at least 5 years.
Forty-six per cent of respondents at NHS GDP settings, 57% of respondents at private GDP settings and 51% at the pharmacies reported attending their GP surgery for a routine check-up within the last 12 months.
Patients attending dental or pharmacy settings were more likely to attend a GP surgery for a routine check-up compared with those in public settings. Those patients attending a pharmacy were not asked about dental attendance. When those attending dental practices were asked about attendance patterns the most frequently reported appointment interval was 6 monthly.
When comparing attendance of NHS dental patients at GP and GDP practices, of the 28% of NHS dental patients who reported they had not had any contact with their GP within the last 12 months, 42% were in favour of having NCD screening at their GDP. When comparing the attendance of private dental patients at GP and GDP practices, of the 25% of private dental patients who reported they had not had any contact with their GP within the last 12 months, 65% were in favour of having NCD screening at their GDP practice. When comparing attendance of pharmacy patients at GPs and pharmacies, of the 17% of pharmacy patients who reported they had not had any contact with their GP within the last 12 months 32% were in favour of having NCD screening at their community pharmacy.
Opinions
Forty-eight per cent of NHS dental patients either strongly agreed or agreed with the concept of screening for NCDs in dental settings. Sixty-one per cent of private dental patients either strongly agreed or agreed with the concept of screening for NCDs in dental settings. Seventy-five per cent of pharmacy patients were in support of screening for NCDs in pharmacy settings. The conditions that most of the public and patients were in support of screening for were T2DM and hypertension in both dental and pharmacy settings.
Healthcare professionals
In total 222 completed questionnaires were returned, of those returned 48% were completed by female healthcare professionals; 58% had been completed by GDPs, 21% by GPs and the remainder by community pharmacists. More than half (51%) of those questioned were treating patients within NHS settings, 34% reported working on a mixed NHS and private basis and 15% reported working on a solely private basis (table 4).
Demographic data of healthcare professional respondents (figures expressed as percentage unless otherwise stated)
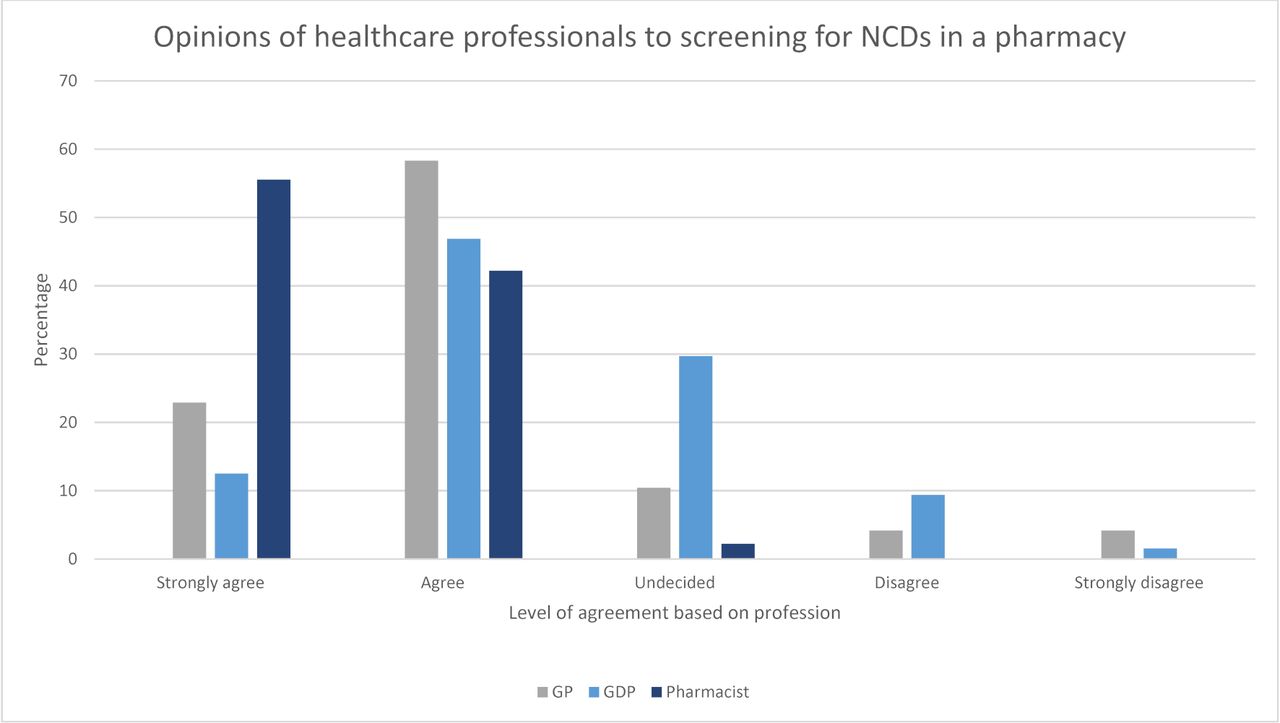
Most GDPs were in favour of risk assessment in a pharmacy setting. A large proportion of GPs and pharmacists were supportive of risk assessment in dental settings (figure 2), but many remained undecided. There was stronger support from healthcare professionals for risk assessment for NCDs in pharmacy settings (figure 3).
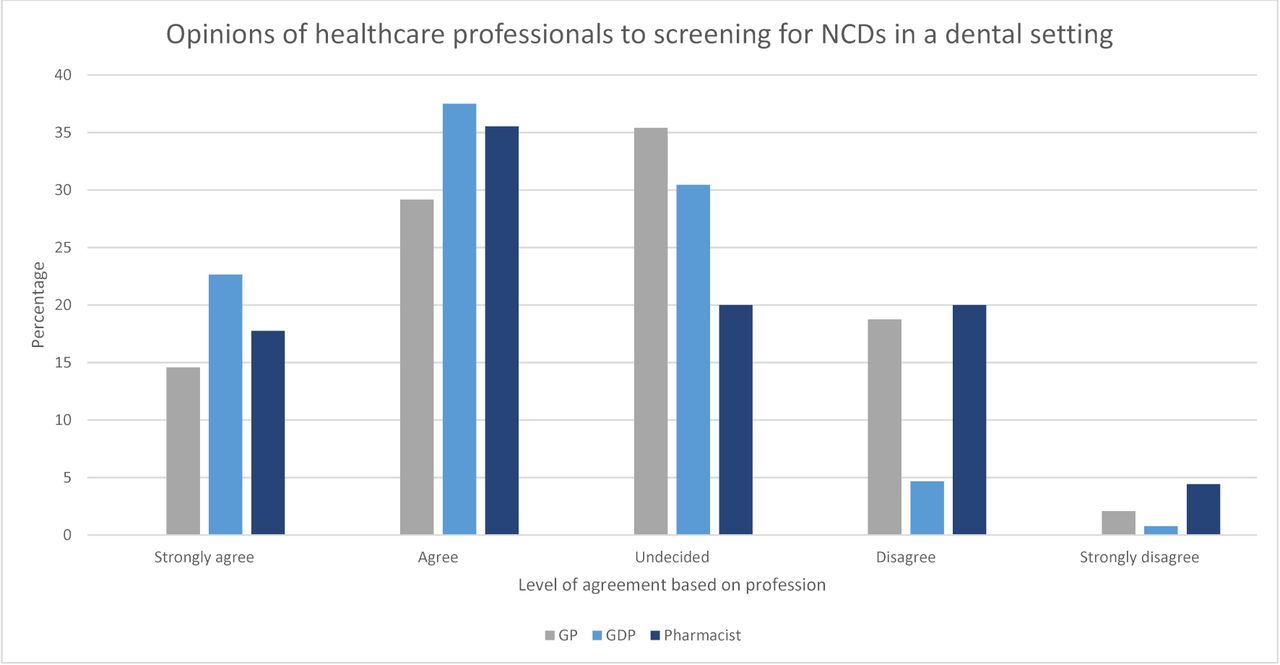
Showing professional opinion to screening in dental practice expressed as a percentage. GDP, general dental practitioner; GP, general practitioner; NCDs, non-communicable diseases.

{kind=link}
{kind=link}
{kind=link}
Showing professional opinion to screening in pharmacy expressed as a percentage. GDP, general dental practitioner; GP, general practitioner; NCDs, non-communicable diseases.
Discussion
Statement of principle findings
This study aimed to determine the attendance patterns of the public at different healthcare settings and to gauge public and patient opinions on using allied healthcare professionals to undertake ‘screening’. Participants were more likely to attend their dental practice for a routine check-up than their GP surgery. Of those patients who reported being regular attenders to a dental surgery for routine check-ups, almost half claimed that they had ‘never’ had a routine health-check at their GP surgery. Furthermore, an additional 26% had not had a routine check at the GP practice in more than 12 months. This implies that dental professionals have access to a cohort of patients who are not routinely accessing their GP surgery for health checks.
All stakeholders surveyed were in broad support of the concept of allied professionals undertaking risk assessment for general health conditions. The public were slightly more in favour for risk assessment in dental compared with pharmacy settings, whereas healthcare professionals expressed slightly greater support for risk assessment in pharmacy compared with dental settings. The conditions receiving the greatest support for risk assessment were T2DM and CVD. The methods for risk assessing that were mostly accepted were validated questionnaires and finger-prick capillary blood testing.
Strengths and weaknesses of the study
The main strength of this study was the large sample size. In total 2919 questionnaires were returned by public and patients with a further 222 healthcare professionals completing the questionnaires. However, the population captured was not representative of the UK population as a whole and caution should be applied in relating findings to the general population. The sampling method used did not allow for calculation of a response rate. Thus, potential bias cannot be ruled out. The NHS dental and pharmacy respondents were the most likely to have attended their GP practice for a routine check-up, with respondents in both public settings being the least likely to attend a GP surgery for a routine check-up. This may suggest that those patients already engaged with healthcare are more likely to take up any proposed risk assessment, should a new service become available. This finding may limit the value of any such service as those in most need of early identification, who are not in contact with a GP are also the group least likely to contact other healthcare professionals.
Strengths and weaknesses in relation to other studies
Health screening in the UK is controversial, although NICE guidelines exist on risk assessing and screening for T2DM, the UK National Screening Committee (UK NSC) currently does not advocate screening for T2DM or the other mentioned NCDs. Despite the current UK NSC position on screening, when asked whether they felt screening for NCD in dental and pharmacy settings was worthwhile most healthcare professionals were supportive of this in both settings.
The results of this study align closely with the findings of Greenberg’s study in the USA, which reported that dentists were in support of chairside screening for medical conditions and were willing to undertake the screening procedures.24 Creanor et al undertook a similar study in the UK whereby patients attending dental clinics in the Southwest of England were asked about diabetes screening. They found that 61% of respondents had never knowingly been screened for diabetes, 87% were in support of screening for medical conditions such as diabetes at the dental clinic.25 This was further supported by a study in Warwickshire where adult patients with diabetes attending medical clinics were asked about screening for diabetes in dental settings. Bowyer et al reported that over half of respondents supported the idea of dentists’ involvement in diabetes screening.26
Furthermore, a study by Bould et al found that the uptake of risk assessment methods for diabetes in dental settings was positive, patients were amenable to finger-prick testing and when a two-stage screening process was employed (validated questionnaire prior to finger-prick test) patients were three times as likely to follow-up with their GP compared with those receiving only one positive result.27
In a recent review of community pharmacy clinical services Murray 2016 (PSNC, 2016) concluded that community pharmacists should develop interventions to further prevent disease progression. Previous evidence from systematic reviews and meta-analyses has shown that community pharmacies could be feasible sites for screening for isolated risk factors.28 29 Screening for individual risk factors in pharmacies has been shown to be effective, in studies in the UK30 and in countries outside the UK.31 32 Furthermore, UK public health initiatives have been previously tested in pharmacies and claimed some success, such as healthy living pharmacies (public health-related services) and health checks (cardiovascular risk assessment). However, further research is needed to determine the uptake of pharmacy recommendations and referrals following the screening and the cost-effectiveness of screening in pharmacies compared with screening from other providers.
Meaning of the study
The choice to seek public, patient and professional opinions for using allied health professionals to undertake proactive targeted risk assessment to the specific NCDs was based on the significant health and economic burden that NCDs have on individuals and society as a whole.33
Utilisation of allied healthcare professionals would be particularly interesting if different healthcare providers could reach/access different population groups. Our surveys demonstrated that, of those patients who reported being regular attenders to a dental surgery for routine check-ups, almost half of patients claimed that they had ‘never’ had a routine health check at their GP surgery. Furthermore, an additional quarter of those surveyed had not had a routine check at their GP practice in more than 12 months. This may indicate that dental professionals have access to a cohort of patients who are not routinely accessing their GP surgery for health checks. However, there is a possibility that many GPs use appointments that were not necessarily booked with health checks in mind to offer opportunistic risk assessment to patients they deem high risk. Thus, patients were also asked about general attendance at GP surgeries, and of those respondents who reported attendance at a dental practice within 12 months, 21% claimed to have not attended their GP practice within the same period. Therefore, this still suggests a potential missed opportunity for risk assessment and preventative advice as one in five patients attending dentists have not had contact with a GP practice within that year.
Our findings support the concept that many people only attend their GP when they are unwell, whereas by contrast, they may visit allied health professionals on a regular basis, even when asymptomatic. With longer opening hours for pharmacies and easy accessibility to dental practices, this potentially places dental teams and community pharmacists in an ideal position to target patients for risk assessment and health screening, especially for those who may not visit their GP regularly.
Many pharmacies already successfully offer screening programmes for a variety of conditions. This may be an opportunity to broaden the scope of this service further and given that opinions of stakeholders are comparable across the settings assessed and screening can be performed to good effect in pharmacy settings, it may be of benefit to explore this concept further in dental settings.
Unanswered questions and future research
The reported study has shown that key stakeholders are in broad support of greater utilisation of allied professionals in the early risk assessment and detection of NCDs. Further work is needed to determine feasibility of implementation of these principles and to establish whether the opinions translate into uptake of the service by patients and the public. It is also important to determine whether long-term intervention by allied professionals’ results in improved outcomes in patient care and whether that also conveys any health economic benefits. Furthermore, consideration must be given to how such a service would be funded as it is unlikely that healthcare professionals will undertake this risk assessment under existing funding arrangements. Therefore, health economic analysis will need to be undertaken to determine the cost savings to the NHS, or wider society and whether these savings can be used to fund the risk assessment. Another option may be exploring patients’ willingness to pay for such risk assessment. Future exploratory work to determine whether allied healthcare professionals would be willing or able to conduct such methods of targeted early detection of NCDs within existing funding arrangements must be considered. Likewise, whether patients would be willing to pay an additional fee or contribution for such a service would need to be determined.
Conclusion
The four key players in the NCD global challenge are CVD, respiratory disease, diabetes and cancer. It has been established that allied healthcare professionals may have access to different cohorts of the population and those members of society less likely to visit a GP may be more likely to visit a community pharmacy or general dentist. It is therefore possible that if dentists and pharmacists have access to patients who are not using healthcare services elsewhere, they may be ideally placed to risk assess, and where appropriate offer preventative advice and test for NCDs. In the dental clinic, this may be especially pertinent where those NCDs share common risk factors and associations with primary dental diseases, such as periodontal disease, for which prevention strategies are already established.
Increased collaboration between general medical practitioners and allied healthcare professionals to stem the rise in NCDs, by assisting with early identification, provision of preventative advice and where appropriate, targeted risk-based identification of disease, may prove beneficial to patients’ general health and oral health alike. The results from this survey suggest that all stakeholders appear to be largely supportive of potential risk identification services for NCDs, especially diabetes and CVD in both dental and pharmacy settings.
References
Footnotes
Contributor Substantial contributions to the conception or design of the work or the acquisition, analysis or interpretation of data for the work: ZY, PS, AY, ZJ, ILC and TD. Drafting the work or revising it critically for important intellectual content: ZY, PS, ZJ, TD and ILC. Final approval of the version to be published: ILC. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. ZY.
Funding This work was supported by a grant from the Oral and Dental Research Trust. NIHR Portfolio number (CPMS ID 32232).
Competing interests ILC acts as a consultant to Oral Health Innovations who provide PreViser and DEPPA risk and disease assessment technologies for dental practices. The other authors of this article have no conflicts of interest to declare.
Patient consent Obtained.
Ethics approval All surveys were approved by the National Research Ethics Service (NRES 16/YH/0293) or the Ethics Committee of the University of Birmingham (RG_15–195).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Pseudonymised individual participant data, used in preparation for this manuscript, will be available immediately following publication for a period of 36 months. This will be available to researchers providing a methodologically sound proposal and for the purposes of achieving the aims of that proposal only. Proposals should be directed to the corresponding author. To gain access, researchers will need to sign a data access agreement.