Article Text

Abstract
Objectives Although alcohol screening is an essential requirement of level I trauma centre accreditation, actual rates of compliance with mandatory alcohol testing in trauma patients are seldom reported. Our objective was to determine the prevalence of blood alcohol concentration (BAC) testing in patients requiring trauma team activation (TTA) for whom blood alcohol testing was mandatory, and to elucidate patient-level, injury-level and system-level factors associated with BAC testing.
Design Retrospective cohort study.
Setting Tertiary trauma centre in Halifax, Canada.
Participants 2306 trauma patients who required activation of the trauma team.
Primary outcome measure The primary outcome was the rate of BAC testing among TTA patients. Trends in BAC testing over time and across patient and injury characteristics were described. Multivariable logistic regression examined patient-level, injury-level and system-level factors associated with testing.
Results Overall, 61% of TTA patients received BAC testing despite existence of a mandatory testing protocol. Rates of BAC testing rose steadily over the study period from 33% in 2000 to 85% in 2010. Testing varied considerably across patient-level, injury-level and system-level characteristics. Key factors associated with testing were male gender, younger age, lower Injury Severity Score, scene Glasgow Coma Scale score <9, direct transport to hospital and presentation between midnight and 09:00 hours, or on the weekend.
Conclusions At this tertiary trauma centre with a policy of empirical alcohol testing for TTA patients, BAC testing rates varied significantly over the 11-year study period and distinct factors were associated with alcohol testing in TTA patients.
- trauma management
- alcohol testing
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This observational study was performed at a Canadian tertiary trauma centre with a mandatory clinical policy of testing for alcohol in all patients who require activation of the trauma team.
We examined how often this mandatory clinical policy of alcohol testing in trauma team activation patients was adhered to over an 11-year study period.
Our analyses included characteristics of patients, their injuries and the trauma care system to determine the independent association of these factors with alcohol testing.
Reasons for non-adherence to the mandatory alcohol testing policy and the improvement thereof were not specifically analysed in this study.
This investigation was limited to the major trauma population at a single centre; thus, our inferences may not be generalisable to other patient populations or institutions.
Introduction
Misuse of alcohol is associated with various problems (physical, social, psychological) and responsible for lost lives, considerable morbidity and significant healthcare costs.1 Alcohol use disorder is regularly seen in hospitals and trauma centres, and is associated with traumatic injury (intentional and unintentional) and death.2 Emergency department (ED) patients have an over-representation of at-risk drinkers with high weekly consumption or heavy episodic drinking.3 Moreover, alcohol-related ED visits predict future problem drinking, alcohol-impaired driving, trauma recidivism and premature death.4 5
Hospitals and trauma centres are often the initial point of contact for patients with alcohol problems, and have a key role in reducing future alcohol-related injuries through brief intervention and/or other treatment programmes as part of trauma care.6 7 Routine alcohol screening and brief intervention (SBI) programmes in trauma centres are well established, but not universal.8 A survey of ED directors at level I and II trauma centres found only 15% had formal SBI policies.9 Alcohol SBI in EDs or trauma centres is effective at reducing alcohol consumption,10 11 impaired driving,12 13 and injury recidivism.14 Blood alcohol concentration (BAC) levels can be readily obtained at presentation or admission when blood is drawn for other diagnostic tests,8 or for assessment of alcohol and its effect on the patient’s presenting condition and injuries (eg, altered level of consciousness, hypotension).15
Collectively, evidence supports the development and implementation of policy statements and clinical practice guidelines to promote routine testing of trauma patients for drug and alcohol intoxication.16 The American College of Surgeons on Trauma requires level I trauma centres in the USA to test for alcohol disorders.17 This was also an expectation of the Trauma Association of Canada, the body responsible for accrediting trauma centres in Canada until 2014. More recently, Accreditation Canada developed criteria for level I trauma centres which included an expectation that alcohol SBI programmes are in place for major trauma patients.18
Despite evidence and associated policies, routine testing is not standard practice in most EDs and trauma centres.19 20 Almost all trauma centres have the capacity to perform BAC measurements and many institutions have adopted a policy of routine testing, yet uniform testing remains elusive.16 Lack of proper screening makes it unlikely that patients who misuse alcohol will be identified and receive appropriate interventions and/or treatment. As such, it is important to gain a better understanding of patient-level, injury-level and system-level characteristics associated with routine alcohol testing. Understanding these factors will assist with improving the screening process by identifying gaps—both in terms of patient populations and system-level issues—that are preventing optimal alcohol testing.
The clinical policy (in effect for the entire study period) at the Queen Elizabeth II Health Sciences Centre (QEII HSC), a tertiary trauma centre in Halifax, Nova Scotia, is that the trauma team leader (TTL) is to direct and ensure routine collection of empiric blood alcohol levels for each trauma team activation (TTA) patient (as per protocol and preprinted orders). The purpose of this study was to examine BAC testing in major trauma cases requiring TTA at the QEII HSC over an 11-year period. Our objectives were to determine the prevalence of BAC testing and assess for patient-level, injury-level and system-level characteristics associated with blood alcohol testing.
Methods
Study setting and population
This study was conducted at the QEII HSC (Halifax, NS), which is an adult (≥16 years) tertiary trauma centre similar to a level I US trauma centre.21 Official policy at the QEII HSC is to test all TTA patients for quantitative presence of alcohol. Test results are used for associated clinical management issues, and to initiate intervention and treatment for patients identified to have substance abuse problems. These test results are not used for forensic reasons.
In Nova Scotia, staff of the provincial trauma programme (Trauma Nova Scotia (TNS)) routinely collect detailed information on all major trauma patients; these data are stored in the Nova Scotia Trauma Registry (NSTR). The NSTR has quality control procedures in place to ensure accurate and complete data entry, and has been used in other peer-reviewed publications.21–25 The TNS definition of ‘major trauma’ includes any injury with an Injury Severity Score (ISS) ≥12 and an appropriate International Classification of Disease External Cause of Injury Code, as well as penetrating injury cases with an ISS ≥9 and any TTAs regardless of ISS. Criteria for TTA include physiological, anatomical, mechanistic and logistic considerations.26 All adult TTA cases recorded in the NSTR over an 11-year period (2000–2010) were eligible for this study. There were no changes to the criteria for TTA during this time. This study was performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines for reporting observational studies.27
Patients and public involvement
Patients or public were not involved in this study.
Variables
Data on all TTAs during the study period were collected from the NSTR. The primary outcome of interest was whether patients had BAC testing performed, which was dichotomised as ‘tested’ or ‘not tested’ for blood alcohol. ‘Tested’ was defined as obtaining a BAC level that was sent to laboratory for analysis at the time of TTA, patient assessment and resuscitation.
Independent variables consisted of patient-level, injury-level and system-level characteristics, along with year variables. Patient-level characteristics included gender, age, health status (co-morbidities), presence of shock (systolic blood pressure <90 mm Hg), respiratory failure (intubation) and patient outcome (length of stay, discharged alive). Injury-level characteristics included ISS, Glasgow Coma Scale (GCS) score at the scene and on ED arrival, injury type (blunt, penetrating, burn), injury mechanism (falls, motor vehicle crash, assault, other (poisoning, self-harm)), presence of head injury, severe traumatic brain injury (Abbreviated Injury Scale (AIS) Head score ≥3) and time from injury to treatment in the ED. System-level characteristics included presence of a surgeon versus non-surgeon as TTL,22 transport to ED (transfer vs direct arrival, ie, no intermediate hospital involvement), transport mode (ambulance vs air transport (helicopter and fixed-wing aircraft)), admission to operating room (OR) directly from ED and whether the patient was exposed to any OR procedures. In addition, we captured time of day, day of week and season, and we examined the yearly trend in testing over the study period.
Data and statistical analysis
Data analysis followed two stages. First, we described characteristics (patient-level, injury-level and system-level) of TTAs, stratified by whether blood alcohol was tested or not. Χ2 tests for categorical variables and Student’s t-tests with 95% CIs for continuous variables (age, length of stay, ISS) were used to note differences between patient populations across all characteristics (p<0.05). The provincial trauma system in Nova Scotia was accredited in 2005, and we compared testing rates between pre-accreditation (2000–2005) and post-accreditation (2006–2010) periods. Variables with missing values were noted as such.
Second, we conducted multivariable logistic regression to examine patient-level, injury-level and system-level characteristics associated with BAC testing. All variables significant at p<0.20 were initially included in the regression model. The variable ‘trauma system accreditation’ was derived from the variable ‘years’ (phi coefficient=1.0, p=0.000) and therefore not included in the multivariable analysis. Characteristics were entered into the model as categorical variables with the exception of age and ISS which were entered as continuous variables. Backward stepwise regression was used to select variables that remained in the model; variables were tested for significance using the likelihood ratio test and non-significant (p≥0.05) variables were removed. The Hosmer-Lemeshow goodness-of-fit test was used to assess the appropriateness of the logistic models. As a sensitivity analysis, we included missing data as a level in the regression model.
The rank-based non-parametric Kendall tau-b method was applied to detect any trend in BAC testing between 2000 and 2010. The null hypothesis was no trend in BAC testing over time; the alternate hypothesis was an increasing or decreasing trend in testing over the study period. The sign of the coefficient indicates the direction of the relationship, and its absolute value indicates the strength with larger absolute values indicating stronger relationships. All data analysis was performed using SPSS V.23 (IBM),28 and Stata V.11.1.29
Results
Patient-level, injury-level and system-level characteristics
A total of 2306 cases included were included in the analysis. table 1 compares patient-level and injury-level characteristics between TTA cases screened for alcohol and those not tested.
Descriptive statistics for patient-level and injury-level characteristics all trauma team activations in Nova Scotia, 2000–2010, by blood alcohol screening (n=2306)
Patients tested for alcohol had lower mean age (36.9 years vs 43.1 years; p<0.001) and were more often male (81% vs 71%; p<0.001) and discharged alive (93% vs 88%; p=0.001) compared with those not tested. A larger proportion of cases without alcohol testing involved patients with higher ISS (20.3 vs 19.0; p=0.023). We also observed a greater proportion of tested patients had a severe GCS score at the scene or on ED arrival, or a severe head injury (AIS Head ≥3).
Regarding system-level characteristics (table 2), BAC testing was more frequent in patients transported directly from the scene to the ED (57% vs 47%; p<0.001), those arriving by emergency medical services (EMS) ground transport (72% vs 65%; p<0.001) and when a TTL surgeon was present (31% vs 26%; p=0.017). Testing was less frequent in cases arriving by EMS air (28% vs 35%; p<0.001) and in patients admitted to OR from the ED (25% vs 29%; p=0.031) or who went to OR at any time for a procedure (55% vs 61%; p=0.002). Rates of alcohol testing were significantly higher in the postaccreditation period compared with the preaccreditation period.
Descriptive statistics for system-level measures for all trauma team activations in Nova Scotia, 2000–2010, by blood alcohol screening (n=2306)
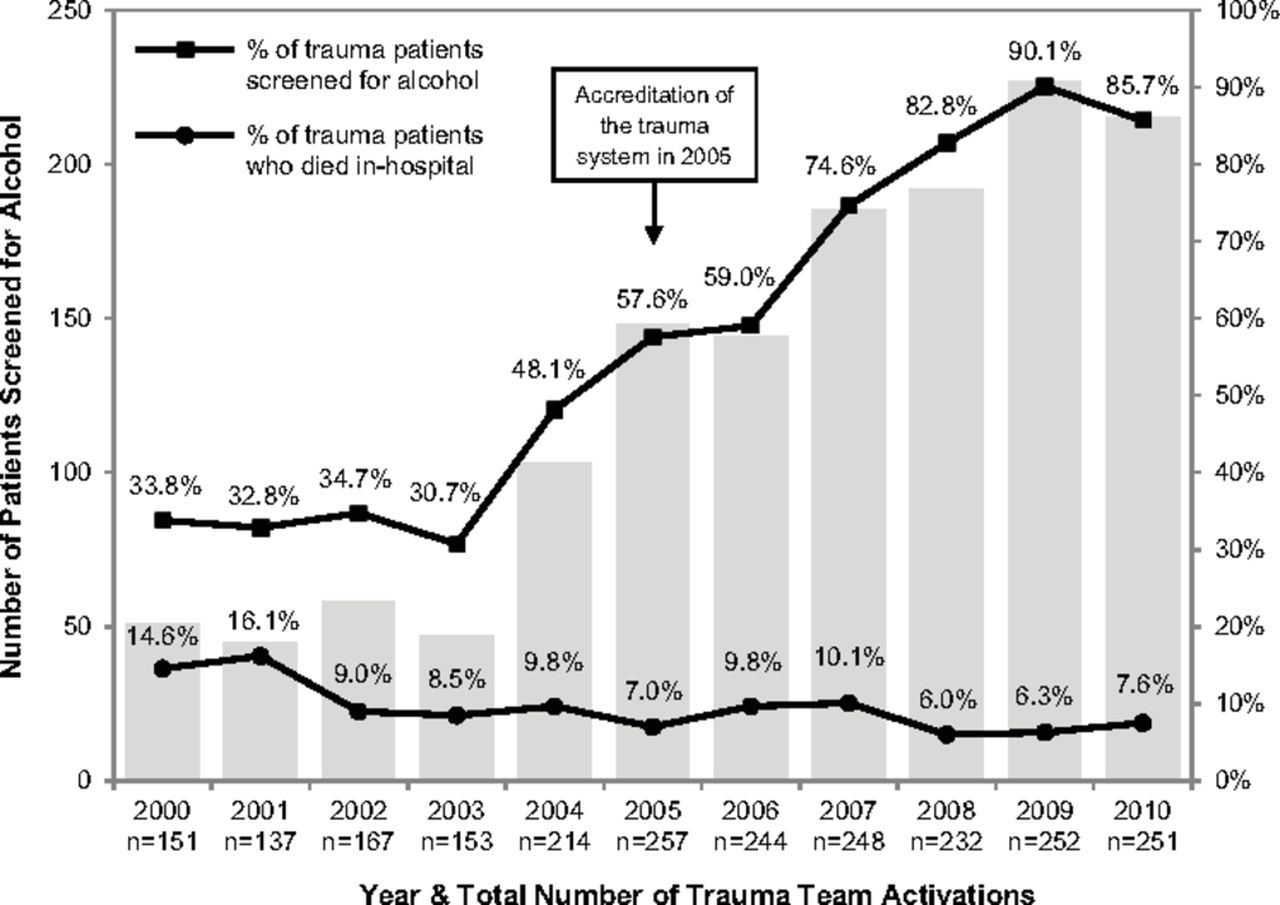
Overall, 61% of the sample received a blood alcohol test, though a clear trend to testing was observed. In 2000, 34% of TTA patients were tested, a rate that increased to 90% in 2009 and 86% in 2010 (figure 1). Still, there remained 10%–17% of TTA patients who were not screened between 2008 and 2010 despite the existence of a mandatory clinical policy to test every TTA patient for alcohol. Time-trend analysis yielded a Kendall tau-b correlation coefficient for BAC testing incidence of 0.36 (p<0.001), indicating a significant increase in testing rates over the course of the study. figure 1 also shows mortality for TTA patients during the study. Although there appears to be a trend over time toward lower mortality in these patients, it is likely that other factors in addition to BAC testing contributed to this trend.
{kind=link}
Blood alcohol testing and mortality in trauma team activation patients, 2000–2010.
Predictors of BAC testing in TTA patients
The results of multivariable logistic regression are reported in table 3.
Multivariable logistic regression of blood alcohol testing on patient-level, injury-level and system-level measures
The following variables were included in the final model: age, gender, injury mechanism, ISS, scene GCS, transport, time of day, day of week, year, shock, intubation and discharged alive. Results of the Hosmer-Lemeshow test indicated a good fit for the model (p=0.305).
Alcohol testing was more likely in patients who were younger (OR 0.99; 95% CI 0.98 to 0.99) and male (OR 2.00; 95% CI 1.54 to 2.61). With increasing ISS, the likelihood of testing decreased (OR 0.99; 95% CI 0.98 to 1.00). The likelihood of BAC testing was greater for patients requiring intubation versus those not intubated (OR 1.63; 95% CI 1.20 to 2.21). Patients in shock were less likely to be tested compared with patients not in shock (OR 0.46; 95% CI 0.27 to 0.78). In terms of transportation, BAC testing was more likely in patients transported directed from the scene to the ED (OR 1.63; 95% CI 1.29 to 2.06). Finally, there were significant temporal effects with higher odds of testing on the weekend compared with the first three weekdays (OR 1.51; 95% CI 1.17 to 1.96), and during early morning hours compared with the rest of the day. Data on shock and scene GCS were missing for some patients; these were included in a sensitivity analysis (online supplementary table 1). With inclusion of this missing data, ISS and shock were no longer associated with BAC testing, while being discharged alive and sustaining an ‘other’ injury mechanism were associated.
Supplementary file 1
Discussion
The findings of this study demonstrate that not all TTA patients underwent alcohol testing despite the existence of a mandatory clinical policy. Thus, having a requirement for alcohol testing in policy format does not reflect clinical implementation. There were significant differences between patients tested for alcohol and those not tested. Patient-level and system-level factors were most strongly associated with testing, particularly gender, age, direct transport from scene to ED and time of arrival. In spite of the steady and significant increase in frequency of alcohol testing at this tertiary trauma centre over the 11-year study period, we continued to identify untested TTA patients.
This study was a retrospective analysis and thus subject to the known limitations of retrospective data collection. Although data were collected from a prospective population-based registry, information was unknown or incomplete in some cases. This investigation was limited to the major trauma population at a single centre; thus, our inferences may not be generalisable to other patient populations or institutions. Furthermore, the reasons for non-adherence to the mandatory BAC testing policy and the improvement thereof were not specifically analysed in this study. Based on the experience of one study author (RG) who is a TTL at the QEII HSC, the most common reason why a TTA patient might not have their BAC tested would be a personnel issue where a member of the healthcare team is unfamiliar with the protocol or the need to perform a BAC test. Regular educational initiatives targeting all staff involved in the care and management of the TTA patient may help improve awareness of the mandatory BAC testing policy. It is important to note that there is a balance between mandatory BAC testing and potentially unnecessary blood draws. There may be competing priorities (eg, urgent need to perform resuscitation or an operative procedure), and the cost of unnecessary testing must also be considered. In Canada, there exists a national campaign (Choosing Wisely Canada) that engages healthcare professionals and voices the need to reduce unnecessary tests and treatments in healthcare.30
Alcohol screening rates vary due to local differences in populations, clinical policies and institutional procedures. MacLeod and Hungerford performed a systematic review of alcohol-related visits to trauma centres in the USA and found screening rates ranged from 31% to 99%.31 Others have reported rates of 16.6% in Taiwan,3247% in the USA,33 and 49% in Australia.34 Studies of alcohol screening in TTA patients observed rates of 85% and 87%,35 36 which are comparable to the rates we observed toward the end of the study period. A recent study of all trauma patients in the Canadian province of Alberta found screening rates rose from 51% in 2001 to 61% in 2010, reaching as high as 69% in 2008.37 Similar to our findings, patients were more likely to be screened if they were younger, male, severely injured or an emergency admission to hospital (compared with a direct admission).
The findings of the present study raise two important issues worth further investigation. First, the patterns observed in blood alcohol testing by patient characteristics raise concerns about potential bias among trauma centre staff. This finding suggests that staff members may be making assumptions as to which patients are more likely to be impaired by alcohol. This is not to say that such assumptions are entirely unjust, as there exists a considerable body of evidence demonstrating that younger males account for the majority of patients found to have positive blood alcohol levels on presentation to the ED.16 37–39 Surprisingly, injury mechanism was not significant in our study in terms of BAC testing, though more severe injuries were tested more often. Second, and equally important, certain system-level factors increased the likelihood of blood alcohol testing. In particular, direct transport from the scene to the ED appears to matter, with testing rates higher among those who arrived directly rather than being transferred from an intermediate hospital. Similarly, while seasonal effects were not evident, testing occurred more consistently in patients who presented late at night and in the early morning hours, and on weekends compared with other times of the week. Again, this may represent assumptions made by staff members during times when excessive consumption is more likely to lead to problem outcomes and a higher volume of alcohol-impaired patients.
Given the extent of non-testing in our study, potential systematic biases suggest missed opportunities for intervention and treatment. For instance, while testing was more likely late at night and in the early morning, patterns in problematic alcohol consumption (particularly among chronic, high-risk users most in need of intervention) do not follow the typical peaks and valleys observed among acute alcohol consumers in the general population.40 As such, vigilant testing at all hours and across all patient types represents the best approach for reaching both moderate and high-risk drinkers. Recognition of potential systematic biases is an important step towards improving overall testing rates and provides a focal point for additional continuing education. Systematic biases in testing represent clearly modifiable features of hospital care and secondary prevention. Ongoing efforts are necessary to encourage and educate clinical staff about alcohol testing, with a focus on patients who are systematically missed. Comprehensive alcohol testing in the ED remains important for clinical care as a means to identify patients requiring intervention, consultation and treatment, and as a method for continuing regional and national surveillance of the burden of alcohol.41
Conclusions
At this tertiary trauma centre with a policy of empiric BAC testing for TTAs, actual testing rates varied significantly over the 11-year study period and specific factors (patient-level, injury-level and system-level characteristics) were associated with testing in this population. These results should inform clinical testing policies to help improve empiric testing and optimise the reach of appropriate, evidence-based interventions for patients with alcohol-related problems.
References
Footnotes
Contributors MA and JMT conceived the research questions and designed the study. SAK performed data collection. ME, NK, MA and SAK performed analysis and drafted the manuscript. ME, NK, RSG, SAK, JMT and MA contributed to data interpretation, critical review and revisions of the manuscript for important intellectual content. All authors approved the final version of the submitted manuscript and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Nova Scotia Health Authority Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.