Article Text

Abstract
Objective To understand how a new patient education programme for renal recipients becomes situated and adapted when implemented in daily hospital teaching practice. The analysis focuses in particular on how principles of individual tailoring and patient involvement are adapted.
Design Ethnographic observation study. 19 teaching sessions were observed, resulting in 35 pages of data written observation notes.
Setting A Norwegian University hospital. The study included the transplantation (TX) post, the medical post and the outpatient clinic.
Participants 10 newly transplanted patients receiving the education programme, and 13 nurses trained in the new programme participated in the study.
Results We observed that the nurses attempted to implement the programme’s core principles of individual tailoring and patient involvement as intended, but that patients found it difficult to formulate their knowledge needs and interest. Patients and nurses developed an approach to individual tailoring and patient involvement, which used knowledge about the patients’ life and experiences as basis for translating generalised knowledge into knowledge that is individualised and meaningful for the patient. The individual tailoring was however also limited, as the nurses balanced between responsibilities for the programme’s principles of individual adaption and patient involvement at the one hand, and responsibilities of safety and economy from a health systems perspective on the other hand.
Conclusion Individual tailoring is observed to be a comprehensive practice which includes verbal, practical and emotional involvement with the patient’s life world. This extends the notion and practice of individual tailoring as selecting among predefined, generalised knowledge based on an initial mapping of the patients’ knowledge. While the adaptions to individual tailoring could have been seen as inaccurate implementation, in-depth analyses discloses that the extended approach to individual tailoring is in fact what retains the programme’s core principles in the implementation context.
- qualitative research
- implementation
- patient education
- individual tailoring
- knowledge translation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Ethnographic observations of naturally occurring teaching sessions allows for in-depth investigation of complex adaptions to the implementation context.
While the study’s small scale limits generalisation, the study discloses important issues in patient education, individual tailoring and implementation that could be further investigated.
Few participants had additional conditions or special needs, which perhaps prevent understanding about particular needs in groups with additional conditions or challenges.
Introduction
About 300 patients per year receive kidney transplantations in Norway. Patients who go through kidney transplantation have to acquire knowledge about immunosuppressive medication, graft surveillance and the benefit of specific lifestyle behaviour in order to reduce rejection episodes, graft loss and the negative consequences of lifelong immunosuppressive medication.1 2 The benefits of individually tailoring patient education have been increasingly documented.3–5 Much research has focused on improving patients’ adherence to medication,6 7 whereas questions regarding what kind of knowledge patients achieve by individual tailoring in patient education have received less attention.
In a recent publication in BMJ Open, Poland et al 8 describe that individual tailoring help patients build ‘individually relevant knowledge of their condition’, which in turn ‘support a situated understanding’. This clarifies that individual tailoring is not merely a question of individually adapted education, but that patients need to develop individualised knowledge. It does however not address the question of how individuality of knowledge is achieved in patient education. To understand how patients achieve such individualised knowledge is however crucial in order to advance patient education to meet patients’ need for individual knowledge.
This article presents an ethnographic observation study of the implementation of a new patient education programme for newly transplanted renal recipients. The question that we investigate is how the new patient education programme is situated and adapted when implemented in the daily teaching practice in the hospital. Our results focus in particular on how the new programmes’ principles of individual tailoring and patient involvement are practised.
The main difference between the new and old patient education programme was that the new programme emphasised stronger individual tailoring, patient involvement and an extended number of training sessions. A randomised controlled trial (RCT) was conducted prior to implementation, which identified that the customised patient education programme increased levels of knowledge, compliance and self-efficacy, and higher quality of life-scores compared with the control group which received standard care.9
An intervention developed in an experimental context cannot be transferred to a real-world setting without contextual adaption.10 Such adaption is not necessarily a threat to accurate implementation, as often assumed, but a precondition for implementation.11 However, implementation also presupposes critical awareness about how this adaption comes about and elements that are added to or removed from the ‘original’ intervention through the implementation process.12 We used ethnographic observation to investigate adaptions in the implementation of the new programme. The method is well suited to study the implementation of multifaceted interventions such as patient education programmes as it allows for detailed descriptions and in depth studies of naturally occurring interaction.13
Background
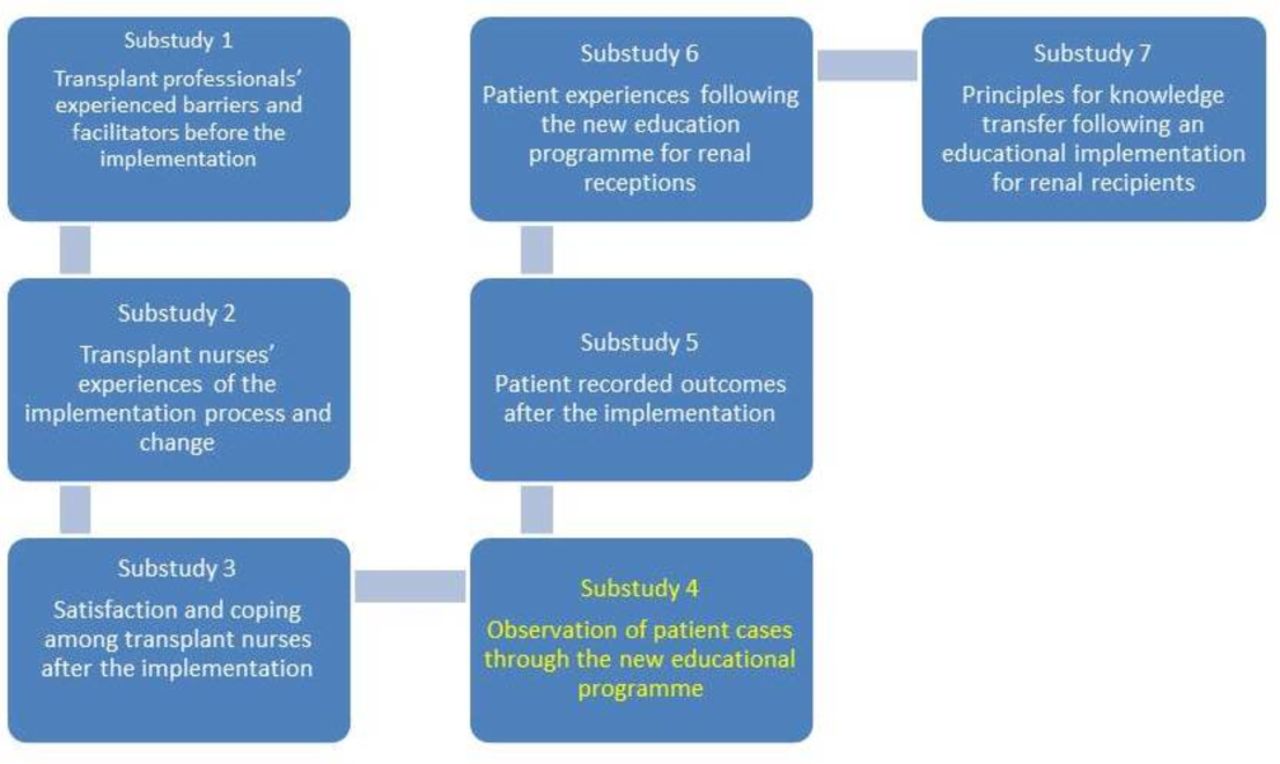
The work reported here is a substudy outgoing from the evaluation project ‘Evaluating and monitoring evidence based implementation of a structured, tailored education programme for renal transplant recipients’. The overall goals of the evaluation project were to (1) improve the quality of patient education and (2) to understand and evaluate processes involved in the implementation, as well as changes in practice following the implementation of the intervention. The evaluation project included seven substudies which investigated both the preimplementation and postimplementation phase of the new education programme. The pre implementation phase addressed identification and analysis of the current situation and the development of an implementation plan regarding competence enhancement of the new patient education programme (substudies 1–3).14 15 The postimplementation phase focused on the delivery of the new patient education programme to the patients (substudies 4–7) and included both the perspectives of patients and staff (figure 1). The current paper presents substudy 4, which investigates how the programme becomes situated and adapted in the implementation context of individual teaching sessions with patients and nurses.
{kind=link}
Overview of the substudies in the research project. Evaluating and monitoring evidence-based implementation of a structured, tailored education programme for renal transplant recipients.14
The evaluation project was inspired by the FORmative Evalutation, Consultation and Systems Technique (FORECAST)framework,16 which is a formative evaluation framework for programme implementation and evaluation. Implementation is seen as a dynamic and two-way process, and continuous collaboration and mutual influence between the implementation teams and the project stakeholders are emphasised. The implementation process should be flexible, and feedback loops are used to secure continuous evaluation and adaption.
The new patient education programme
The new programme consisted of five one-to-one teaching sessions with a trained nurse, lasting about 40–60 min. Three different departments were involved: the TX post, the medical post and the outpatient clinic. The first two sessions were held at the TX post, and the first session was held during the first week after transplantation. Most patients were discharged directly to the outpatient clinic where three more sessions were held. Patients needing special care or more follow-up on medications and self-surveillance were admitted to the medical post and received additional sessions.
During the five sessions, essential information on the three knowledge areas of medication, rejection and lifestyle were provided. These areas were also covered in the standard written information handed out for all renal recipients post-transplant, which was used as a basic tool for the sessions. Under each of the predetermined themes, the content was contextualised and further detailed based on each patient’s needs and life situation. The patients also received a diary in which medications, temperature, fluid balance and urine was registered.
Development of the new education programme involved studies of educational theory, a review of previous research on patient education, knowledge about transplantations and clinical experience.1 17
Compared with previous education programmes used in the hospital, the new programme emphasised patient centring and individual adaption. In order to ensure individualisation of the knowledge, the method of ‘academic detailing’ was used. ‘Academic detailing’ is a strategy based on learning principles and includes identification of baseline knowledge and needs (measured by knowledge questions), definition of evident training areas, a skilled instructor, encouragement of active participation, repetition and elucidation of key areas and feedback on behaviour change.18
Methods
Study design
Ethnographic observation emphasises the collective aspects of human life and practices, and explores shared behaviour, customs and beliefs.19 It allows the researcher to investigate naturally occurring practices as they unfold in specific contexts,13 and provides thick descriptions of these practices, as well as the contextual circumstances that impinge on them. Ethnographic observation was thus a fruitful method for investigating in depth how the new programme was adapted and situated when encountering the implementation context.
Data collection
Observations
Ten patients were included in the study. Two or three (of five) sessions in each patient’s teaching programme were observed: one at the TX post, one at the medical post in cases where patients were admitted there and one at the outpatient clinic. We observed a maximum of three sessions per patient (table 1). All five sessions of the programme were observed at least once. Inclusion of 10 patients was considered sufficient to capture a detailed material containing variances and patterns in how the new programme was taught and received. Data collection ended as planned, as the material was considered providing in-depth insight into the implementation process and rich on relevant examples.
Number of observations per patient
A total of 19 teaching sessions were observed; 10 at the TX post, 1 at the medical post and 8 at the outpatient clinic.
Participants
Nurses
A total of 13 nurses were included: 1 male and 12 female. Eight worked at the TX post, one at the medical post and four at the outpatient clinic. One nurse had <1 year of experience working with renal recipients, five had 1–5 years, three had 6–10 years and four had >10 years of experience.
Patients
The TX nurses included patients in the study (table 2). Selection criteria was that the patients were not in need of a translator, and that the patient was fit enough to participate in regular teaching sessions. With these exceptions, all patients were asked. The nurses however remarked that patients with severe additional conditions were more likely to say no. As such, the material includes only a few patients who had additional conditions or needed special follow-up.
Included patients: sex and age
Observation strategy
The observations were conducted by a researcher (IL) with competence and experience in ethnographic observation and qualitative studies of communication of knowledge. Due to little knowledge about renal transplantation and the daily practice at the hospital, she visited each post for one or two whole days prior to observations. She also spent time at the departments between scheduled observations and took part in formal and informal gatherings, such as meetings and lunches. This was done to make the researcher more familiar with the daily practice at the departments, and to be available for nurses’ questions and to create an atmosphere of trust around the project.
Observations notes were written during and directly after observations, and contained description of situations, quotes and more theory-driven reflections and preliminary analysis. As the researcher was unfamiliar with the setting and content of the education programme, an open approach was emphasised in the earliest observations. In subsequent observations, key topics for further observations were identified and pursued. These observations specifically addressed issues like: nurses’ and patients’ definition of the sessions’ purpose, communication, structuring of the sessions, patient participation and communication of needs, as well as how material artefacts were involved in the sessions. The observations resulted in a total of 35 data written pages of observation notes.
Data analysis
Data analysis began shortly after data collection and involved several phases. The first phase involved detailed reading of the data and identification of topics for further analysis, guided by the research question of how the programme was adapted and situated during implementation in the clinic. Topics such as communication, knowledge, patient involvement and patient participation were addressed. Topics and quotes from the data were presented to the researcher group, and generated feedback which narrowed down topics for further analysis. In the second phase, two of the researchers (IL and EE) deepened the analyses by working with excerpts of the observation notes. Further discussions with the researcher group resulted in the identification of two main topics: 1) a widened concept of knowledge tailoring and 2) challenges and limitations for knowledge tailoring in daily practice.
Patient involvement
The project and research question was developed on basis of literature revision, discussions in the researcher group and clinical experience. A user representative from The Norwegian Association for Kidney patients and Organ transplanted took part in the discussions. Patients were not involved in the recruitment to and conduct of the study. Results will be disseminated to study participants through the journal published by The Norwegian Association for Kidney patients and Organ transplanted and through oral presentations.
Results
This study inquires how a new patient education programme becomes situated and adapted when implemented in the daily teaching practice in the hospital, with special attention on how the programme’s core principles of patient centredness and individual tailoring is practised. We find that when implemented, the programme’s approach to individual tailoring and patient involvement is insufficient. As a response, the nurses and patients develop an extended approach to individual tailoring and patient involvement, which includes the patient’s life world. We also find that the implementation context constrain individual tailoring and patient involvement.
Involving patients and mapping individual needs
As described, the new programme emphasised principles of individual tailoring and patient involvement. During the observed sessions, the nurses often attempted to map the patient’s needs by starting the conversation with a question. For example, the nurses often started the session by asking if the patient had read the written material that they had received, if he had any questions about it or if there was anything in particular that he wanted to talk about in the session. Opening sessions with a question was a method for mapping the patient’s knowledge, and it also reflected the new programme’s core principle of patient involvement, as it invited the patients to take ownership of the situation and of their own knowledge needs and interests.
The patients, however, were often acting reserved. Most patients confirmed that they had read or looked through the information material, but very few had any follow-up questions or particular interests. Many were silent and acting expectantly, seemingly waiting for the nurses’ initiative. That is, despite the nurses’ attempts to map the patients’ needs by inviting them to take an active patient role in the situation, it seemed it was often difficult for the patients to respond as intended. In turn, it became difficult for the nurses to structure the session based on an initial mapping of the patients’ knowledge. Consequently, in many of the observed sessions, the nurses had to find an alternative approach to the teaching sessions, which was often observed to use the written material; structuring the sessions by the three predetermined topics of medication, rejection and lifestyle.
Thus, in many observed sessions it was not possible to tailor the sessions as intended by the patients’ needs and knowledge. Instead, many sessions took a more standardised form, structured by the written material.
Including the patient’s life world
When patients refrained from taking an active, knowledge-seeking role in the sessions, it could be interpreted as a lack of knowledge or interest. Accordingly, when the nurses structured the sessions based on the standard written material, it could be seen as inaccuracy in implementation. However, when nurses started talking about the predefined topics, the patients would often respond with interest and follow-up questions. A pattern in our material was that their response was often explicitly related to their daily life at home, that is, one patient was particularly interested in the information about chickenpox, as he told the nurse that he had children at home who had not yet had chickenpox. Another patient was particularly interested in the information about medication and travelling, and told the nurse that he had a summer house in South Europe where he used to go with his children and grandchildren. This suggests that the patients’ difficulties of formulating knowledge interests or needs were not related to lack of such, but to difficulties in assessing and using the generalised information material as basis for identifying their own knowledge needs and interests.
We found that the nurses actively used the information they had acquired about the patients’ lives as a tool to individualise the generalised knowledge in the material. For example, a general advice in the information material was to exercise regularly to counteract weight gain and loss of bone density, which are known side effects of the immunosuppressant medication. This generalised knowledge was individualised by a nurse, based on her knowledge about the patient’s life at home: “You can take your dogs for an extra walk and make sure to get some extra exercise”. In another session, a nurse used her knowledge about the patient’s life to individualise the generalised knowledge about increased risk of skin cancer, asking the patient: “When you are on your boat, do you make sure that you use sunscreen?”
Nurses also attended to patients’ general condition, state of mind and personal style of communication. They adapted to the patients, for instance, by shortening the session if a patient seemed tired or unwell, or by actively tuning in to the patient’s way of communicating. For example, a nurse could lower her voice and tempo with a reserved patient, while acting more outgoing and humorous with another patient. The nurses also responded to patients’ knowledge interests or particular needs by making arrangements outside of the sessions, for instance, by offering to provide information material, or scheduling appointments with specialists or home care during visits at home on behalf of the patient.
Our data are rich on examples of how individual tailoring of the education programme involves a more complex and comprehensive practice than an initial mapping of the patient’s knowledge about the content of the education programme. Observation of the teaching sessions suggests that patient tailoring involves actively engaging with the patient’s life world. The term life world originates from phenomenology and refers to our horizon of experiences, which constitute the background on which all things appear meaningful.20 Applied here, the term illustrates how the patients and nurses use the patients’ daily life, work, family and interests, as well as the patients’ behaviour and communication as a primary frame of reference for individualising the education.
Limits to individual tailoring
In some observations, patients concluded that a certain part of the programme content was not relevant to them. For example, one of the patients, a young man, told the nurse that he was determined not to have children, and that information about precautions regarding reproduction was irrelevant for him. Several patients also commented that having lived with medication regimes for many years prior to the transplantation, they were already familiar with the importance of compliance, and did not need detailed instructions or repetition. A few patients explicitly opposed to certain parts of the information, like one patient who repeatedly said things like: “you need not be a rocketeer to understand that”, ‘that is self-explanatory’ or ‘that is unproblematic’.
In cases where patients told the nurses that they had existing knowledge, or that they felt some knowledge was irrelevant to them, the nurses would not easily accept this as sufficient basis for tailoring the session. For instance, in the case with the man not wanting children, the nurse first suggested that he might change his mind later on. When the patient denied this, the nurse insisted that the knowledge nonetheless could become useful in the future and that the patient should know about the precautions. A similar response was given to an underweight patient who had already explained to the nurse that she wanted to gain weight. The nurse gave the information about diet as usual, but added: “now, you are slim, so there is no concern, but you should know about it anyway”. When a patient found some of the information excessive or irrelevant, the nurses often responded with formulations like ‘repetition does not hurt’, or ‘it can become relevant in the future’. This may be interpreted as while the patients’ knowledge about their lack of knowledge was considered an important basis for tailoring, their knowledge about what they already know or did not need to know was not regarded as a sufficient basis for tailoring.
Discussion
Whereas the study includes a limited number of participants, it discloses important insights to further develop individual tailoring in patient education. The methodology enable in-depth studies of complexities in implementation and in individual tailoring in patient education settings.
The use of FORECAST and feedback loops provided continuous adaptation throughout the entire implementation process and awareness about individualised knowledge. Still, one might question whether the FORECAST framework fully captured the complexity of the implementation process. Although the model ensures continuous adaptation and modification of the intervention, it tends to presuppose that the knowledge to be implemented is a package that can be traced through the implementation ‘pipeline’ and to which the implementation process owes some kind of fidelity. Our results demonstrate that a more flexible framework is needed that considers knowledge as a process of continuous interaction, an –ing rather than a thing.
Previous research has shown that tailored patient education increases learning for patients with chronic conditions.5 9 The principle of individual tailoring suggests a process of developing individualised knowledge, which has been shown to be important for patients.8 Our results suggest that individual tailoring is enacted as a comprehensive practice, which entails actively engaging with the patients’ knowledge about their life and experiences in order to translate generalised knowledge into meaningful knowledge within the frame of the patient’s life world.
The new patient education programme in this study used academic detailing as an approach to secure individual tailoring and patient involvement. We observed that the nurses attempted to involve patients, and map knowledge needs by encouraging patients to define their own knowledge needs. However, in many cases the patients were not able to take the active role and articulate their own knowledge needs, which in turn left the nurses without a basis for further individualisation of the programme.
In a review of patient-reported barriers to shared decision making, Joseph-Williams et al 21 conclude that providing patients with knowledge is insufficient, and that patients must also be granted power by healthcare providers to enable them to take part in health-related decisions. Our results illustrate that the formulation of individualised knowledge seems to be crucial for the empowerment of patients. More precisely, it seems from our results that presenting patients to generalised knowledge of medication, transplant rejection and lifestyle does not help them identify their own knowledge needs. Relating the knowledge to their own life world however helps patients to articulate knowledge needs, and in turn to develop individualised knowledge about medication, transplant rejection and lifestyle.
Seeing the patient as part of the wider context that makes up the patients’ life world, would include the patients’ families, homes, work places and local society. The stories told by the patients often involved their closest family; that is, spouse, children and grandchildren. It has been shown that family members and other caregivers provide important support to patients with chronic conditions. This indicates that involving family in patient education might be beneficial. It may help the patients and their families to integrate knowledge about medication, rejection of graft and lifestyle in their daily life. Family involvement in patient education could also counteract caregivers’ feelings of being unprepared and having insufficient knowledge.22
While involving family could be valuable, it can also be practically challenging as the patients receive the programme while admitted to the hospital. A benefit of educating patients while admitted to the hospital is that it allows the nurses to observe the patients progress in learning the medical regime and the registration of body fluids. However, as illustrated in our results, development of individualised knowledge of how to live with the regimes required to keep the organ and maintain good health, seems to be related to the patients’ daily life outside of the hospital. Having the general knowledge of how to prepare medication and register body fluids might be a different kind of knowledge than the individualised knowledge needed to develop good habits and long-term adherence.
As such, patient education should seek to help patients identify possible situations in their daily lives where they may use and adapt the generalised knowledge provided by the information material. Moreover, as the individualised knowledge seem to be tied closely to experiences in the patients’ lives, it might be valuable if the education take place in, continue or become repeated when the patient has returned home and have gained experience in living their life with a transplanted organ.
When nurses limit individual tailoring, we see it as an act of balancing between responsibilities for correct implementation on the one hand, and for patient safety and health expenses on the other hand. That is, when they insist on teaching certain topics, although the patients find it irrelevant or unnecessary, they are prioritising statistical knowledge about risk for graft loss and other complications, as well as economic knowledge about the expenses of non-compliance and possible consequential complications over the patients’ own knowledge. Previous research have also identified that it may be challenging for patients with chronic disease to make their individual knowledge heard by healthcare personnel. Healthcare personnel’s reliance on biomedical, economic or statistical knowledge over the individual knowledge of the patient may be an important barrier to individual tailoring and patient involvement.22 23
Conclusion
Our results indicate that individual tailoring should help patients identify how and when generalised knowledge about medication, rejection and lifestyle is relevant in their daily life outside the hospital. As such, the observed practice extends the notion of individual tailoring as selecting topics based on an initial mapping of the patients’ knowledge of the generalised information.
It can be further asked if developing knowledge, that is, meaningful within the frame of their own life may help patients with maintaining the new regimes of medication and lifestyle in the transition to home, and thus improve long-term compliance. Another possible question to pursue is whether incorporating patients’ daily life and family into patient education programmes can contribute to individual tailoring.
While the approach to individual tailoring that was practised during implementation of the new patient education programme could have been understood as failed implementation, the ethnographic approach allowed for in-depth analyses which disclosed complex adaptions to the implementation context. As such, our study strengthen the argument that implementation processes should be studied with critical awareness about how adaptions to the intervention are made, and what causes them.10 11 23
Acknowledgments
The authors are grateful to the participants in this study who generously allowed us to observe the teaching sessions, and to the user representative from The Norwegian Association for Kidney patients and Organ transplanted who contributed in the project.
References
Footnotes
Contributors MHA, KHU, AW and EE designed and led the project. IL conducted observations, the first analysis of data and drafted the manuscript. All authors gave feedback on analysis and contributed to revise the manuscript.
Funding This research was funded by the University of Oslo, Oslo University Hospital and the University of Stavanger.
Competing interests None declared.
Patient consent Not required.
Ethics approval The study was assessed and approved by the Data Protection Office at Oslo University Hospital (2014/5573). All participants were informed about anonymity, confidentiality, publication and their right to withdraw from the study at any time without any consequences.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This is a qualitative study and therefore the data generated is not suitable for sharing beyond that contained within the report.