Article Text

Abstract
Objectives Neck pain is a significant condition that is second only to depression as a cause of years lived with disability worldwide. Thus, identifying and understanding effective treatment modalities for neck pain is of heightened importance. This systematic review aimed to investigate the effects of cupping on neck pain from the current literature.
Design Systematic review and meta-analysis of randomised controlled trials (RCTs).
Setting Nine databases, including Chinese, Korean and Japanese databases, were searched for data up to January 2018 with no restrictions on publication language.
Participants Patients with neck pain.
Interventions Cupping therapy as the sole or add-on intervention compared with no treatment or active controls.
Primary and secondary outcome measures Pain severity, functional disability and quality of life.
Results Eighteen RCTs were selected. Compared with the no intervention group, the cupping group exhibited significant reduction in pain (mean difference (MD) −2.42(95% CI −3.98 to −0.86)) and improvement in function (MD −4.34(95% CI −6.77 to −1.19)). Compared with the active control, the cupping group reported significant reduction in pain (p=0.0009) and significantly improved quality of life (p=0.001). The group that received control treatment with cupping therapy (add-on group) displayed significant pain reduction compared with the active control group (p=0.001). Of the 18 studies, only 8 reported occurrence of adverse events, which were mostly mild and temporary.
Conclusions Cupping was found to reduce neck pain in patients compared with no intervention or active control groups, or as an add-on treatment. Depending on the type of control group, cupping was also associated with significant improvement in terms of function and quality of life; however, due to the low quality of evidence of the included studies, definitive conclusions could not be drawn from this review. Future well-designed studies are needed to substantiate the effectiveness of cupping on neck pain.
PROSPERO registration number CRD42016047218.
- neck pain
- complementary therapies
- meta-analysis
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This systematic review investigated the effectiveness of cupping in treating pain, and placed no restrictions on publication language.
This study employed stringent inclusion and exclusion criteria, and nine databases were accordingly searched for randomised controlled trials.
The analysis addressed functional improvement, quality of life and safety of cupping, and risk of bias and levels of evidence.
The results of data synthesis may be limited due to the heterogeneity and low quality of evidence of selected studies.
Introduction
A recent WHO study of the 20 major causes of years lived with disability (YLD) from 2000 to 2012 worldwide reported that neck pain is the second leading cause of YLD.1 One study of patients in the Netherlands showed that neck pain was associated with 1% of total medical expenditure and 0.1% of gross domestic product, 77% of which comprised indirect medical expenses associated with absence from work or disability expenses.2 Prevalence of neck pain is directly associated with escalated medical costs and negative impact on productivity, potentially increasing long-term absences from work. The lifelong prevalence of neck pain in adults ranges from 14.2% to 71%, although this rate varies greatly across studies.3 Neck pain can easily progress to chronic conditions, with approximately 25% to 60% of patients developing chronic back or neck pain within the first year.4 Additionally, neck pain is reported to be most prevalent in high activity age groups, particularly individuals aged 35 to 49 years,5 and is also more common in women.3
Standard first-line therapy for neck pain can be largely divided into pharmacological and non-pharmacological therapies. Pharmacological treatment frequently involves use of acetaminophen and non-steroidal anti-inflammatory drugs (NSAIDs). However, acetaminophen and NSAIDs are known to increase risk of reduced liver function, liver failure and haemorrhagic gastritis,6 and side effects may be more common when these drugs are used long-term for chronic neck pain. For these reasons, many studies have investigated the clinical effectiveness of complementary medicine therapies, including acupuncture for chronic pain conditions.7
One type of complementary therapy that can be used for neck pain is cupping. Cupping is a physical treatment, typically used by acupuncturists and other complementary medicine therapists, that uses glass or plastic cups placed on the skin over a painful area or acupuncture point to create negative pressure through suction. The rationale for use of cupping is not yet fully understood; it is described as a detoxification process by which waste matter and toxins are removed, and as a harmonisation process for the imbalance of Qi, a traditional Chinese medicine term for ‘vital energy’.8 Cupping has been used globally for several thousand years, particularly in countries such as Egypt and China.8 Today, cupping is widely used as a holistic treatment in Europe for inpatient care and the prevention and treatment of various disorders, as well as for promotion of general health.9 In South Korea, cupping is a popular treatment, and is covered by national health insurance; in 2013 alone, insurance claims for cupping reached a total 215 billion Korean won.10
There are two types of cupping: dry and wet. Dry cupping is a technique in which cups are applied to the skin to create a vacuum for suction without drawing blood, whereas in wet cupping, blood is drawn with scarification before applying the cups for blood-letting. Cupping therapy is used for poststroke rehabilitation and hypertension, and has been reported to be effective for treating pain and musculoskeletal disorders.11 12 A systematic literature review published by Yuan et al in 2015 reviewed the effects of cupping on neck pain, reporting that cupping is effective for reducing pain and improving function.13 However, only articles published up to 2013 were included in that review, and as new clinical trials investigating cupping for neck pain have since been published, an updated systematic review on the topic is needed. Moreover, Yuan et al 13 restricted the publication language to include only English and Chinese language articles.
Therefore, the aim of this study was to assess current evidence of cupping for neck pain and better understand its effects on pain, function, quality of life (QoL) and safety through the review of randomised controlled trials (RCTs). To conduct a more extensive review, no restrictions were placed on publication language, and studies in English, Korean, Japanese and Chinese were included.
Methods
The protocol of this systematic literature review was registered in the PROSPERO international prospective register of systematic reviews (CRD42016047218). This review was performed and reported in adherence with the Preferred Reporting Items for Systematic Reviews and Meta Analyses.14
Literature search
Studies that used cupping as an intervention for neck pain were searched in the Ovid-Medline (1946 to January 2018), Ovid-EMBASE (1980 to January 2018), Ovid-Allied and Complementary Medicine (AMED) (1985 to December 2017) and the Cochrane Central Register of Controlled Trials up to 9 January 2018. The Chinese database China National Knowledge Infrastructure, Korean databases Oriental Medicine Advanced Searching Integrated System and National Discovery for Science Leaders and Japanese databases J-stage and ISHUSHI were also used. Search terms included a combination of Medical Subject Headings (MeSH) terms such as neck pain (eg, neck pain, cervical spondylosis, cervical radiculopathy, cervical disc herniation and myofascial pain syndrome) and cupping. Details of the search strategy are presented in online supplementary appendix 1. The publication language of study articles was not restricted.
Supplemental material
Study inclusion and exclusion
Two or more investigators (YJL, SK and/or SHL) independently selected articles for analysis from the searched articles. After excluding duplicate publications, titles and abstracts were reviewed to primarily screen for articles according to the inclusion and exclusion criteria. The full texts of these articles were then reviewed for secondary screening of articles per inclusion and exclusion criteria. Only RCTs were considered. Any disagreement in the study selection process was resolved by discussion, and when an agreement was not reached, a third investigator intervened to reach consensus. Study subjects included adult patients with neck pain, including neck pain with neuropathy, and the authors did not discriminate between acute and chronic phases of neck pain. However, post-traumatic pain caused by whiplash or sports injuries was excluded as the natural history of neck pain may differ in such cases. Furthermore, patients with myelopathy or cervical headache/vertigo without neck pain were also excluded. All types of cupping therapies were included without restriction regarding dry or wet cupping, and the type of cupping device was not limited. Control groups included patients who underwent usual care for neck pain, such as physical therapy, NSAIDs, heat pack therapy and acupuncture,15–17 as well as inactive controls, such as waiting lists or no intervention groups. The outcome variables assessing the effectiveness of cupping included pain intensity, neck disability indexes and QoL. Pain intensity was measured using the visual analogue scale (VAS), the McGill Pain Questionnaire and the Northwick Park Neck Pain Questionnaire (NPQ). The Neck Disability Index (NDI) was generally used to evaluate neck function disability. QoL was assessed using the 36-item Short-form (SF-36) and EuroQol-5 Dimension (EQ-5D) questionnaires. However, studies that did not use objective instruments and reported outcomes in terms of improvement rates without standards, and investigations that used instruments without confirmation of reliability and validity were excluded.
Risk of bias evaluation and data extraction
Risk of bias in the RCTs was assessed by seven categories according to the Cochrane Risk of Bias. Studies that used appropriate methods for each item and specified the methods in the text were considered to have low risk of bias; studies that did not perform the relevant item or used inappropriate methods were considered to have high risk of bias; and studies that did not mention specific methods or used ambiguous expressions to describe the methods for each item were considered to have an unclear risk of bias. Two or more investigators independently assessed all research data, and disagreements were resolved through discussion. When an agreement could not be reached, a third investigator intervened to reach consensus. Two reviewers independently read the full text of all articles and extracted data according to a predetermined format. Any disagreements were resolved by discussion between the two reviewers.
Data analysis
A meta-analysis was performed using quantitative data from each study to assess the effectiveness of cupping. The mean difference (MD) and 95% CIs were calculated using the Cochrane Collaboration software (Review Manager (RevMan) V.5.3, Copenhagen: The Nordic Cochrane Centre) for Windows (Microsoft Corporation, Redmond, Washington, USA). Heterogeneity across studies was assessed using the χ2 test with a significance level of p<0.10 and I2 statistics. When heterogeneity was statistically significant, the cause of heterogeneity was analysed through subgroup analysis. Sensitivity analyses were also conducted to test the robustness of results by determining the impact of a single study on overall results. If statistical heterogeneity was found, sensitivity analyses (by eliminating one study at a time) were performed to explore possible reasons for the heterogeneity. A random effects model was applied, and publication bias was not assessed when the number of studies in the group was <10.
Quality of evidence
The quality of evidence for each outcome was assessed in accordance with the Grading of Recommendations, Assessment, Development and Evaluation (GRADE). Quality of evidence was classified into high, moderate, low and very low. To determine the quality of evidence, the following domains were assessed according to the standards suggested by the GRADE group: risk of bias, imprecision, inconsistency, indirectness, publication bias, large magnitude of effect, dose–response and confounding.18
Patient and public involvement
Patients and public were not involved in the development of the research question and outcome measures or design of this study, or recruitment to and conduct of the study as a systematic review and meta-analysis. There are no plans for the results to be disseminated directly to study participants.
Results
Search results
A total of 541 articles were retrieved, including 86 from Ovid-Medline, 137 from Ovid-EMBASE, 19 from Ovid-AMED, 43 from the Cochrane Library, 193 from a Chinese database, 47 from Korean databases and 16 from Japanese databases. Following the first and second rounds of screening, a total of 18 articles were selected for review. The search results are shown in figure 1.

PRISMA flow diagram of the literature search. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta Analyses.
Features of the included studies
A total of 18 studies were analysed in two separate analyses19–36: direct comparison of the cupping (sole) and control groups; and an add-on analysis comparing the control with cupping group with the control only group. Two studies used three groups; 15 studies were included in the sole analysis while five studies were included in the add-on analysis.
Seven19 21 23 26–28 34 of the 18 studies used wet cupping while 11 studies used dry cupping. The frequency of cupping therapy varied greatly. Two studies performed only one round of therapy, and four conducted two to four rounds. The majority of studies conducted >10 rounds of therapy because most patients who were treated had neck pain with radiculopathy or chronic neck pain. The region of administration was typically the upper shoulder and neck area, and cupping was primarily administered to Ashi or other proximal acupoints. As these studies mainly treated pain, most presented pain scores in the form of VAS scores; disability was presented in NDI scores, while QoL was mostly reflected in responses to the EQ-5D and SF-36 questionnaires. The features of each study are presented in table 1.
Characteristics of the included studies
Risk of bias assessment
Random sequence
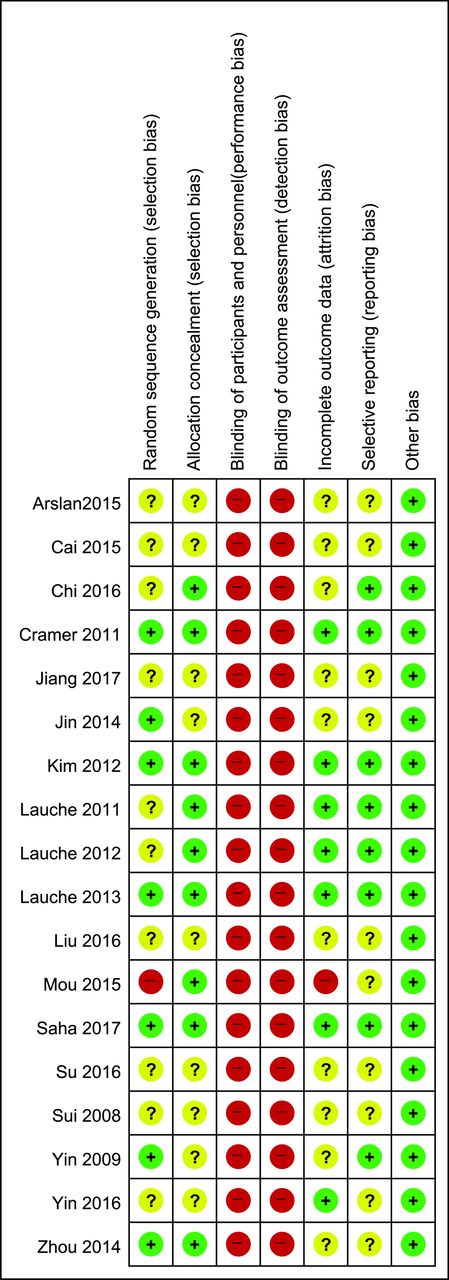
Seven of the 18 studies20 22–25 27 28 were assessed to have low risk of bias as they randomly allocated the subjects using a table of random numbers. One study did not specify the randomisation method, and the group sizes notably varied, that is, 68, 56 and 59; this study was thus assessed to have high risk of bias.26 The remaining 10 studies, however, only mentioned randomly assigning subjects without specifying the method used for randomisation; thus, these studies were assessed to have an unclear risk of bias. The results are shown in figure 2.

Risk of bias in the included studies, as assessed using the Cochrane Collaboration’s risk of bias tool. +, high risk of bias; ?, unclear risk of bias; -, low risk of bias.
Allocation concealment
Nine20 22 24–26 28–31 studies concealed allocation using a sealed envelope, and thus were considered to have low risk of bias. The remaining studies were determined to be unclear as they did not describe the method of allocation concealment used.
Blinding
Control groups were either waiting list controls or active controls. Although efforts have been made to develop a sham version of cupping,37 blinding is difficult given that sham cupping is not often used. Chi et al 29 described single blinding; however, it was difficult to assess whether blinding was actually implemented. Hence, all studies were considered to not have blinded their investigators and participants. With regard to the blinding of participants and medical personnel, all studies were considered to have high risk of bias. Similarly, blinding of outcome assessors could not be performed in most studies as many used VAS for pain measurement and patient-reported outcomes. Blinding of outcome assessors would have been made feasible if the studies had used physician-reported outcomes or other outcome variables measured by the examiner; however, such studies were found lacking. Therefore, all studies were considered to have high risk of bias.
Incomplete outcome data
Seven20 22 24 25 27 30 31 studies reported the number of excluded and withdrawn participants, and the number of participants included for final analysis. It was decided that the number of withdrawn participants and the reasons for withdrawal were not a cause of bias; therefore, these studies were considered to have low risk of bias. One study was regarded to possess a high risk of bias as 33 participants from the intervention group and 27 from the control group dropped out after only one session of treatment.26 The remaining studies were determined to be unclear for not mentioning the number of participants who withdrew or were excluded.
Selective reporting
Ten20 22 24 25 27 29–31 of the 18 studies were determined to have unclear risk of bias regarding selective reporting as they did not describe adverse events (AEs) nor did they register the trial protocols. The remaining eight studies were found to have reported all outcome variables initially planned to be investigated, and thus were determined to have low risk of bias.
Other biases
All studies were assessed to have low risk of other biases.
Analysis
Cupping versus no treatment
Pain
Five studies were included in the meta-analysis.20 29–32 Compared with the no intervention group, the cupping group reported significant reduction in pain with an MD of −2.42 (95% CI −3.98 to −0.86). Considerable heterogeneity was observed (I2=93%; p<0.00001 (χ2 test)); however, the study by Chi et al 29 showed a statistically outlying effect size; a sensitivity analysis was conducted with the study omitted, and resulted in an MD of −1.48 (95% CI −1.86 to −1.10; I2=0%; p=0.57) with the heterogeneity resolved.
Disability
Three studies were included in the analysis.20 30 31 Results revealed that the cupping group reported significant functional improvement compared with the no intervention group with an MD of −4.34 (95% CI −6.77 to −1.91; I2=6%; p=0.35).
Quality of life
Three studies were included in the analysis,20 30 31 and results showed that the cupping group indicated significant improvement in the mental component summary of SF-36, with an MD of 5.32 (95% CI 0.83 to 9.80; I2=32%; p=0.23). No statistical significance was found in terms of the physical component summary of SF-36 with an MD of 2.46 (95% CI −0.36 to 5.29) (figure 3).

Forest plots demonstrating the effect of cupping as the sole intervention versus no treatment on neck pain.
Cupping versus active control
Pain
Ten studies were included in the analysis.21–28 34 35 Of these 10 studies, 9 reported the outcome in VAS, while one study reported NPQ scores.21 In analysis of the nine studies, the cupping group exhibited significant reduction in pain with an MD of −0.89 (95% CI −1.42 to −0.37; p=0.0009) compared with the control group. The χ2 test, however, revealed some heterogeneity (p<0.00001; I2=88%). In order to resolve the heterogeneity, studies were analysed separately depending on the type of cupping: either wet (with scarification) or dry. Meta-analysis of three studies conducted with dry cupping indicated an MD of −1.50 (95% CI −2.28 to −0.72; I2=28%; p=0.25). On the other hand, analysis of studies with wet cupping showed an MD of −0.70 (95% CI −1.32 to −0.07; I2=92%; p<0.00001) with unresolved heterogeneity. Omission of the study by Zhou28—which had a notably large effect size—resulted in an MD of −0.49 (95% CI −0.78 to −0.20) with I2=-35%, p=0.19, implying that the heterogeneity was considerably resolved. The single study that reported outcomes with NPQ indicated an MD of 3.59 (95% CI 2.02 to 5.16), suggesting that cupping significantly decreased pain compared with the control.
Disability
Four studies were included in the analysis.22 24–26 Compared with the control, the cupping group demonstrated functional improvement, with an MD of −4.36 (95% CI −8.67 to −0.04; p=0.05), but not to a statistically significant degree, and substantial heterogeneity was identified (I2=62%; p=0.05).
Quality of life
Two studies were included in this analysis.22 25 Compared with the control, the cupping group reported significant improvement in the physical component summary of SF-36, with an MD of 5.44 (95% CI 2.09 to 8.78; p=0.001). However, statistically significant differences were not found for the mental component summary of SF-36 with an MD of 0.44 (95% CI −4.05 to 4.93) (figure 4). The study by Kim et al reported EQ-5D outcomes as median values, and therefore inclusion for meta-analysis was not feasible. In this study, the cupping group and control reported identical median values of 0.91, suggesting no statistical difference.

Forest plots demonstrating the effect of cupping as the sole intervention versus active control on neck pain.
Cupping with active control versus active control (add-on)
Pain
Five studies were included in the analysis.19 26 33 35 36 Adding cupping therapy to the treatment administered in the control group led to significant reduction in pain, with an MD of −0.87 (95% CI −1.14 to −0.61; p<0.00001).
Disability
Only one study reported a disability-related outcome,26 and the effect on disability was not significant, with an MD of 3.61 (95% CI −3.93 to 11.15; p=0.35). Heterogeneity was not identified (I2=19%; p=0.29) (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots demonstrating the effect of cupping as an add-on intervention on neck pain.
Safety of cupping
Ten of the 18 studies included in the final analysis did not address safety, while eight studies did. First, Kim et al 24 reported skin laceration (n=1), whole body itching (n=1), pain at the cupping sites (n=1) and generalised body ache (n=1) in four patients in the cupping group; however, the study reported that the symptoms were mild and resolved within a few days. Lauche et al 31 reported one case of pain during the procedure itself in addition to tension headache, migraine, tinnitus and wound healing itches; however, all side effects were mild and temporary. Chi et al 29 reported two cases of mild low back pain due to the seated position in the cupping group. Lauche et al 25 reported muscular tension (n=1), increased pain (n=1) and prolapsed intervertebral disc (n=1). While prolapsed intervertebral disc should be regarded as a severe event, the original authors stated that a causal relationship was unlikely. Lauche et al 30 reported tingling sensation in the hands and arms (n=1), strain/pain at the treated area (n=2), strain/pain in the general neck region (n=1), slight headache (n=1), tiredness (n=1), shivering attack (n=1) and blurred vision (n=1). Lauche et al 30 reported that all symptoms subsided within 4 hours, and that the causal relationship with cupping was unclear. Yin et al 27 reported one case of delayed wound healing due to wet cupping. Cramer et al 22 reported muscle soreness (n=2), minor haematoma (n=1) and increased neck pain for 1 hour to 5 hours (n=2). In the study by Saha et al,20 two participants complained of headache that resolved within 1 hour. One participant suffered upper back pain, which subsided within days, and one participant reported slight dizziness. Although one case of lipoma was identified during the trial, it did not have any causal relationship with cupping, as reported by the authors.
Levels of evidence
The qualityof evidence for each analysis is shown in table 2. In the waiting list comparison, the quality of evidence for the outcomes of pain, QoL and disability was assessed to be low to very low due to concerns regarding risk of bias, imprecision and inconsistency. In the active control comparison, the quality of evidence for pain and QoL was low due to risk of bias and imprecision, and that for disability was assessed to be very low due to risk of bias, imprecision and unexplained heterogeneity. In the add-on comparison between the active control and active control with cupping groups, the quality of evidence for pain in the dry cupping add-on group was low due to risk of bias and unexplained heterogeneity. The quality of evidence for pain outcomes was very low. The quality of evidence for disability outcomes in the add-on groups was low due to risk of bias and imprecision (table 2).
Meta-analysis of outcomes and level of evidence
Discussion
The present study aimed to assess the evidence supporting the effectiveness of cupping for neck pain through a comprehensive systematic literature review. We performed a systematic and inclusive search in non-Asian and Asian databases, including those based in China, Korea and Japan, where cupping is popular and widely used. Eighteen articles were selected and analysed according to the type of control group used. When compared with inactive controls, cupping significantly reduced pain, and improved function and QoL. However, the heterogeneity between studies was quite high in terms of pain reduction, and the quality of evidence was lowered as a consequence. As one study, by Chi et al,29 reported a considerably large effect size, the heterogeneity was resolved when this study was omitted in the sensitivity analysis. Although in most studies the quality of evidence was found to be low to very low, the marked pain reduction and improvement in function and QoL found to be associated with cupping may be clinically relevant. When compared with active controls, the cupping group exhibited significant reduction in pain but no significant differences in functional improvement. Analysis in pain outcomes found an MD of −0.89 (95% CI −1.42 to −0.37); however, heterogeneity was high and subgroup analysis was thus performed. Effect sizes were similar across studies using dry cupping but varied greatly across studies using wet cupping; omission of the study by Zhou et al 28 resolved the heterogeneity. Additional analyses are needed to clarify whether the differences between studies can be attributed to different types of wet cupping procedures or whether other sociopsychological factors were involved. Wet cupping involves drawing blood before cupping, and, despite being accepted in some cultures, may not be tolerated in others. Furthermore, the intensity of the procedure and amount of bleeding may also have affected study outcomes, which may have further contributed to the varying effect sizes. Alternatively, the type and frequency of procedures and patient pain severity could contribute to varying effect sizes.
When used to compliment existing treatments, cupping was found to significantly reduce pain, with an MD of −0.87 (95% CI −1.14 to −0.61). However, in addition to statistical significance, the effect size of a treatment should be assessed for clinical significance. Based on four studies of cupping, Lauche et al 38 proposed the minimal clinically important difference (MCID) of VAS to be −8 (−0.8 of a 10-point scale), the NDI to be −3 and the physical component summary of SF-36 to be +5.1. From the current meta-analysis, cupping exhibited an MD of −2.42 compared with the waiting list control, −0.89 compared with the active control and −0.87 as an add-on treatment, which all surpasses the above criteria for the MCID of VAS. With regard to NDI, cupping indicated an MD of between −4.34 and −4.36, depending on the type of control, which also meets the MCID criteria. For the physical component summary, however, cupping failed to display a treatment effect larger than MCID. In contrast, cupping showed an effect size exceeding MCID when compared with the active control, which calls for further investigation.
Cupping has been used for several thousand years in such diverse regions as early Egypt and China.8 In traditional Chinese medicine, cupping is widely used to eliminate stagnated Qi and Blood, and facilitate circulation.39 Since ancient times, cupping has been considered to be effective in the local treatment of areas of inflammation.40 A previous review analysing the reported mechanism of cupping suggested that the positive effects of cupping are the result of a haemodynamic mechanism facilitating muscle function, as demonstrated by the reduction of deoxy-haemoglobin and elevated oxy-haemoglobin levels in muscle areas treated with cupping.41 Other studies have suggested that cupping involves a mechanism for removing oxidative stress,42 and produces therapeutic effects through diffuse noxious inhibitory control43; this would contribute to the alleviation of pain.
For these reasons, a growing number of clinical trials are investigating the effects of cupping on pain and various disease symptoms. Through the analysis of 135 RCTs on cupping, Cao et al 44 reported that clinical trials of wet cupping have been conducted in association with various disorders such as herpes zoster, facial paralysis, cough/dyspnoea and acne. A more recent systematic review investigated cupping in relation to overall disease45; however, although the analysis included some articles pertaining to neck pain, it did not focus on the condition. In another systematic literature review on the efficacy of cupping for lower back pain, cupping was found to lead to significant reductions in pain and improvement of function.13 46 Only one previous review has specifically evaluated the effect of cupping on neck pain, but that review was published in 2013 and analysed only five trials.13 Therefore, the results of the present study, which included 18 RCTs and did not limit inclusion by language, provide greater clinical relevance and implications.
However, this study has several limitations. One significant shortcoming is that only some studies reported issues related to safety. Although severe AEs were not found in association with cupping in the studies that reported side effects, many studies did not report side effects at all. A systematic review investigating the side effects of cupping reported that the most common side effect was scar formation, and there have been some previously reported cases of severe side effects.47 However, adverse reactions to cupping may vary according to the proficiency of the practitioner, type of procedure and disinfection and sterilisation processes implemented during the treatment procedure.47 Certain severe AEs, such as infection, may be preventable as their occurrence can be directly associated with the education, training, experience and proficiency of therapists. Another limitation was the low or very low quality of evidence for all outcomes; this low quality of evidence was primarily caused by risk of bias and unexplained heterogeneity between studies. Additionally, many selected studies did not maintain rigorous standards or procedures regarding allocation and blinding. Furthermore, the outcomes included for analysis in this study were all patient-reported outcomes (ie, pain, disability, QoL), and none of the included studies were designed to assess the placebo effect of cupping. It is possible that the results may have been influenced by the fact that all outcome measures were patient-reported and the lack of blinding. Moreover, all of the included studies, with the exception of a study published by Su et al in 2016,33 were conducted only in patients with chronic neck pain. Whether the therapeutic effect of cupping is dependent on the clinical characteristics (acute vs. chronic) of neck pain remains to be elucidated. Finally, many of the included studies had small sample sizes.
Nevertheless, cupping may be an important and cost-effective therapy for the treatment of neck pain. For example, Lauche et al 25 performed a clinical trial on home-based cupping. Due to the increased use of computers and smartphones around the world, the prevalence of neck pain is rising steadily,48 and this type of pain can often develop into chronic pain. Thus, this study is meaningful in that it evaluates a non-invasive, simple and effective treatment modality for patients with chronic pain.
Conclusion
The current results suggest that cupping may be effective for patients with neck pain in terms of reducing pain and improving function and QoL, when compared with no treatment or active controls. The level of evidence for the findings of the included studies, however, was found to be low or very low, thus preventing strong conclusions from being drawn for the effectiveness of this treatment. Although this study did not identify notable AEs in the articles reviewed, cupping is not without side effects, and further well-designed, large-scale studies employing standardised procedures are needed to thoroughly examine potential adverse effects. Furthermore, wet cupping requires rigorous education and training on hygiene and precautions, as it entails a blood-letting process. Although definite conclusions cannot be drawn from this study, cupping appears to be a potentially effective and safe therapy for neck pain.
References
Footnotes
Contributors SK, M-RK, I-HH and YJL designed the study. SK, S-HL and YJL conducted the systematic search. SK, M-RK and YJL assessed the literature for inclusion and extracted the data. JL, J-SS and IHH monitored data collection. E-JK, D-SH, JL, J-SS and IHH interpreted the data. SK, M-RK, I-HH,and YJL wrote the draft; S-HL, E-JK, D-SH, JL and J-SS critically revised the manuscript. All authors have read and approved the final version.
Funding This study was supported by the Traditional Korean Medicine R&D Program funded by the Ministry of Health & Welfare through the Korea Health Industry Development Institute (KHIDI) (HB16C0035).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.