Article Text

Abstract
Introduction Liver cirrhosis affects health-related quality of life (HRQoL) even in its early stages. Morbidity is especially high when the disease decompensates and self-care actions become essential. Nurse involvement in secondary prevention in other chronic diseases has contributed to better symptom control, less need of inpatient care and improved HRQoL. In order to evaluate the impact of nurse involvement in the follow-up of patients with liver cirrhosis, we decided to compare structured nurse-led clinics, inspired by Dorothea Orem’s nursing theory and motivational strategies, with a group of patients receiving standard care. The primary outcome is HRQoL and the secondary outcomes are quality of care, visits to outpatient clinics or hospitals, disease progress and health literacy.
Methods and analysis This is a pragmatic, multicentre randomised controlled study conducted at six Swedish hepatology departments. Eligible patients are adults with diagnosed cirrhosis of the liver (n=500). Participants are randomised into either an intervention with nurse-led follow-up group or into a standard of care group. Recruitment started in November 2016 and is expected to proceed until 2020. Primary outcomes are physical and mental HRQoL measured by RAND-36 at enrolment, after 1 and 2 years.
Ethics and dissemination The study is ethically approved by the Regional Ethical Review Board in Uppsala. The results shall be disseminated in international conferences and peer-reviewed articles.
Trial registration number NCT02957253; Pre-results.
- liver cirrhosis
- nurse-led clinic
- health-related quality Of life
- qualituy of care
- economics
- nursing
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This pragmatic multicentre randomised controlled study design enables evaluation of a nurse-led clinic intervention in patients with liver cirrhosis in the real-life context.
All nurses involved in the study are proficient in the field of liver diseases, having a holistic understanding of the situation of liver cirrhosis.
The generic health-related quality of life instrument RAND-36 is used as a Swedish version of a liver-specific instrument is currently unavailable.
There is a risk of unwittingly transferring the intervention to the control group. This is counteracted by the multicentre design and will shorten the time for recruitment of participants.
Introduction
The incidence of liver cirrhosis in Sweden is approximately 14 per 100 000 citizens each year.1 It is a disease with high mortality as well as high morbidity, affecting patient’s health-related quality of life (HRQoL). Fatigue and depression are already frequent during the early, compensated, phase of liver cirrhosis and are believed to impair HRQoL by affecting the patient’s social life.2 HRQoL is further impaired in the decompensated patients, when symptoms of ascites, hepatic encephalopathy (HE) or variceal haemorrhage occur.3 4
In the compensated stages, lifestyle changes are important to prevent or delay disease progression. While in the decompensated phase, customised lifestyle changes and self-care become essential in the management of the disease.5 Unstructured follow-up in outpatient settings causes frequent readmissions due to the reappearance of complications of cirrhosis. The reason may be drug-related side effects, for example, diuretics, non-adherence to self-care or medical treatment. One-third of these episodes are said to be preventable with closer follow-up in an outpatient setting.6 7
Motivating patients for self-care activities is essential in nursing care. For this, Orem’s theory of nursing,8 consisting of the three theories: self-care, self-care deficit and the nursing system may be applied. This theory guides nurses to identify and support patients to enter self-care for better symptom control and improved health.8–10 In liver cirrhosis, management of patients with liver cirrhosis is traditionally taken care of by physicians, while nurse-led clinics are still rare. However, previous studies on liver cirrhosis, nurse-led clinics have suggested that nurse-led clinics will contribute to better patient concordance with physician recommendations11–13 and medical treatment,11 12 with positive effects on patients HRQoL.12 Furthermore, there are indications that nurse-led clinics increase the quality of care by increasing the number of patients treated according to medical healthcare guidelines.12 Finally, the patients have reported a high degree of satisfaction by nursing care in such outpatient settings.12 14 Despite these reports, the significance of adjunctive nurse-led clinic to standard care by physician in liver cirrhosis is unclear. Conversely, in chronic heart failure, nurse-led care is established and proved equally effective as traditional care by the physician within outpatient settings.15 The holistic and person-centred approaches by the nurse, including motivational strategies, have been shown to be crucial in the secondary prevention of chronic heart disease, reducing the need for inpatient care and to increase HRQoL.16 17 Hence, the experience from nurse-led clinics in chronic heart disease is likely to provide guidance regarding content, methods and necessary skills in the set-up of nurse-led clinics within the field of liver cirrhosis.
The aim with the present study is to compare HRQoL in patients with liver cirrhosis receiving either adjunctive nursing care based on Orem’s nursing theory or standard care only in outpatient settings.
Methods and analysis
The protocol follows the statement of Standard Protocol Items: Recommendations for Interventional Trials 2013,18 for study protocol and Template for Intervention Dscription and Replication (TIDieR).19 .
Study design
The study has a pragmatic, multicentre randomised controlled comparative design.
Study arms
Patients in the intervention group obtain structured visits to nurse-led clinics depending on the severity of the disease. The intervention is adjunctive, that is, the intervention is added to standard care. Patients in the control group get standard inpatient and outpatient care according to clinical routines.
Study sites
The study settings consist of six outpatient clinics at hepatology departments in Sweden, two county hospitals and four university hospitals. None of the clinics had structured nursing care for patients with liver cirrhosis at the beginning of the study. The six outpatient clinics serve a population of approximately 2 000 000 individuals, comprising about 20% of Sweden’s population.
Eligibility criteria
Diagnosis of liver cirrhosis is based on clinical investigation, laboratory findings, histology, MRI, computer tomography, ultrasound or elastography. Factors likely to strongly affect the primary variable due to other reasons than liver cirrhosis, that is, severe comorbidities and those unable to adhere to the study protocol, that is, persistent, overt HE, are excluded. Inclusion and exclusion criteria are presented in table 1.
Inclusion and exclusion criteria
Screening and recruitment of participants
Invitation letters are sent by intervention nurses (INs), offering oral information. Patients are invited to a screening visit to IN for baseline measurements. Those who meet inclusion criteria are registered. Patients, who agree to participate, hereafter denoted as participants, are randomised after giving informed consent. Newly diagnosed patients are recruited consecutively (figure 1). INs are responsible facilitators and consecutively follow participants.

Recruitment and randomisation of participants. CC, compensated control group; CI, compensated intervention group; DC, decompensated control group; DI, decompensated intervention group; LC, liver cirrhosis.
Randomisation
Computerised randomisation (Randomize.Net, Interrand, Ottawa, Canada) is performed at the screening visit with randomly mixed block sizes of 4, 6 and 8, stratified by study site and disease severity in terms of compensated or decompensated state (figure 1). Blinding of the randomisation sequence is applicable to all involved personnel; allocation will be 1:1. Baseline measurements are completed before randomisation. Further blinding is not possible in this study.
Description of the intervention
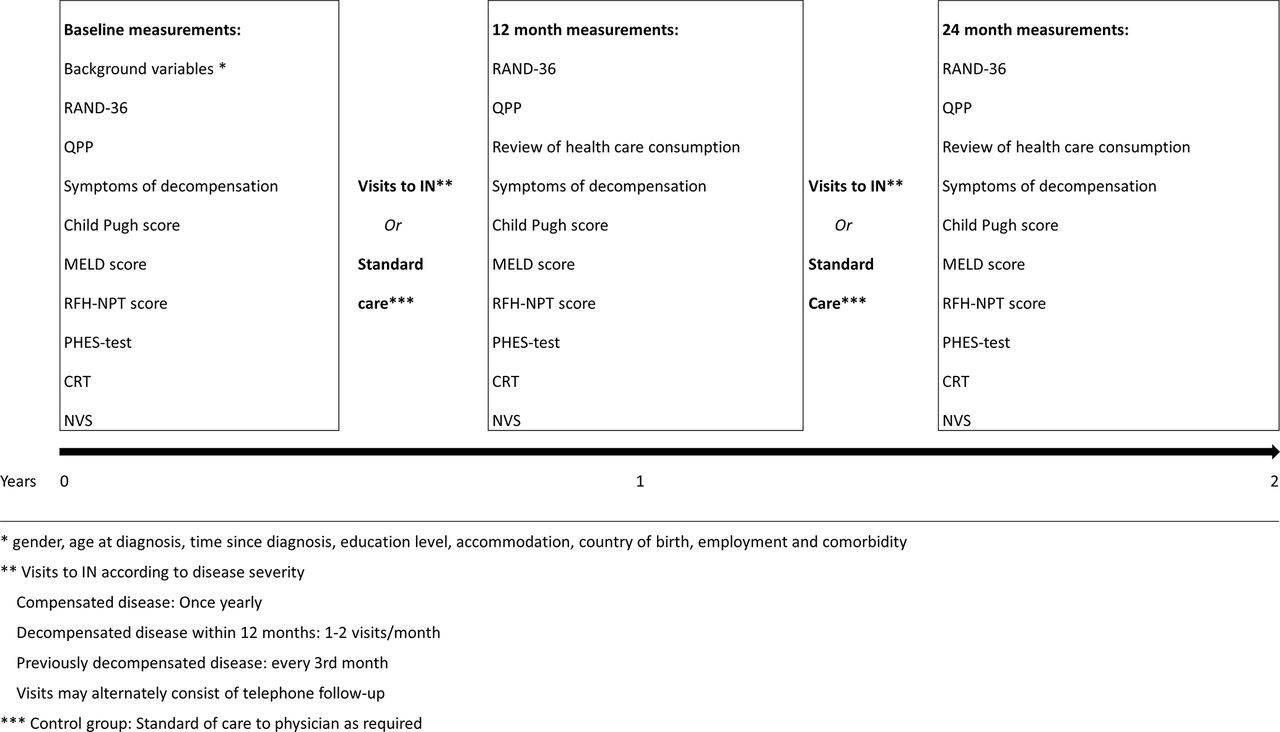
Participants in the intervention group offer scheduled individual visits to INs at the nurse-led clinic, in addition to visits to a physician according to clinical practice. Intervals between visits to the nurse-led clinic are varying from once yearly in compensated stable disease, up to two visit per month in decompensated disease (figure 2). The tailored frequency and content of visits are individualised to promote person-centred care (table 2).

Study measurements and intervention nurse visit interval. CRT, continuous reaction time; IN, intervention nurse; MELD, Model for End-Stage Liver Disease; NVS, Newest Vital Sign; PHES-test, psychometric HE score; QPP, quality of care from the patient’s perspective; RFH-NPT, Royal Free Hospital-Nutritional Prioritising Tool.
Description of the intervention
Participants in the control group will receive standard care by physicians within hepatology inpatient or outpatient clinics as required and a yearly follow-up for data collection by IN within the study (figure 2).
Each visit to INs contains assessment of disease severity to enable early action against disease progression and malnutrition (table 2). The intervention includes treatment and nursing care inspired by Dorothea Orem’s nursing theory.10 Further, motivational interviewing (MI),20 communication strategies will be used. Both Orem’s theory and MI implies that individuals have an intrinsic motivation to make appropriate choices, to promote health and prevent disease or to perform actions to counteract disease.10 20 The task of the IN is to assess the participants’ self-care needs and their ability to perform essential self-care in order to discover self-care deficits. To evoke participants’ motivation, INs listen and reflect on preparatory and mobilising change talk. In addition, INs give information adherent to MI techniques to facilitate participants understanding of actual self-care and medical treatment (figure 3). When applicable, INs offer next of kin instructions to help the participant achieve self-care.

{kind=link}
{kind=link}
{kind=link}
The four processes of motivational interviewing techniques. IN, intervention nurse; MI, motivational interviewing.
The areas of the intervention are: (1) monitoring risk factors for deterioration of the liver disease, (2) information and motivation to perform self-care and adhere to medical treatment, (3) nutrition assessment and support, (4) motivation of lifestyle changes essential for preventing or delaying disease progress and (5) psychosocial care. A booklet written by MH is handed to all INs describing these five areas converted into terms of Orem’s nursing theory.
One objective of INs’ use of MI is to promote engagement and increased collaboration between IN and participant via the MI spirit concepts: partnership, evocation, compassion and acceptance. Another objective is that INs evoke participants’ own motivation and explore patients’ own thoughts about a target behaviour when there is need for behavioural change. When participants express mobilising ‘change talk’,20 they are ready for the planning phase (figure 3). The intervention is individually tailored and INs’ activities depend on actual needs. An information booklet about liver cirrhosis is available to participants as a complement to oral information.
Standard care includes flexible visits or telephone follow-up by physicians, gastroscopies, ascites drainage, registered nurse telephone counselling by a nurse not participating in the study and inpatient care.
Intervention nurses
At each of the six clinics, 1–2 INs are involved in the intervention. All of these are registered nurses with a minimum of 2 years experience from hepatology inpatient or outpatient care. Implementation of the intervention and training of INs include a 6-hour seminar with a short description of MI and Orem theories followed by a 3-day training to perform MI. INs are also educated in pathophysiology of liver cirrhosis, nursing care according to presenting symptoms, study bias and study instruments. Scheduled tutorial group sessions to follow the intervention and MI practice will be due every 6 months for all INs during the study period.
Study piloting
A pilot of the intervention and patient questionnaire was performed in Falun from 2014 to 2015 with 26 participating patients. The aim was to define the actual size of the population available for the study and to assess the time and budget for the INs’ assignment.
Baseline sociodemographic data collection
Sociodemographic data collected at enrolment are presented in figure 2.
Primary outcome
Physical and mental HRQoL are the two main outcomes in the present study measured by RAND-36.21 RAND-36 consists of 36 category scale questions: the answer to each question ranges from 0 to 100, a higher value predicts better health. From the RAND-36 questionnaire, eight subscales are derived: (1) physical functioning, (2) role limitations caused by physical health problems, (3) pain, (4) energy/fatigue, (5) social functioning, (6) role limitations caused by emotional problems, (7) emotional well-being and (8) general health perception. Out of the eight subscales, two summary components are derived: Physical Component Summary (PCS) and Mental Component Summary (MCS).21 22 HRQoL measurements by the RAND-36 has high validity and reliability to identify differences in HRQoL over time within and compared with patient populations with different chronic diseases.22
Secondary outcomes
Patient’s perspective of quality of care due to a change in follow-up strategy: The questionnaire quality of care from the patient’s perspective (QPP)23 includes four dimensions: (1) medical-technical competence, (2) physical-technical conditions, (3) identity-orientated approach and (4) sociocultural atmosphere. Within each dimension, the participants first value their experience of the specific care aspects they have received ((1) totally agree, (2) agree in large part, (3) partly agree or (4) do not agree) and second, the importance of these aspects ((1) of greatest importance, (2) of great importance, (3) of some importance or (4) of little or no importance). The difference between the experienced care and the importance of each question is categorised as: excess of, balanced or lack of quality of care. A short form of QOP has been found valid and reliable.24 In the present study, participants receive a modified QPP 38-item questionnaire adjusted for patients with liver cirrhosis in outpatient care. The modification has been approved by the instrument developer. The questionnaire includes a variation of yes/no questions, category scales from 1 to 4 and open-ended questions.
Visits at outpatient clinics and admissions to hospital: Visits at outpatient clinics, number of admissions to hospitals and days of inpatient care at medical wards or intensive care units will be recorded as measures of healthcare consumption. In case of significant clinical outcomes, these data will later be used to perform a separate health economic analysis.
Disease progress
Child Pugh score25 includes five variables: serum albumin, serum bilirubin, prothrombin time, ascites and encephalopathy. Each variable grading from 1 to 3 and the total range is 5–15. A higher value means a more advanced disease. Three risk classes are derived: A=score 5–6, B=score 7–9 and C=score 10–15.26
The Model for End-Stage Liver Disease (MELD)27 predicts the 3-month mortality of patients with chronic end-stage liver disease. Based on laboratory findings, MELD is a valid and reliable instrument. The formula for MELD is constant for disease aetiology, the calculation score is: 9.57 x log e (creatinine mg/dL)+3.78 x log e (bilirubin mg/dL)+11.20 x log e (INR) +6.4. The score is continuous, ranging from 6 to 40, a high score predicts an increased risk of mortality within 3 months.28
The Royal Free Hospital-Nutritional Prioritising Tool (RFH-NPT)29 assesses the risk of malnutrition in liver cirrhosis as a predictor of disease deterioration and transplant-free survival. RFH-NPT correlates with deterioration of the liver disease and divides participants into low (0 points), medium (1 point) or high (2–7 points) risk groups for malnutrition. Parameters taken into account are nutritional history (unplanned weight loss, dietary intake body mass index) and current complications of liver cirrhosis (acute alcoholic hepatitis, ascites, general fluid overload). The instrument used in the study is a translation into Swedish from the English version. Validation of the translation is made in a research seminar within the research group.
Appearance of decompensation episodes (eg, ascites, overt HE and variceal bleed) is assessed at screening, after 12 months and after 24 months through medical records. HE is common in liver cirrhosis with a cumulative risk of 30%–40%.30 According to the West-Haven criteria,31 HE ranges from 0 to 4. Grades 0–1 mean subclinical or minimal symptoms (covert HE) and grades 2–4 mean severe neuropsychiatric symptoms (overt HE).30 Even milder grades of HE affect HRQoL.30 31 In the majority of cases, HE is treatable. Two psychometric tests in combination are recommended to detect covert HE.30 In this study, the psychometric HE score (PHES) and continuous reaction time (CRT) are used:
PHES consists of five-step paper and pencil tests,32 and includes a line drawing test, a serial dotting test and a digit symbol test to examine motor speed and accuracy, visual perception, visuospatial orientation, visual construction, concentration and attention. The test ends up with a score ranging from +6 to −18; −4 or less is the cut-off for a pathological result.
CRT33 is a 10 min test with auditory stimuli in headphones in intervals of every 2–6 s. It tests the reaction time and endurance by pushing a trigger button after a signal. Using the software EKHO reaction-time analysis tool, an index <1, 9 with 150 repetitions separate HE from other brain dysfunctions with a specificity of 0.92 and sensitivity of 0.93.
Health literacy (HL): involves a person’s ability to receive, process and understand basic medical information in making decisions and taking actions to promote health.34 The grade of HL may influence the intervention as it impacts the participants’ ability to understand and translate information into practice. The instrument Newest Vital Sign,35 which consists of six standardised questions about nutrition label information, is used. The questions is asked by INs, the correct answer scores 1 point, a score of 4 or above indicates no limits of HL and scores below 4 indicate limited HL. The instrument is translated from English to Swedish within another study (Health literacy among Swedish lung transplant recipients 1–5 years after transplantation, A Lennerling, A Kisch and A Forsberg, personal communication, 2018). Validation of the translation has been made in a research seminar within our research group and the risk of translation errors was judged to be low.
Participant flow through the study
Study time for each participant is 24 months (figure 2), after which participants in the intervention group may continue their follow-up at the nurse-led clinic if they want to. Participants in the control group may be offered follow-up at the nurse-led clinic after the end of study. Data collection and frequency of visits to INs are presented in figure 2. Reasons for withdrawal from the study are liver transplantation, move out of follow-up area or mortality. In case of two consecutive cancelled visits to an IN, a reminder will be sent, asking participants to contact INs for further participation in the study.
Data analysis and sample size calculation
Analysis includes the two primary variables in RAND-36: the PCS and the MCS. These components will be calculated based on weights from the oblique method,36 to avoid potential problems in interpretation due to negative weights. A repeated measurements model will be used for analysis of baseline, 12 and 24 months values of the component summary score. Treatment group, time (baseline, 12, 24 months) with interaction, and decompensated/compensated state will be fixed effects, while site will be a random effect in the model. The main contrast of interest to be estimated with this model is change from baseline to month 24 for both treatment groups. For the treatment group comparison, Bonferroni-Holm method using a corrected alpha=2.5% will be used to compensate for multiple testing of both PCS and MCS.
All tests will be two sided. For analyses of secondary variables, p values<0.05 are considered significant. Multiple imputation will be used for missing values.
For the power calculation, a SD of 9 points was used based on back-calculated residual variances from CIs for MCS.37 A change of 3–5 points is estimated to be a minimally clinically important difference and corresponds to an effect size of 0.09–0.28.22 It is argued that even smaller changes are important,38 and a change of 2.5 points is therefore considered to be potentially relevant for the power calculation. To ensure a power of 0.80 for the effect size of 2.5 points and a Bonferroni-corrected alpha level of 2.5%, the recommended sample size is 250 participants per treatment group, that is, 500 in total.39 With a calculated 33% non-inclusion rate, enrolment time is estimated from November 2016 to December 2020 or until 500 participants are included.
Patient involvement
Five patients contributed with comments on the questionnaire that resulted in changes in tree of the 78 questions. No patients were involved in study design, research question or recruitment. The results will be disseminated to the study participants in a short summary after the publication of the study.
Strengths and limitations
This randomised controlled trial in the field of nursing is a complex intervention with a pragmatic design and has a high risk of confounding factors. In a pragmatic design,40 the research aim is to reflect the clinical practice. Participant heterogeneity and a minimum of exclusion criteria are therefore allowed to a larger extent. The researcher must be aware of factors that may bias study results. In this study, participants may have other chronic diseases that may affect HRQoL. Patients with severe comorbidity are not included in this trial as it would have required a larger sample than available. A prolonged study of 5 years raises the risk of unwitting transfer of the intervention on to the control group when other personnel than INs start to develop skills included in the study protocol.17 To reduce this risk and preserve the ability to identify changes in HRQoL, study time is set to 4 years. Furthermore, six study sites are included in the study that aims to shorten the time for the study as well as reduce time for contamination of the control group. Six study sites, however, imply a risk of performance differences regarding the intervention and control group. In a forthcoming study, the context and mechanisms that may affect the results will be assessed in a process evaluation as described by Moore et al.41 To reduce bias in inclusion, participants in the control group offer a nurse-led clinic when study participation ends.
Although RAND-36 has proved sensitivity to changes in liver cirrhosis, a disease-specific instrument may be more nuanced. However, available disease-specific HRQoL instruments for liver cirrhosis are unfortunately not translated into Swedish. The former comparable generic instrument SF-3622 has been shown to be sensible for differences in HRQoL in populations of liver cirrhosis,.4 42
The MI experience may affect INs’ ability to use MI skills in conversations with participants. However, all INs in the present study are proficient or experts in nursing in the field of liver cirrhosis, having a holistic understanding of the situation of the disease. During the study, the INs will attend tutorial sessions twice a year to develop their skills in MI.
The occurrence of overt HE limits the enrolment of participants. Overt HE may have an impact on the ability to answer questionnaires used in the study. At enrolment, patients with covert HE are accepted. Before measurements at 12 and 24 months, HE tests will be repeated before the participants answer the questionnaires. Participants with overt HE will not be asked to answer the questionnaires, including RAND-36 and QPP, due to the risk of unreliable answers.
To our knowledge, this is the largest randomised controlled study evaluating nurse-led intervention in liver cirrhosis. The pragmatic design enables us to evaluate the effect of the intervention in the real-life context under which the study is performed. The results will hopefully contribute with important knowledge about nurse involvement in the care of patients with liver cirrhosis that can be applied in the routine clinical setting.
Dissemination
The study result will be published in peer-reviewed journals and presented at international conferences. The result will be used for education and competence development within the field. Study results are reported on the group level.
Acknowledgments
To Frank Miller for statistical support and to patient advisers for comments in development of the patient questionnaire.
References
Footnotes
Contributors MH has contributed to the design, implementation of the study and responsible for drafting the manuscript. DS has taken part in the design of the study and supervised MH in drafting the Manuscript, and has approved the final manuscript. AS has taken part in the design of the study and supervised MH in drafting the manuscript, and has approved the final manuscript. EK has taken part in the design of the study and supervised MH in drafting the Manuscript, and has approved the final manuscript. SL has taken part in the design of the study and supervised MH in drafting the manuscript, and has approved the final manuscript. FR has taken part in the design of the study and supervised MH in drafting the manuscript, and has approved the final manuscript.
Funding This work was supported by Ester Åsberg Lindberg foundation and Centre for Clinical Research in Dalarna. The CRT equipment was funded by Norgine.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study has been approved by the Regional Ethical Review Board in Uppsala (Dnr: 2016/146) and is performed according to the Declaration of Helsinki and to the Swedish Ethical Review Act.
Provenance and peer review Not commissioned; externally peer reviewed.