Article Text

Abstract
Objectives Moderation of alcohol consumption is included as a class I, level of evidence A recommendation in the current European guidelines for the management of hypertension. We investigated its awareness and self-reported implementation among European physicians across different specialties and workplaces.
Design and setting A cross-sectional survey study conducted in two annual German meetings (German Society of Cardiology and the German Society of Internal Medicine) and two annual European meetings (European Society of Hypertension and European Society Cardiology) in 2015.
Participants 1064 physicians attending the European meetings were interviewed including 52.1% cardiologists, 29.2% internists and 8.8% general practitioners.
Main outcome measures Physician screening of alcohol consumption, awareness and self-implementation of the recommendation of the current European guidelines about moderation of alcohol consumption for the management of hypertension.
Results Overall, 81.9% of physicians reported to generally quantify alcohol consumption in patients with hypertension. However, only 28.6% and 14.5% of participants reported screening alcohol consumption in their patients with newly detected or treatment-resistant hypertension. Physicians recommended a maximum alcohol intake of 13.1±11.7 g/day for women (95% CI 12.3 to 13.8) and 19.9±15.6 g/day for men (95% CI 18.8 to 20.9). In case of moderate to high alcohol consumption, 10.3% would manage only hypertension without addressing alcohol consumption, while 3.7% of the physicians would do so in case of alcohol dependence (p<0.001).
Conclusions The average amount of alcohol intake per day recommended by European physicians in this survey was in agreement with the guidelines. The low number of physicians that screen for alcohol consumption in patients with newly detected and with treatment-resistant hypertension indicates an important deficit in the management of hypertension.
- alcohol management
- survey
- alcohol screening
- guidelines implementation
- lifestyle changes
- hypertension
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Identifying deficits in the management of alcohol consumption among European physicians attending annual scientific meetings in the field of cardiovascular or internal medicine indicates a need to develop better future alcohol interventions.
The majority of physicians participating in this survey were hospital based (78.5%), although outpatient care in the ambulatory setting plays a predominate role in the long-term management of hypertension.
Answers were self-reported in a face-to-face interview, which might have shifted some results upwards and led to an overestimation in our analysis.
Introduction
High blood pressure (BP) or hypertension represents a main non-communicable risk factor for global burden of disease.1 In 2015, the global age-standardised prevalence of raised BP was 24.1% in men and 20.1% in women,2 affecting more than one billion subjects worldwide3 and thus constituting a primary health concern.3 The harmful use of alcohol accounts for 5.1% of the global burden of disease and injury, measured in disability-adjusted life years,4 5 and for 3.3 million deaths every year, representing 5.9% of all deaths worldwide.5 Among the more than 200 diseases and injuries for which alcohol causality is well established,6 we also find a linear relationship between elevated BP and alcohol consumption.7 8 The exact mechanism of alcohol-induced hypertension is complex9 and on a molecular level still largely unknown.9 On one hand, alcohol seems to increases the tendency to vasoconstriction due to an impairment of the baroreceptors10 11 and imbalance of the central nervous system regulation, resulting in enhanced sympathetic activity.12 In addition, alcohol consumption increases also cortisol levels and stimulates the renin–angiotensin–aldosterone system.13 The chronic alcohol-induced elevation of angiotensin II has been shown in rodents to directly cause inflammation and endothelial injury through increase of oxidative stress.14 15 This, on the other hand, leads to inhibition of endothelium-dependent nitric oxide production and thus to endothelial dysfunction with impaired vasodilation.16 17
Accordingly, moderation of alcohol consumption to no more than 20–30 g of alcohol per day in men and 10–20 g of alcohol per day in women was one of the six recommended lifestyle changes in the current European Society of Hypertension (ESH) and European Society of Cardiology (ESC) guidelines for the management of arterial hypertension18 (online supplementary table 1). While not done in the previous edition in 2007 and its reappraisal in 2009, the last available guidelines (2013) graded the strength of this six recommended lifestyle changes for the first time with a class I evidence level A.
Supplementary file 1
Currently, BP control rates in patients treated with hypertension across Europe are insufficient, with less than 50% of the patients achieving BP goals,19–21 and alcohol seems to be the least intervened factor in the management of hypertension.22–24 According to the latest WHO status report on alcohol and health,6 the amount of alcohol consumed in the European Region is almost twice the worlds average.6 Thus, efforts aiming to improve BP control, specifically through interventions in the management of alcohol consumption, are justified. Furthermore, the impact of screening and brief interventions for alcohol use in primary care have been proven positive in many European projects,25 26 such as the Primary Health care European Project on Alcohol27 and the Optimizing Delivery of Health care Interventions.28 29
Against this background, we conducted a survey to investigate, by European physicians across different specialties and workplaces, screening of alcohol consumption, awareness and self-implementation of the recommendation to moderate alcohol consumption in their patients with hypertension.
Methods
The survey collected data during four annual congresses between April and October 2015. Two of the meetings were German (meeting of the German Society of Cardiology (DGK)30 and the German Society of Internal Medicine (DGIM)31), and two were European (ESH32 and ESC).33 Attending physicians willing to participate were interviewed in German in the two German meetings and in English at the two European meetings. The complete questionnaire consisted of two parts: the first containing 10 (online supplementary table 2) and the second 6 questions (table 1), respectively. Basic demographic data of the participants as well as awareness and implementation of the six recommended life style changes in the 2013 ESH/ESC guidelines18 into clinical practice were assessed through part 1 (online supplementary table 2); the results are reported elsewhere.34 Part 2 of the survey included six questions (table 1), which focused exclusively on the awareness and implementation of the European physicians regarding the role of moderation of alcohol intake in the management of their patients with hypertension.
Questionnaire items included in this study (corresponding to part 2 of the original survey)
Throughout the manuscript, we expressed all measures using consistently grams of alcohol to report amounts of ethyl alcohol (ethanol). According to the UK Chief Medical Officers,35 a unit of alcohol contains 8 g of pure alcohol.35
Patient and public involvement
No patients were involved in this study.
Statistical analysis
Data were analysed with SPSS software (IBM SPSS Statistics V.24). The number of responses available for each questionnaire item is reported, and relative frequencies are given as adjusted percentages excluding missing values. For each variable of interest comparisons within the following subgroup categories were performed: meeting (European: ESH/ESC vs German: DGK/DGIM), place of work (hospital vs practice), medical specialisation (general practitioner (GP) vs cardiologists vs internists vs other specialisations). For comparison between categorical variables, χ2 test analyses were performed. For continuous variables, t-tests or one-way analyses of variance (with Bonferroni post hoc correction for multiple comparisons) were applied. A two-sided p<0.05 was considered statistically significant.
Results
The characteristics of the participating physicians are given in table 2. Overall, 1064 physicians (37.4% female) took part in the survey (806 at the European and 258 at the German meetings, respectively). About 20% of the asked physicians were not willing to participate in the survey. The participants were predominantly cardiologists (52.1%) and internists (29.2%), while 8.8% were GPs and 78.5% of all physicians were hospital-based.
Characteristics of participating physicians
Estimating proportion of patients with hypertension with additional alcohol problems
Participating physicians (n=946) estimated that 18.0%±15.9% (range: 0%–95%) of their patients with hypertension have additional alcohol problems. Higher percentages were estimated by physicians attending the German meetings compared with their colleagues attending the European meetings (22.3% vs 16.8%; p<0.001). By their own estimates, physicians working in a practice reported that significantly higher rates of patients with hypertension have additional alcohol problems compared with their hospital-based colleagues (estimated 21.4% patients visiting a practice have additional alcohol problems vs estimated 17.2% in hospital; p<0.05). Concerning different medical specialisations, GPs estimated that a significantly higher percentage of their patients with hypertension (27%, p<0.001) are affected by additional alcohol problems compared with cardiologists (16.7%), internists (18.4%) or physicians from other specialisations (16.9%).
Quantification of alcohol consumption
Overall, 81.9% of participating physicians (n=1028) responded ‘yes’ to the question ‘Do you quantify alcohol consumption in your patients with hypertension?’ (Q11, table 1). Physicians attending the German meetings quantified the alcohol consumption of their patients with hypertension significantly less often than the attendees of the European meetings (74.5% vs 84.3%; p<0.001). The frequencies for quantification of alcohol consumption did not show any statistically significant association according to place of work or specialisation of physicians (data not shown).
Screening of alcohol consumption in different clinical settings
In the survey, 986 physicians responded to the question ‘When do you ask for alcohol consumption in patients with hypertension?’ (figure 1A). Screening of alcohol consumption took place primarily in the context of newly detected hypertension (28.6%) rather than in patients with hypertension and very high BP (17.5%) or in patients with treatment-resistant hypertension (14.5%). Free-text answers were additionally sorted and classified into ‘Rarely-never’ and ‘Always-regularly’. Overall, 55.2% of the respondent physicians reported regularly quantifying alcohol consumption in their patients with hypertension. When responses of the attendees at the European and German meetings were compared, significantly more physicians attending the European meetings reported asking about alcohol consumption in their patients with hypertension regularly (68.8% vs 10.8%; p<0.001; figure 1A).
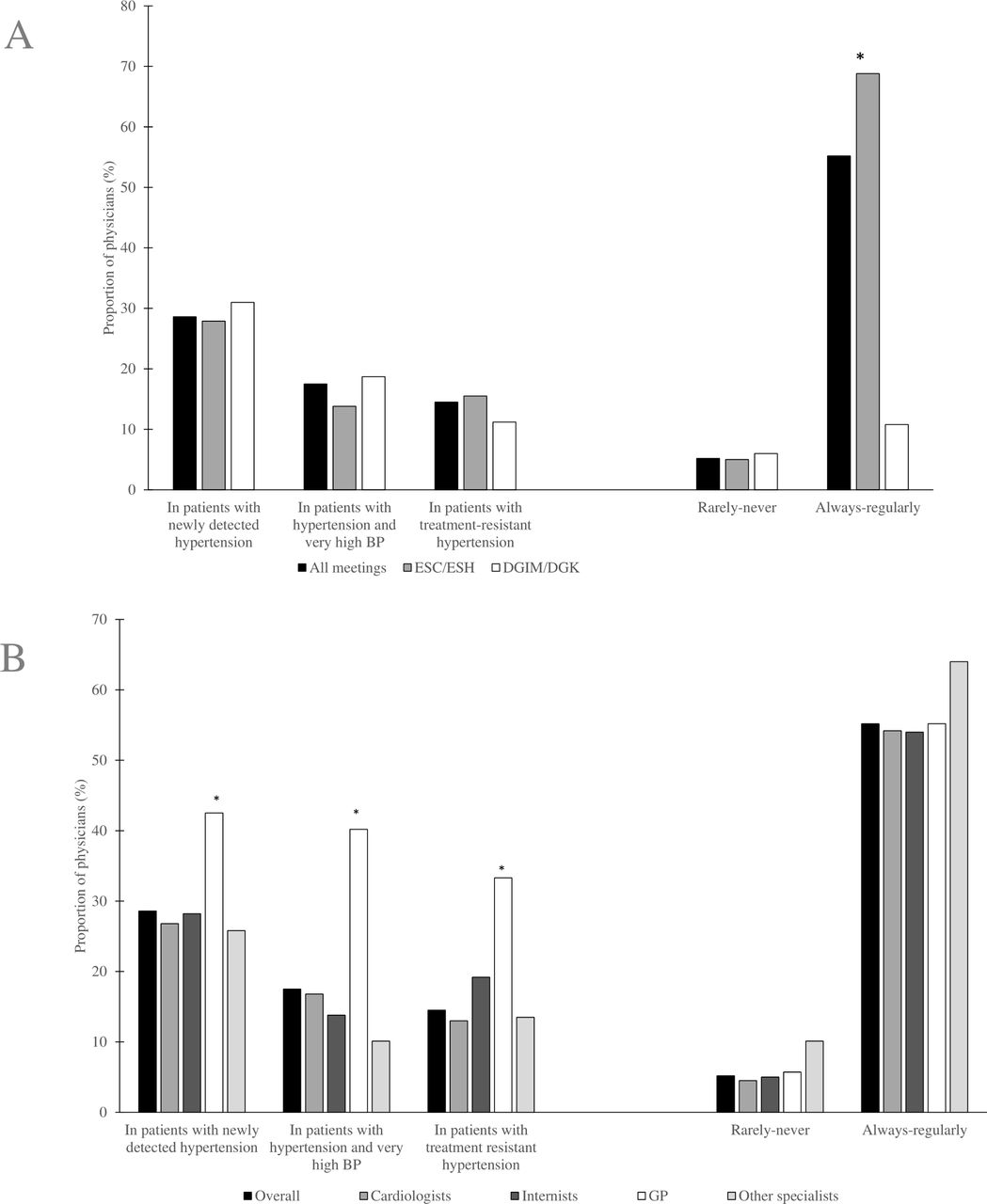
Proportion of physicians (%) answering the multiple choice question: ‘When do you ask for alcohol consumption in patients with hypertension?’ (A) Proportion of physicians (all meetings n=986) attending the European meetings compared with the physicians attending the German meetings. Differences are significant *p<0.05. (B) Proportion of physicians from different medical specialties (overall n=981); *Difference is significant p<0.05 for GP compared with each one of the other specialisations. BP, blood pressure; DGIM, German Society of Internal Medicine; DGK, German Society of Cardiology; ESC, European Society of Cardiology; ESH, European Society of Hypertension; GP, general practitioner.
GPs asked significantly more often (42.5%) than internists (28.2%), cardiologists (26.8%) or physicians from other medical specialisations (25.8%; all p<0.05) about alcohol consumption in patients with newly detected hypertension. Similar differences between GPs and physicians from other specialties were observed regarding screening of alcohol consumption in patients with very high BP as well as in patients with treatment-resistant hypertension (figure 1B).
Self-reported management or referral of patients with hypertension for the treatment of hypertension and/or alcohol problems
In patients with both hypertension and moderate to high alcohol consumption, 52% of the responding physicians (n=1021) would treat and manage both conditions by themselves and 10.3% would manage only hypertension without taking further action. In case of alcohol dependence, 13.8% would treat both hypertension and alcohol dependence, while 3.7% would treat only hypertension without taking further action, and 64.1% would only treat hypertension and refer the patient to a specialist for the management of alcohol dependence (p<0.001). These differences are shown in figure 2.

{kind=link}
{kind=link}
Proportion of physicians (%) answering the multiple choice question: ‘What actions will you take when you diagnose someone with hypertension and alcohol consumption?’ Differences are significant *p≤0.001 in case of moderate and high alcohol consumption (n=1021, physicians) versus alcohol dependence (n=1025, physicians). GP, general practitioner.
In patients with moderate or high alcohol consumption but without alcohol dependence, 58.9% of the internists reported managing both hypertension and alcohol problems significantly more as compared with cardiologists (49.2%) and other specialists (44%; p<0.001). Differences between internists and GPs were not statistically significant (58.9% vs 52.8%; p>0.05). In addition, physicians working in a practice were significantly more likely to manage both hypertension and the alcohol problems themselves, than their colleagues working in a hospital (59.1% vs 50.3%; p<0.05). Physicians attending the German meetings reported managing both alcohol dependence and hypertension significantly more than their colleagues attending the European meetings (14.7% vs 10.9%; p<0.001).
Maximum amount of alcohol per day recommended
Physicians reported to recommend a maximum alcohol intake of 13.1±11.7 g/day for women (n=901 reporting physicians; 95% CI 12.3 to 13.8; range: 0–150) and 19.9±15.6 g/day for men (n=884 reporting physicians; 95% CI 18.8 to 20.9; range: 0–150).
For men, 43% of physicians recommended less than 20 g alcohol intake/day, 44% recommended between 20 and 30 g/day and 13% recommended more than 30 g/day. In their recommendations for women, 21% recommended less than 10 g/day, 71% recommended 10–20 g/day women and 8% recommended more than 20 g/day women.
Physicians attending the German meetings were significantly more tolerant with their recommendations of the maximum amount of alcohol per day for women and men than their colleagues attending the European meetings (15.8±9.4 g/day vs 12.1±12.2 g/day for women and 28.3±17.5 g/day vs 16.9±13.7 g/day for men; p<0.001). Physicians working in a practice were consistently more tolerant than hospital-based physicians in their recommended maximum alcohol intake for men (23.5±20.8 g/day vs 18.8±13.6 g/day; p<0.05), but not for women (14.7±15.0 g/day vs 12.6±10.5 g/day; p>0.05). Significant differences were not observed for the alcohol intake of men or women between physicians belonging to different medical specialisations (table 3).
Recommendation for alcohol intake of participating physicians
Discussion
The relationship between elevated BP and alcohol consumption is well established,7 8 and the importance of their burden of diseases,1–6 36 prove them as global public health priorities. Consequently, alcohol consumption and raised BP are key parts of WHO goals to reduce non-communicable diseases (NCD) global NCD mortality by 25% by 2025.6
According to a review and meta-analysis by Roerecke et al,8 moderation of alcohol consumption can reduce BP in a dose-dependent manner in people drinking more than 24 g of pure alcohol per day.8 Furthermore, this reduction was shown to be similar to that of other lifestyle changes,8 such as regular exercise37 or reduction of weight.38 Lifestyle changes can reduce or eliminate the need for antihypertensive medication in patients with hypertension,39–41 and their BP-lowering effects can be comparable to those effects achieved by drug monotherapy.39 40 Nevertheless, even if elevated BP and harmful alcohol consumption are preventable public health priorities, until the last 15 years, alcohol policies were largely not supported by sufficient research findings.42 43 Recently, globally important public health organisations such as Global Alcohol Policy Alliance44 supported the generation of evidence-based recommendations on alcohol policies.44 In Europe, Alcohol Measures for Public Health Research Alliance (AMPHORA)45 was the first research project on alcohol from a public health perspective that had been cofinanced by the European Commission through the Seventh Framework Programme of Research.46 AMPHORA’s affiliated organisations from all 27 member states aimed to generate scientific evidence about alcohol consumption and alcohol-related harm to help cover the European policy gap.45 In its final report updated in August 2013, AMPHORA reported that there is still a lot to be done and emphasised the need to identify more clearly which factors on a European level are limiting the effectiveness and implementation of alcohol policies.47 Therefore, our efforts assessing the awareness, screening and current interventions in alcohol consumption in patients with hypertension among European physicians are very well justified.
Our analysis showed that European physicians also recognised a high prevalence of high BP and comorbid alcoholism. About 27% of the patients with hypertension have additional alcohol problems, as estimated by their treating physicians. Similarly, in the general population aged 15–64 years, 300 of 1000 men consume 40 g of alcohol or more per day in Europe.48 Some aspects and practices on the management of alcohol in patients with hypertension observed in the current survey appear acceptable or positive. These include the amount of alcohol recommended by the participating physicians for both genders, which was below the thresholds recommended in the European guidelines.18 In addition, more than 80% of the physicians reported to generally quantify the alcohol consumption of their patients with hypertension. The screening of alcohol consumption was, however, very poor in some important clinical settings. Less than one-third of the European physicians asked about alcohol consumption in cases of newly detected hypertension and less than one-fifth asked in patients with very high BP. Moreover, even fewer (14.5% of the participating physicians) asked patients with treatment-resistant hypertension about alcohol consumption. This result is of major clinical interest, because 10%–30% of patients with hypertension are considered to be resistant to treatment,49 50 and patients with treatment-resistant hypertension have a considerably higher risk for stroke, cardiovascular and kidney disease than patients with controlled hypertension, as shown in multiple studies.51–54 Furthermore, there is good evidence that treatment-resistant hypertension can also be linked to non-adherence to moderation of alcohol consumption.55–57 Regarding the low number of physicians asking about alcohol consumption in newly detected hypertension, in patients with very high BP and in patients with treatment resistance observed in our current study, we cannot exclude the possibility that some physicians assumed that answering ‘regularly’ in our survey did include all of the situations mentioned above, although this question was read in the interview as a multiple choice question with the possibility of more than one answer (Q12 in figure 1). Moreover, even considering this possibility, only half of the interviewed physicians, and also half of the GPs answered ‘regularly’ to the question: ‘When do you ask about alcohol consumption in patients with hypertension?’ These percentages of alcohol screening are still unsatisfactory.
In comparison to a similar study conducted exclusively in GPs in Europe, Rehm et al 22 noted that 34% of interviewed GPs reported sufficient screening of alcohol in patients with hypertension. However, the study design and questions are not fully comparable with the present report: The study by Rehm et al,22 was based on online questionnaires, and the interviewers did not ask if GPs quantified alcohol consumption in their hypertensive patients (yes/no). Instead, sufficient screening was assumed if GPs screened at least 7 out of 10 hypertensive patients for alcohol consumption.22 In another part of the same study, published separately by Kraus et al,58 less than half of the German and European patients with hypertension in primary care were screened for alcohol use.58 Collectively, the findings by Rehm et al 22 and Kraus et al 58 are in agreement with our analysis concluding that screening for alcohol consumption in hypertensive patients is poor among German and European GPs and should be improved.
In the current survey, a significantly greater fraction of physicians participating in the German meetings estimated that their patients exhibit both hypertension and alcohol problems compared with the participants at the European meetings. Nevertheless, a significantly greater fraction of physicians attending the German meetings (25.5%) did not quantify alcohol consumption in their patients with hypertension as compared with their colleagues attending the European meetings (15.7%). Accordingly, physicians attending the German meetings had lower awareness of the class I level of evidence A recommendation on the moderation of alcohol consumption contained in the ESH/ESC guidelines18 than their peers attending the European meetings.34 Similarly, Kraus et al 58 reported in their survey analysis, that German GPs do not consider alcohol intake as a major risk for hypertension58 and their screening rates were slightly lower than the European average.58 It is arguable that these differences between German and European physicians are due to a stronger cultural bond with alcohol than other European countries,59 60 which might obscure the perception of alcohol-related harm among German physicians.
The deficits identified in this study are worth overcoming, as alcohol screening and brief intervention have showed positive results in many European projects.25 27 28 Lack of resources, training and support from management, as well as workload26 have been described as barriers to the adoption of screening and brief intervention.26 We believe in the importance of finding economically sustainable ways of working against these barriers with the objective of systematising alcohol interventions. Future research should serve as a valuable feedback measuring the effects and extend of such implementation.
Among the limitations of this study, there might have been a bias towards inclusion of physicians who have a particular interest in the management of hypertension. In addition, reasons for non-participation were not recorded in our study. Also, while we recorded the nationality of the participating physicians, country of practice was not assessed in our survey. During the conduction of the survey, participants who volunteered to participate in the survey were informed by the interviewers before the start of the interview that only one participation was allowed. As participation in the survey was voluntary with anonymised data collection, we cannot exclude the possibility, although deemed very unlikely, of intentional or unintentional multiple participations. The implementation of standardised assessment of alcohol intake, like Alcohol Use Disorders Identification Test for Consumption,61 or Severity of Alcohol Dependence Questionnaire62 or other available screening instruments, as well as how physicians assess and diagnose alcohol dependence, were not recorded in our study. Furthermore, the majority of physicians participating in the survey were hospital based (78.5%), although long-term management of hypertension is predominantly carried out in an ambulatory setting. Moreover, because some questions were formulated as closed questions (ie, questions that can be answered with yes/no) and answers were self-reported, social pressure might have shifted some results upwards and led to an overestimation in our analysis.
In summary, European physicians recognise the high prevalence of comorbid hypertension and harmful alcohol consumption. In addition, some aspects of their management strategies in patients with hypertension regarding alcohol consumption appear adequate. In contrast, alcohol consumption screening in cases of newly detected hypertension, in patients with very high BP, and in treatment-resistant hypertension is very poor. Given the clinical importance of the latter conditions, the current report further supports the notion that improvements of awareness among European physicians on moderation of alcohol intake as an important modifiable lifestyle factor in hypertension management are necessary.
Acknowledgments
We are thankful to Angelika Thomas and Rhoda Wismer (signum [ pr GmbH, Cologne) for their excellent support. The survey results were presented at the 27th European Meeting on Hypertension and Cardiovascular Protection 2017 in Milan.
References
Footnotes
Contributors LZT performed the statistical analyses, interpreted the data and wrote the manuscript. JB supervised the statistical analyses and revised the manuscript. TGR helped perform the statistical analyses with constructive discussion and revised the manuscript. RK conceived and designed the study, revised the manuscript for important intellectual content and provided supervision.
Funding This survey was funded by Lundbeck AS (Valby, Denmark). We acknowledge support from the German Research Foundation (DFG) and the Open Access Publication Fund of Charité–Universitätsmedizin Berlin.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.