Article Text

Abstract
Objective Hepatocellular carcinoma (HCC) is the third leading cause of cancer death worldwide. We conducted network meta-regression within a Bayesian framework to compare and rank different treatment strategies for HCC through direct and indirect evidence from international studies.
Methods and analyses We pooled the OR for 1-year, 3-year and 5-year overall survival, based on lesions of size ˂ 3 cm, 3–5 cm and ≤5 cm, using five therapeutic options including resection (RES), radiofrequency ablation (RFA), microwave ablation (MWA), transcatheter arterial chemoembolisation (TACE) plus RFA (TR) and percutaneous ethanol injection (PEI).
Results We identified 74 studies, including 26 944 patients. After adjustment for study design, and in the full sample of studies, the treatments were ranked in order of greatest to least benefit as follows for 5 year survival: (1) RES, (2) TR, (3) RFA, (4) MWA and (5) PEI. The ranks were similar for 1- and 3-year survival, with RES and TR being the highest ranking treatments. In both smaller (<3 cm) and larger tumours (3–5 cm), RES and TR were also the two highest ranking treatments. There was little evidence of inconsistency between direct and indirect evidence.
Conclusion The comparison of different treatment strategies for HCC indicated that RES is associated with longer survival. However, many of the between-treatment comparisons were not statistically significant and, for now, selection of strategies for treatment will depend on patient and disease characteristics. Additionally, much of the evidence was provided by non-randomised studies and knowledge gaps still exist. More head-to-head comparisons between both RES and TR, or other approaches, will be necessary to confirm these findings.
- resection
- radiofrequency ablation
- microwave ablation
- transcatheter arterial chemoembolization
- percutaneous ethanol injection
- hepatocellular carcinoma
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- resection
- radiofrequency ablation
- microwave ablation
- transcatheter arterial chemoembolization
- percutaneous ethanol injection
- hepatocellular carcinoma
Strengths and limitations of this study
This is a network meta-regression within a Bayesian framework to compare and rank different treatment strategies for HCC through direct and indirect evidence from international studies.
Strong and reliable methodological and statistical procedures were applied.
The individual or tumour characteristics within HCC articles would be a source of heterogeneity.
A major limitation is in the inclusion of non-randomised studies, in which selection bias is likely to confound observations. Selection of treatment is likely to be based on individual or tumour characteristics, and thus these factors will bias and confound observations of survival.
Other studies did not report the primary outcome of interest (5-year survival) and this was a particular limitation among randomised studies.
Introduction
Cancer was the second leading cause of death in 2013, behind cardiovascular disease, and in 2013 more than 8 million people died from cancer globally.1–3 Hepatocellular carcinoma (HCC) was the sixth most common cancer worldwide and the third leading cause of cancer death, with 5-year overall survival rates under 12%.4 5
Hepatic resection (RES) was the traditional choice for patients with HCC, without cirrhosis and with good remaining liver function.6 Despite nearly 70% 5-year survival, recurrence rates after surgery were high.7 Repeated hepatectomies to lengthen survival were not often appropriate owing to multiple-site tumour recurrence or patient background of liver cirrhosis.8 9 Many locoregional therapies have been developed including ablative treatments such as percutaneous ethanol injection (PEI), radiofrequency ablation (RFA) or microwave ablation (MWA) and transarterial therapies such as transcatheter arterial chemoembolisation (TACE) or transarterial chemotherapy infusion (TACI). Locoregional therapies were minimally invasive and therefore are cheaper and faster to recover, as compared to resection. Such approaches may be appropriate for patients with unresectable, small or multiple carcinomas or those with severe cirrhosis. However, there may be a greater risk of recurrence because of incomplete destruction of cancer cells at the treatment margin, as seen with RFA.10
The selection of treatment strategy was determined by liver function, tumour stage and patient performance status,7 but much uncertainty still remains surrounding the comparative efficacy of different treatment approaches. A recent review of international guidelines for HCC found similarities but also some discrepancy in treatment allocation recommendations because of regional classification differences, secondary to a lack of solid or high-level evidence.11 A recent review of therapies also revealed that there was no consensus on whether surgery or ablation was better for small tumours.7 Some discrepancy in prevalence and treatment outcomes may be still in different regions because of local biology, available resources or expertise and access to care.11 However, if we ever hope to achieve standardised and evidence-based therapy for HCC, the unanswered question surrounding relative treatment efficacy of RES compared with ablative locoregional therapies should be resolved.
Traditional meta-analysis is limited by existing head-to-head treatment comparisons within included studies. It is therefore not possible to gauge the relative benefit of the two treatments that have never been directly compared in studies. Real-life treatment decisions are hindered by gaps in existing evidence, but network meta-analysis enables integration of direct and indirect comparisons to provide estimates for relative comparisons across many treatments.12 Recent published network meta-analysis focused on advanced HCC by TACE alone or combined treatments,13 14 as well as antineoplastic drugs (sorafenib, erlotinib, linifanib, sunitinib and brivanib),15 and early- or very early-stage HCC via surgery or thermal ablation.16 However, in this study, we included the latest literature, and focused on the comparison of interventional and surgical treatments, including RES, RFA, MWA and TACE plus RFA (TR), PEI using subgroup analysis of tumour size (smaller: <3 cm; larger: 3–5 cm) and study design (cohort or randomised clinical trial (RCT)). In order to investigate comparative effectiveness among RES and common locoregional ablative therapies, we performed a strong and reliable Bayesian network meta-analysis.
Search strategy
We conducted a systematic review and report findings in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Network Meta-Analyses (PRISMA-NMA)17 (online supplementary text S1). The following databases were searched: PubMed, Embase, Web of Science and Scopus, up to May 2018, using these keywords: resection, surgery, hepatectomy, radiofrequency ablation, transarterial chemoembolisation, microwave thermal ablation, ethanol injection, liver, cancer and tumour (online supplementary text S2). No language restrictions were used. Bibliographies from other relevant review articles were cross-examined for potential missed studies. Disagreement was resolved by a third reviewer. Citations were downloaded into reference management software and duplicate citations were electronically or manually removed.
Supplemental material
We systematically included the studies using the following criteria: (1) original data from prospective or retrospective cohort studies and RCTs in humans; (2) reporting at least two treatments, including resection or any local ablative therapy (RES, RFA, MWA, PEI or TACE+RFA (TR)); (3) mean lesion size ≤5 cm and (4) evaluating overall survival rate not less than 1 year after first or recurrent treatments. Conference abstracts and case reports were excluded, as were older publications from studies with multiple publications.
Patients and public involvement
The patients or public were not involved in the study.
Data extraction and study quality
Two investigators independently extracted and cross-checked the data from the eligible studies: author, year, study design, country, disease type, inclusion criteria, treatment style, study size, gender, age, tumour size, follow-up duration, treatment complications and survival outcomes. If in disagreement, a third reviewer was asked to adjudicate. The level of evidence was appraised using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) guidance,18 which was classified into four levels: high, moderate, low and very low. The quality score was downgraded according to five domains, including the risk of bias, inconsistency, indirectness, imprecision and publication bias while scores were upgraded according to large effect, appropriate control for plausible confounding and dose–response gradient.
Data analysis
Network meta-analysis was used if a ring or open evidence loop was available to know the number of arms and the sample size of each intervention. When possible, pair-wise direct head-to-head comparisons were conducted to calculate the OR of 1-, 3- and 5-year survival and their 95% CI. Between-study heterogeneity was evaluated using the tau-squared statistic (τ).2 19 A node-splitting analysis was applied to check the consistency between direct evidence (existing real reported comparisons) and indirect evidence (estimated treatment comparisons) for their agreement on a specific node.20 Bayesian network meta-analysis with Markov chain Monte Carlo (MCMC), through a consistency model, was utilised to estimate the pooled ORs and its 95% credible interval (CrI) for direct and indirect comparisons.16 The inconsistency model was used to check for heterogeneity due to chance imbalance in the distribution of effect modifiers. Consistency in every closed loop was checked by the loop-specific approach in order to estimate whether treatment survival effects were disturbed by variance in the distribution of potential confounding factors among the studies. In order to compare and rank survival rates of different treatments, we examined all studies first and then separately assessed smaller (<3 cm) and larger (3–5 cm) tumours. Random-effect meta-regression models were used, with and without adjustment for study design (cohort or RCT) and subgroup analyses were also conducted for RCTs in order to examine treatment effectiveness. We appraised the ranking probabilities for all therapies for each intervention and the treatment hierarchy was ordered by the surface under the cumulative ranking curve (SUCRA).21 Sensitivity analysis was conducted to remove each study, in turn, and estimate the treatment effect in the remaining studies. Funnel plots were utilised to check the possible presence of publication bias or small-study bias.22 In this study, we used Bayesian MCMC simulations by WinBUGS 1.4 and graphically presented the results using Stata V.13.
Results
Study characteristics
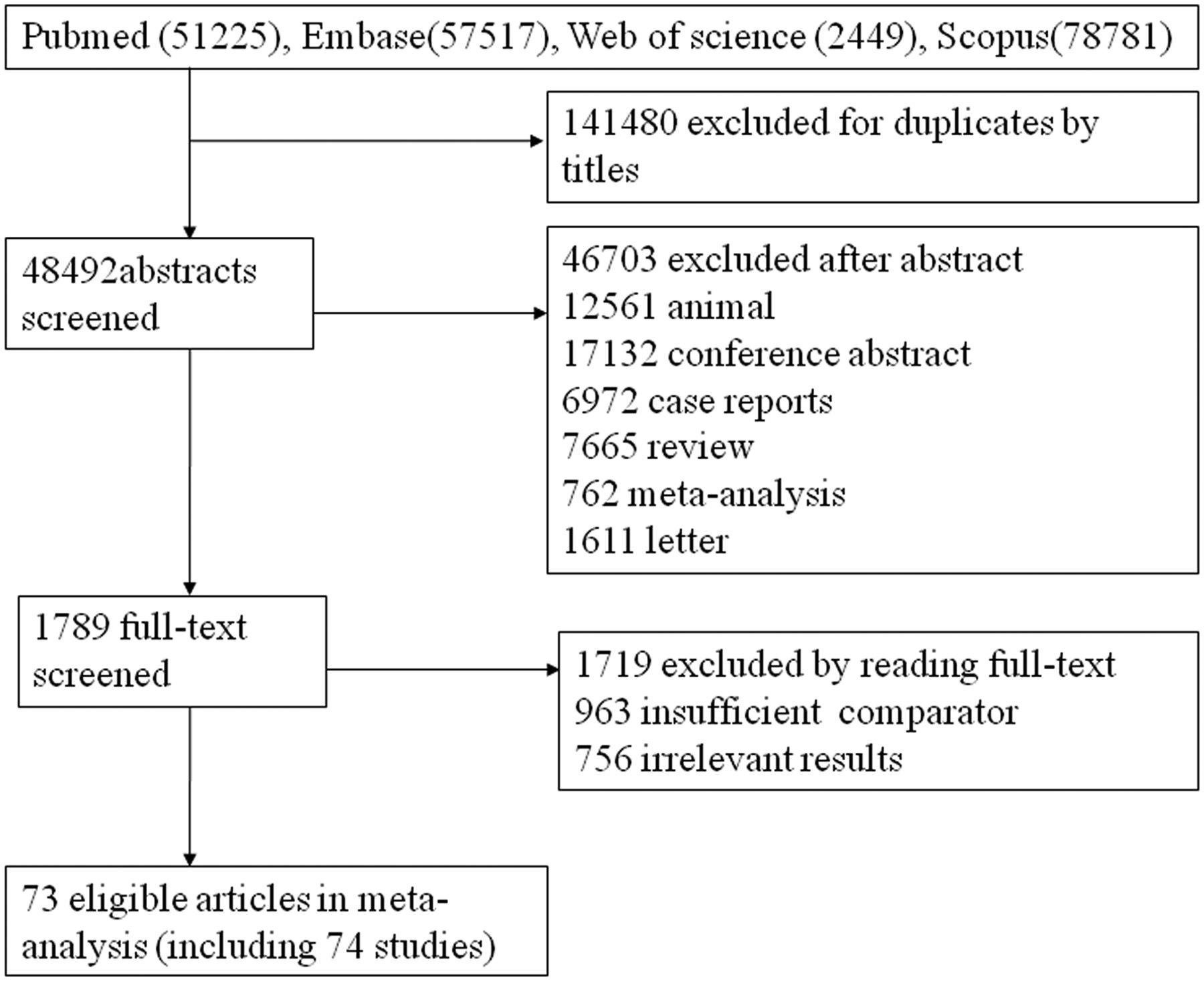
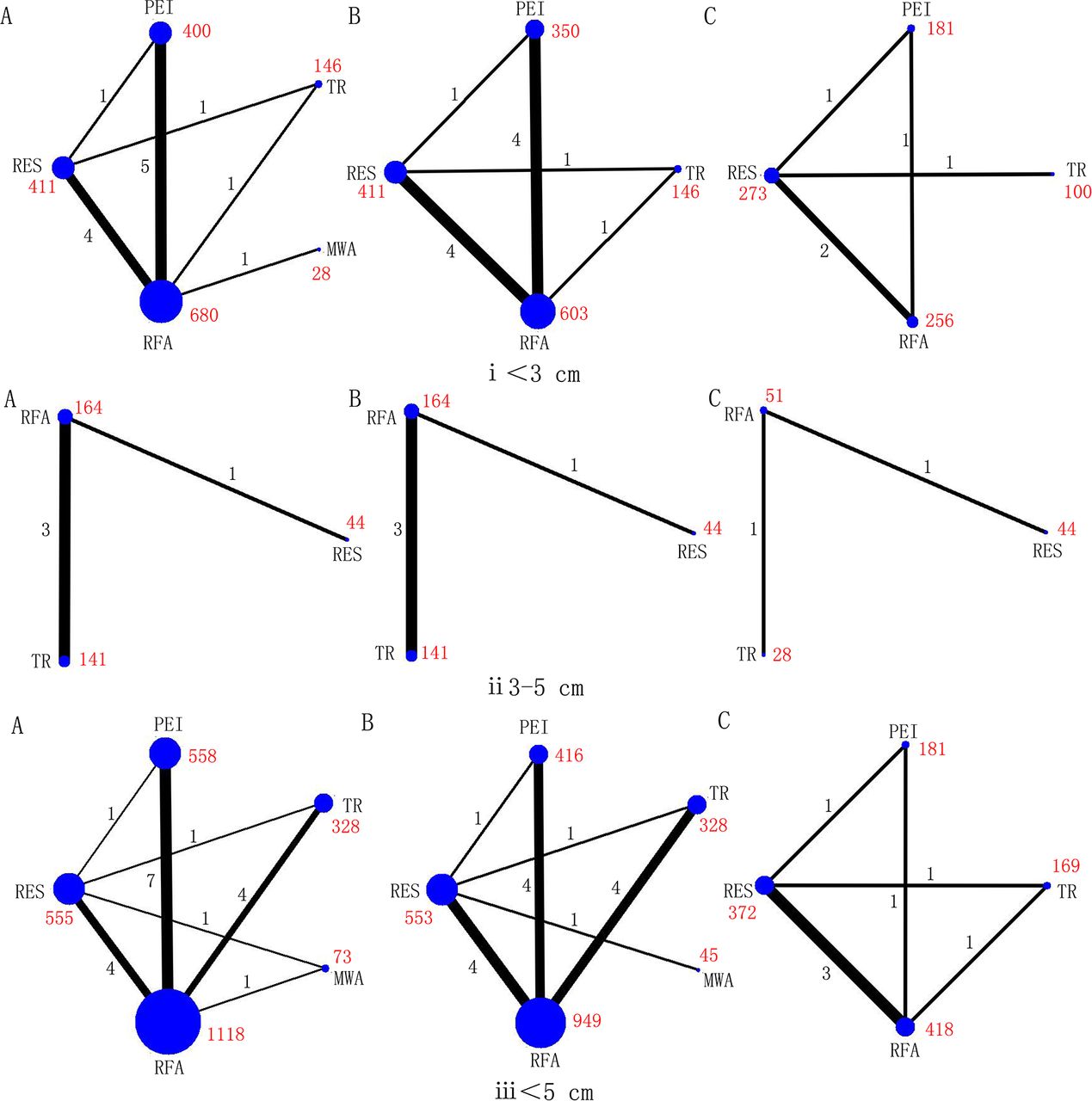
After screening, 74 relevant studies in 73 articles were identified, of which 20 were RCTs and 54 were cohort studies.23–96 We excluded 136 504 duplicate or non-relevant citations (figure 1). The summary characteristics of these studies are shown in online supplementary table S1. Overall, 32 345 patients of mean age from 46 to 73.5 years, with approximately 29 236 tumours, were assigned to receive RES, RFA, MWA, TR and PEI, and the mean follow-up ranged from 1.5 to 5.7 years. In addition, the number of connected studies to the lines (black) and sample size of each treatment (red) were shown in figures 2 and 3, respectively.

Flow chart of search.

Networks of treatment comparisons for 1 year (A), 3 year (B), and 5 year (C) survival rates in RCTs. Circle size is proportional to the number of included patients and line width indicates the number of studies comparing the connected treatments. The number in red indicates the sample size and the number in black indicates the number of studies. (i) Lesions <3 cm. (ii) Lesions 3–5 cm. (iii) Lesions≤5 cm.
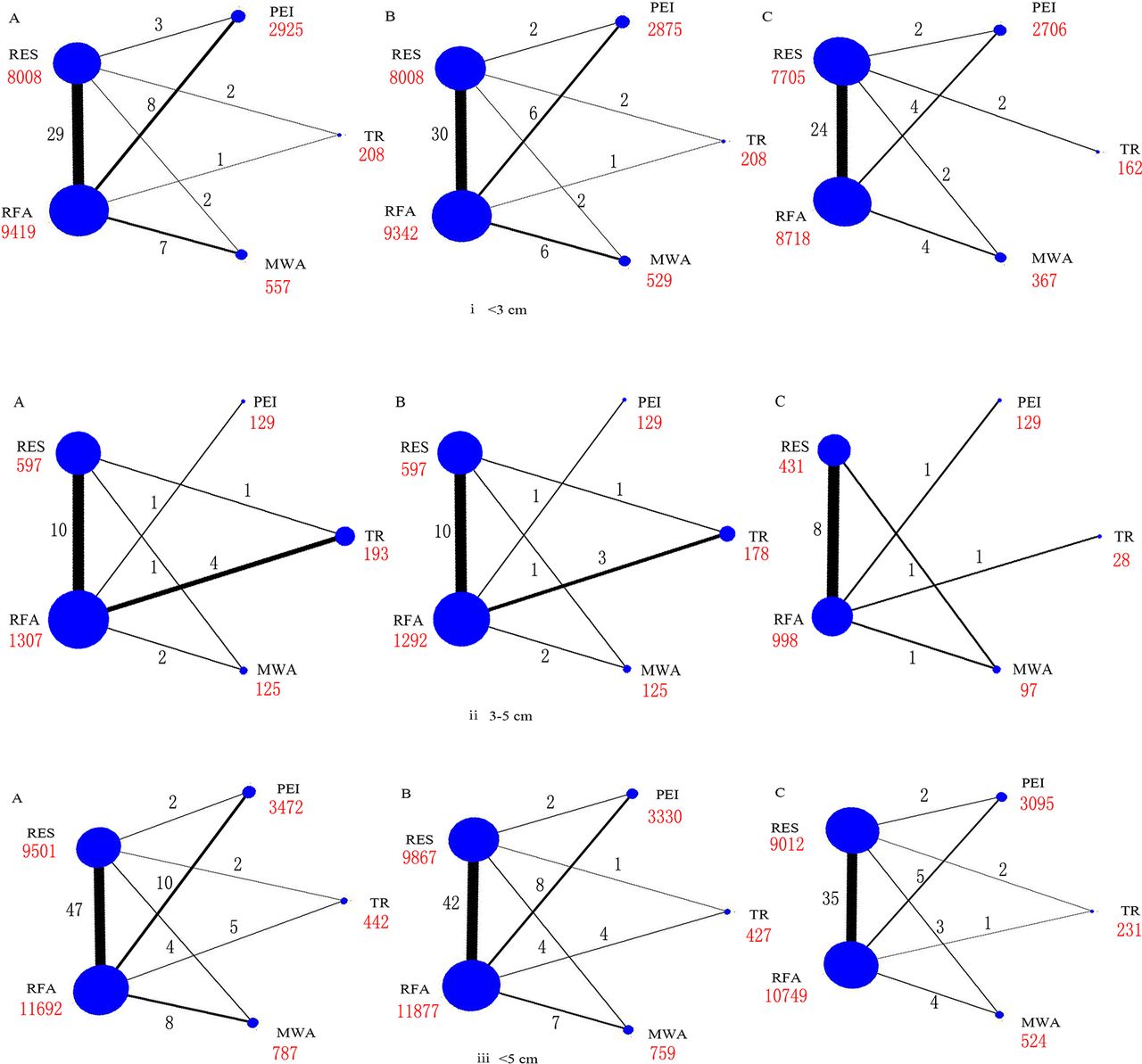
Networks of treatment comparisons for 1 year (A), 3-year (B), and 5-year (C) survival rates in all the studies. Circle size is proportional to the number of included patients and line width indicates the number of studies comparing the connected treatments. The number in red indicates the sample size and the number in black indicates the number of studies. (i) Lesions <3 cm. (ii) Lesions 3–5 cm. (iii) Lesions≤5 cm.
Network meta-analysis results
Ten possible treatment comparisons among the five interventions were examined in the included studies. Comparable survival estimates were made for each treatment (per 1000 patients) and the survival OR among each of the treatment comparisons, according to follow-up duration, are presented in online supplementary table S2, along with estimation of the quality of evidence using GRADE criteria.
Across the range of treatment comparisons and follow-up durations, evidence was graded between low and high quality. Evidence was often graded as low quality owing to publication bias and graded as high quality owing to a larger number of participants in direct comparisons.
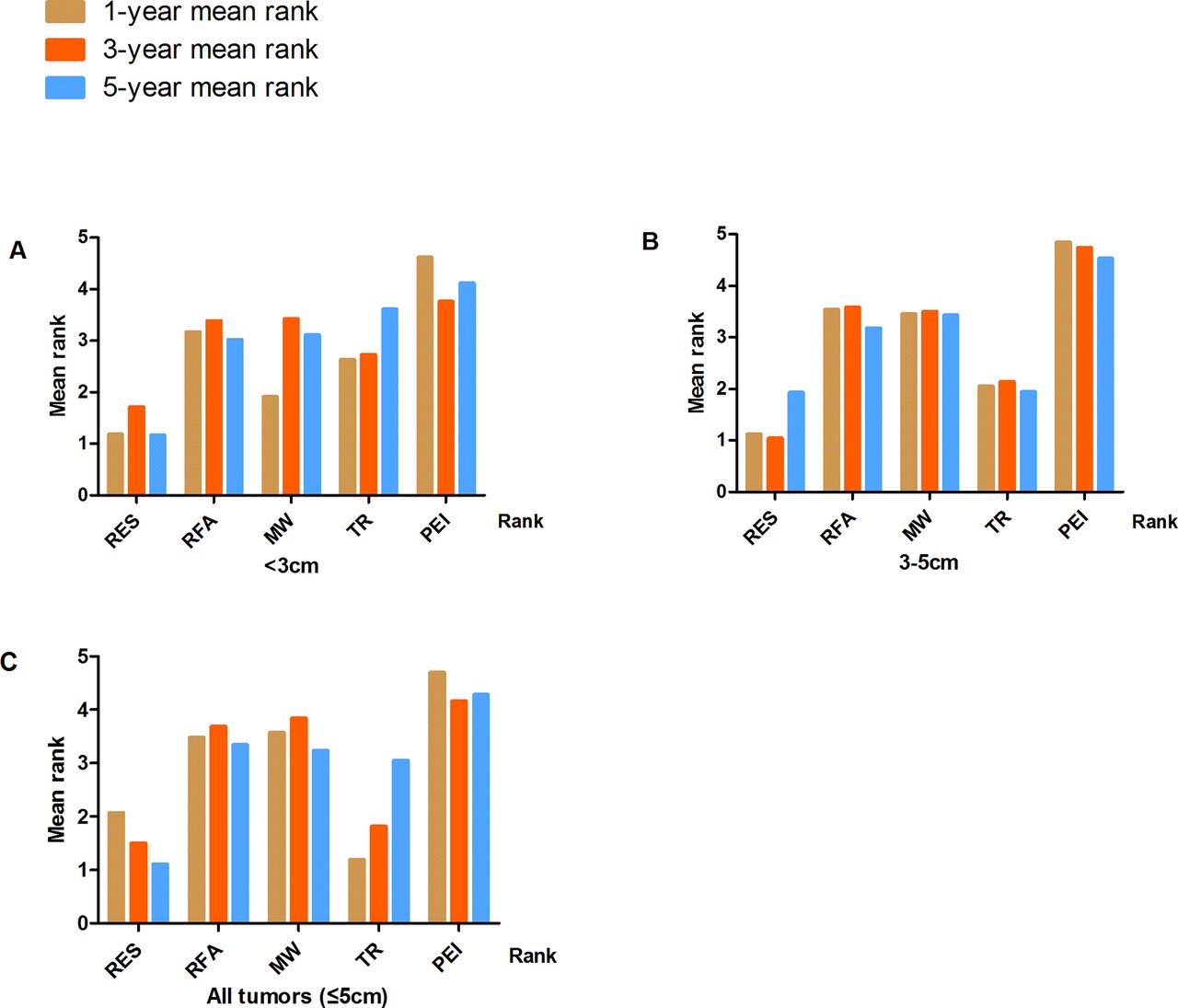
Survival probabilities (estimated using Meanrank) and ranks for the five treatments in patients with tumours <3 cm, 3–5 cm or ≤5 cm (with and without adjustment for study design) are graphically displayed in figures 2–5, and numerical details are given in online supplementary tables S3–S4. RES was consistently associated with greater survival (rank 1) compared with MWA, RFA, TR and PEI for the 5-year survival estimates. The ranks were similar for 1- and 3-year survival with RES or TR being ranked as 1 or 2 in most analyses. After adjustment for study design, and in the full sample of available studies (n=74), the treatments were ranked as follows for 5-year survival: (1) RES, (2) TR, (3) RFA, (4) MWA and (5) PEI (online supplementary table S4).

Treatment ranks for 1-year, 3-year and 5-year survival rates, according to lesion size in RCTs: (A) Lesions <3 cm. (B) Lesions 3–5 cm. (C) Lesions≤5 cm (full sample).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment ranks for 1-year, 3-year and 5-year survival rates, according to lesion size in all studies. (A) Lesions <3 cm. (B) Lesions 3–5 cm. (C) Lesions ≤5 cm (full sample).
Efficacy comparisons from network meta-regression for all treatments are summarised in tables 1 and 2, according to follow-up duration and initial tumour size. Compared with RES, the 5-year survival in all studies (trials and observational studies) for all tumours ≤5 cm, was 0.45 (95%CrI 0.23 to 0.82) for PEI, 0.59 (95%CrI 0.25 to 1.20) for TR, 0.55 (95%CrI 0.25 to 1.05) for MWA and 0.52 (95%CrI 0.29 to 0.88) for RFA (table 2). When examining the comparisons across all treatments, the only significant difference for tumours<3 cm was for 5-year survival, and a significantly worse survival was observed for PEI compared with RES 0.43 (95%CrI 0.17 to 0.89). For tumours between 3 and 5 cm, no significant differences were observed at 5-year survival, but significantly worse 3-year survival was observed with PEI, MWA and RFA compared with RES (table 2). Despite smaller number of studies in analyses of only RCTs, the pairwise comparisons showed similar results. However, all relative rankings should be interpreted with caution because most network meta-regression comparisons did not suggest a statistically significant difference between treatments. Detailed results of each comparison for survival rates were shown in online supplementary tables S5–S10.
ORs (95% credible interval) according to network meta-analyses for the survival for all pairwise comparisons in randomised controlled trials
ORs (95% credible interval) according to network meta-analyses for the survival for all pairwise comparisons in all studies
Loop-specific methods detected no inconsistency between the pairwise and network meta-analysis for most closed loops in the network (online supplementary figure S1). However, inconsistency was observed between direct and indirect comparisons for the following loops: lesions<3 cm: RES-RFA-TR, PEI-RES-RFA, MWA-RES-RFA; lesions 3–5 cm: MWA-RES-RFA, RES-RFA-TR; and lesions≤5 cm: RES-RFA-TR). In addition, tests for inconsistency were carried out (online supplementary tables S11–S13), which indicated a close relationship of between-trial heterogeneity and inconsistency between ‘direct’ and ‘indirect’ evidence.
Sensitivity analysis and publication bias
No significant change was observed when any one study was deleted. Funnel plots indicated that the included studies in each group were distributed symmetrically around the vertical line (x=0), suggesting that no obvious evidence of publication bias or small-sample effect existed in this network (online supplementary figure S2).
Discussion
There were many techniques for attaining a large ablated zone and complete necrosis of HCC and this comprehensive review addressed two of the more common treatments, namely resection and ablation. In this network meta-analysis, of the five examined therapies, the pooled data showed RES ranked best in full sample analysis with or without adjustment for study design. In both smaller (<3 cm) and larger tumours (3–5 cm), RES remained the highest ranking treatment. However, most of the individual treatment comparisons were not statistically significant and thus, RES may not be superior to all other therapies. Our evidence indicated locoregional therapies and particularly RES or TR (TACE+RFA) were associated with longer survival.
Our observation of better survival outcomes with TR may be through the advantage of dual mechanisms. With TR, TACE-induced hypoxic injury on cancer cells through occlusion of blood vessels and was followed by local ablation. This combination therapy may result in a larger ablated zone,97 reducing the possibility of micrometastasis and recurrence, and thus, resulting in better survival outcomes than RFA alone.
While being more invasive, and despite risk of complications, RES was associated with better survival outcomes after 1 year, 3 years and 5 years. This may be due to removal of larger sections of liver than can be targeted with locoregional therapies, thus removing a larger area of potentially cancerous cells. Additionally, rat models indicated that the liver has the potential to quickly restore its original size after partial hepatectomy. This may be mediated via interactions of lipopolysaccharide (LPS), tumour necrosis factor (TNF)α, interleukin (IL)−6, and transforming growth factor β (TGFβ).98 However, evidence from rat models and human studies indicated that resection success was associated with resection size and regeneration was stunted with larger resections.99–101 The safe limit for remnant liver volume in normal liver was approximately 30% of total liver volume, but this was estimated to rise to 40%–50% in those with liver disease.99 102 Liver resection was recognised as the most efficient treatment for HCC but was only applicable for less than 30% of all patients. However, developments in preoperative imaging techniques, laparoscopic surgery and newly developing combinations with chemotherapy may extend its application to more advanced tumours.102 Furthermore, the consistent associations observed with all studies and only in RCTs indicated that patient selection bias in the observational studies does not wholly explain the better survival outcomes with RES.
Overall, we found PEI was associated with shorter survival than the other four therapies, a finding which is supported in previous studies.24 33 One study reported RFA was superior to PEI in achieving short- and long-term survival outcomes, although PEI and RFA showed similar 5-year survival in lesions<3 cm.55 The possible reason why PEI is less effective than RFA may be because lesions often have a thick capsule and therefore ethanol may not distribute through tissues.
There are several limitations in this study. First, a major limitation is in the inclusion of non-randomised studies, in which selection bias is likely to confound observations. Selection of treatment is likely to be based on individual or tumour characteristics, and thus these factors will bias and confound observations of survival. Second, this study included both RCTs and observational studies, in which study designs and type of data collection may not be comparable. However, findings were consistent among both study designs. Third, all included studies did not report our primary outcome of interest (5-year survival) and this was a particular limitation among randomised studies. Fourth, for many individual comparisons, there were either no direct comparisons or comparisons from only a small number of studies. The lack of evidence may increase the risk of bias, which could enlarge or undervalue effect size, and may explain the small inconsistency seen between direct and estimated comparisons. Thus, we should be cautious in interpreting treatment rankings for the different survival times and for different size lesions. While adverse events from treatments may differ (not evaluated in detail in this review), by examining overall survival outcomes in our review, we have taken account of both long-term potential benefits and harms from treatments. The focus of these findings should therefore be on the overall observation that RES or TR may be superior in terms of survival, rather than focusing on specific OR values for individual treatment comparisons.
In conclusion, the findings of the current Bayesian network meta-analysis indicate that RES or TR may be among the most effective therapeutic approaches for HCC for 5-year survival in both smaller (<3 cm) and larger (3–5 cm) lesions. However, evidence was of variable quality, and the majority of evidence came from non-randomised studies, which are prone to selection bias and knowledge gaps still exist. For not, at the individual level, selection of strategies should depend on patient and clinical characteristics. To facilitate generation of evidence-based recommendations for HCC therapy, and to standardise treatment approaches, further head-to-head comparisons, especially of resection and ablative therapies, are required from high-quality RCTs, with long follow-up for survival outcomes.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
Footnotes
GT and SY are co-frst authors.
HC and LL contributed equally.
Contributors Conceived and designed the experiments: HC, T’J, LL. Performed the experiments: GT, SY, JY, DT, QZ, FC, T’J. Analysed the data: GT, SY, JY, QZ. Contributed reagents/materials/analysis tools: QZ, FC. Wrote the manuscript: GT, SY, T’J. Critically revised and approved the final version of manuscript: DT, HC, T’J, LL. Study supervision: HC, T’J, LL.
Funding This study was supported by the opening foundation of the State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, The First Affiliated Hospital of Medical College, Zhejiang University, grant NO. 2015KF06; This study was supported by the Foundation of Zhejiang Health Committee (2017KY346).
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.