Article Text

Abstract
Objectives To assess consistency in the format and content, and overlap of subject and timing, of medication safety letters issued by regulatory health authorities to healthcare providers in Canada, the USA and the UK.
Design A cross-sectional study comparing medication safety letters issued for the purpose of alerting healthcare providers to newly identified medication problems associated with medications already on the market.
Setting Online databases operated by Health Canada, the US Food and Drug Administration and the UK Medicines and Healthcare products Regulatory Agency were searched to select medication safety letters issued between 1 January 2010 and 31 December 2014. Format, content and timing of each medication safety letter were assessed using an abstraction tool comprising 21 characteristics deemed relevant by consensus of the research team.
Main outcome measures Main outcome measures included, first, characteristics (format and content) of medication safety letters and second, overlap of subject and release date across countries.
Results Of 330 medication safety letters identified, 227 dealt with unique issues relating to medications available in all three countries. Of these 227 letters, 21 (9%) medication problems were the subject of letters released in all three countries; 40 (18%) in two countries and 166 (73%) in only one country. Only 13 (62%) of the 21 letters issued in all three countries were released within 6 months of each other.
Conclusions Significant discrepancies in both the subject and timing of medication safety letters issued by health authorities in three countries (Canada, the USA and the UK) where medical practice is otherwise comparable, raising questions about why, how and when medication problems are identified and communicated to healthcare providers by the authorities. More rapid communication of medication problems and better alignment between authorities could enhance patient safety.
- health advisory letters
- direct healthcare professional communication
- potentially inappropriate prescribing
- medication management
- adverse events
- medication safety
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- health advisory letters
- direct healthcare professional communication
- potentially inappropriate prescribing
- medication management
- adverse events
- medication safety
Strengths and limitations of this study
Although previous studies have assessed the uptake and effectiveness of medication safety letters, we were unable to find any studies comparing the format and content or overlap of topic and timing, of medication safety letters across jurisdictions.
Through assessing consistency in the format and content, and overlap of topic and timing, of medication safety letters issued by regulatory health authorities in Canada, the USA and the UK to healthcare providers regarding newly identified medication problems and recommending a change in practice, we found that there was very little consistency between jurisdictions, raising questions about why, how and when medication problems are identified by health authorities as warranting a medication safety letter.
Although we checked for letters issued 6 months before and after the study period (1 January 2010 to 31 December 2014), it is possible that overlapping medication safety letters were issued outside of that expanded time frame.
The abstraction tool we used has not been formally validated and results may not be generalisable internationally given the focus on Canada, the USA and the UK.
Our study results suggest that patient safety could be enhanced by more rapid communication of medication problems and better alignment between national regulatory authorities.
Introduction
Medication safety letters (also known as ‘Dear Doctor’ or Direct Healthcare Professional Communication letters) are used by regulatory health authorities in many countries to communicate a variety of information to healthcare providers, including newly identified problems associated with medications already on the market. These letters are typically issued following the authority’s review of new information about the medication in question which is typically provided by pharmaceutical companies or by pharmacovigilance (spontaneous reporting) programmes. Once an issue is brought to light, often many years after the medication’s approval,1 there is a moral and ethical imperative to issue a medication safety letter to healthcare providers in a timely manner, in order to prevent poor health outcomes in patients. Understanding the choice of medication safety letter subjects, as well as their format, content and timing, is critical for effective risk communication.2
No standardised approach exists between countries for preparing medication safety letters, either in terms of their choice of topic, format or content, although the Medicines and Healthcare products Regulatory Agency (MHRA) has taken steps to standardise these letters within the UK, and within the European Union (EU), the European Medicines Agency (EMA) has also taken steps to standardise and harmonise them. Letters issued by authorities in similar jurisdictions are often structured differently and lack consistency in the amount and type of information they provide, even when dealing with the same medication problem. Little is known about how the format or content of a medication safety letter influences the likelihood that a letter will be read by providers or that it will lead to desired changes in practice. However, we do know that many medication safety letters do not effectively communicate relevant information to healthcare providers3 and that many healthcare providers are unlikely to change their practice after receiving them.4 For example, the Food and Drug Administration (FDA) has reported that only 13% of medication safety letter recipients can even recall receiving them.5 Furthermore, it is unclear what effect the information received from pharmaceutical companies or pharmacovigilance programmes may have on the quality of medication safety letters that may be subsequently issued by regulatory health authorities, or on their reception by healthcare providers.6
The ‘Dear Doctor’ project is a programme of research that aims to critically assess the format, content, evidence base, appropriateness and clinical impact of medication safety letters across three countries (Canada, USA, UK) that are similar in terms of their approach to practising medicine, linguistic profile and level of industrialisation. The objectives of the present study were twofold: first, to assess and compare the characteristics (format and content) of medication safety letters issued by regulatory health authorities in Canada, the USA and the UK to healthcare providers and second, to compare the overlap of topic and timing of their release across countries. Conceptually, the premise was that a letter should be included in the study if a healthcare provider would be prescribing without the most current and appropriate knowledge of the benefits and risks of a medication/condition if he/she was to miss that specific letter.
Methods
Patient involvement
Patients were not involved in this study.
Search strategies to identify medication safety letters
Online databases were searched to identify medication safety letters. Canadian letters were identified through Health Canada’s online database of recalls and safety.7 US letters were identified using the FDA’s online archive of recalls, market withdrawals and safety alerts.8 UK letters were identified using the UK MHRA’s Drug Safety Updates.9 Medication safety letters were included if they were written specifically to alert healthcare providers to newly identified medication problems and suggest a change in practice. Letters pertaining to devices and device companies or other medical-related products and companies were excluded. Letters were excluded if they did not pertain to the medication’s effect on the patient (eg, focusing instead on issues like the underfilling of vials, incorrect labelling or batch recall notifications), or if they were written to inform healthcare providers of a possible medication concern but were not yet suggesting a change in practice. Furthermore, letters were included regardless of whether a change in labelling was indicated or not. Finally, we did not include other types of safety alerts that were found on the regulators’ websites, such as alerts intended for the general public.
For the description of characteristics (first objective—format and content), we included letters published in the 5-year period from 1 January 2010 to 31 December 2014, inclusive. Two or three independent reviewers (SP, MH for Canada and the USA; DdL, MH and CDB for the UK) screened the medication safety letters identified in the search to evaluate their eligibility for inclusion. Where consensus could not be reached by these reviewers, an additional reviewer (LMB) provided input, and the final decision was reached by consensus. The same process was used for the analysis of overlap in terms of the topic (medication problem) and release date (second objective). To assess topic overlap between jurisdictions, the search was broadened to include medication safety letters issued 6 months before and 6 months after the 1 January 2010 to 31 December 2014 period in order to assess whether overlapping medication safety letters may have been released during this extended period. A 6-month window was considered a reasonable time period because the investigators agreed that it provided a balance between timeliness and allowing for expected bureaucratic lag.
In two cases, Health Canada issued a letter authored by the drug company that manufactured the described medication (Dabigatran Etexilate (published 12 December 2012) and Lithium (published 5 February 2014)), in addition to their own medication safety letter. In these two cases, the medication safety letters were written about the same medication problem and released on the same date as the company-authored letters, but included different basic characteristics. As the purpose of the study was to investigate how information is presented in medication safety letters issued by Health Canada, and these ‘duplicate’ letters differed in their format and content, both were included (four letters in total).
Abstraction tool used to describe medication safety letters
An iterative feedback process was used among research team members with expertise in clinical medicine, pharmacy, pharmacology, pharmacoepidemiology and public health, to achieve consensus on a list of clinically desirable medication safety letter characteristics, including aspects of content, format and timing with a focus on the medication problems that were the topics of medication safety letters and their corresponding release dates. An abstraction tool, consisting of 21 unique characteristics, was created using Microsoft Excel to facilitate identification and documentation of the presence or absence of these characteristics in each medication safety letter selected (table 1 for list of characteristics). Characteristics included general information about the medication safety letter and the medication at issue, as well as safety-specific concerns such as contraindications based on age or comorbidities, identification and quantitative information about adverse effects, interactions and dosing information. The characteristics were chosen to identify whether medication safety letters followed a particular structure. The introduction was thought to be important as it set the stage for recommendations with regard to practice change, and the presence of a clearly identified conclusion was thought to be important, as it might be the only section read by a busy practitioner wanting to focus on the core issue at hand. The abstraction tool was tested on a small sample of medication safety letters to ensure it effectively captured the information being sought.
Percentage of medication safety letters from each jurisdiction with listed characteristics
Information was abstracted from each medication safety letter using the abstraction tool. To assess for common content and format features of medication safety letters and to look for standardisation in these areas across jurisdictions, we conducted an overall comparison of medication safety letter characteristics, regardless of topic overlap (see table 1). Medication safety letters identified in the Health Canada, FDA and MHRA databases were cross-matched to identify medications that were the subject of the medication safety letters in more than one country. To be considered a match from a ‘topic overlap’ point of view, each letter was required to focus on the same medication problem for the given medication. For medication problems that were the topics of medication safety letters published in all three countries, their release date was compared.
Statistics
The percentages presented in the results are meant to describe the medication safety letters included in the present study, and not to treat them as a sample representative of a greater whole; therefore, only descriptive statistics were used, and we refrained from carrying out hypothesis-testing inferential statistics.
Results
Identification and selection of medication safety letters for inclusion
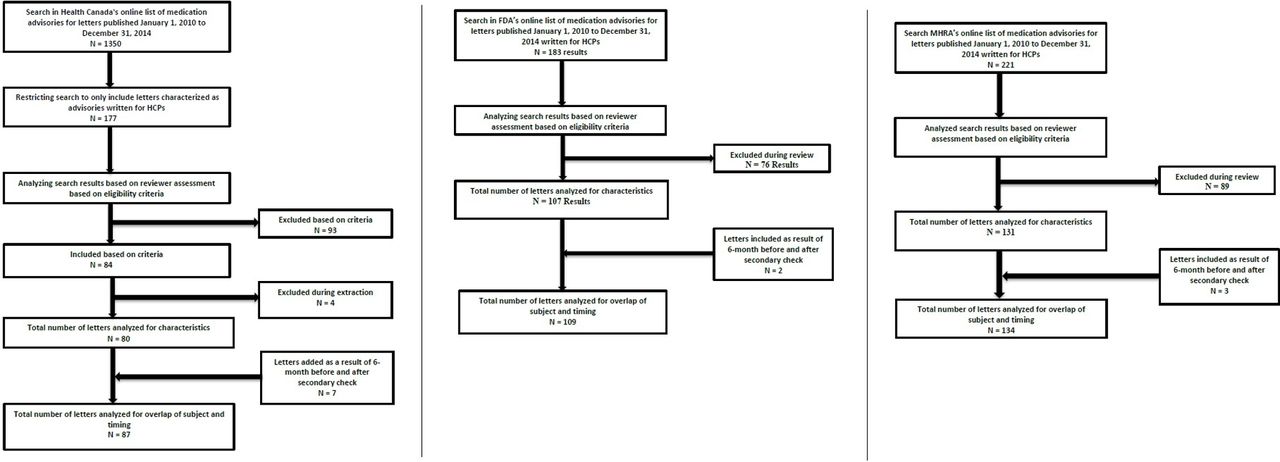
We included 45% (80/177) Health Canada, 58% (107/183) FDA and 59% (131/221) MHRA medication safety letters (total: 318 medication safety letters) published between January 2010 and December 2014 (figure 1). With respect to topic overlap, the additional search of each database 6 months before and after the study period identified 7, 2 and 3 (total: 12) additional letters published by Health Canada, the FDA and the MHRA, respectively. Therefore, the total of all letters included in the topic overlap analysis was 330. The content analysis (table 1), however, only focused on the 318 letters issued during the study period.
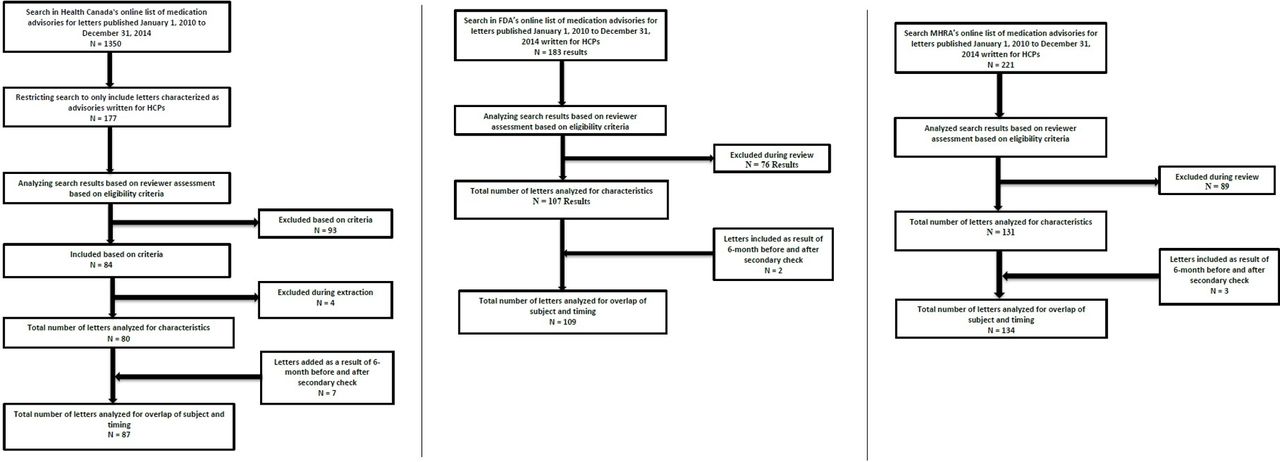
Process used to identify medication safety letters for analysis. FDA, Food and Drug Administration; HCP, healthcare professional communication; MHRA, Medicines and Healthcare products Regulatory Agency.
In evaluating the 330 medication safety letters included, while accounting for overlapping medication problems (ie, two or three letters, each from a different jurisdiction, addressing the same medication problem), a total of 243 dealt with unique medication problems identified during the study period, of which 227 (93%) pertained to medications available in all three jurisdictions. This included 93% (81/87) of Health Canada medication safety letters, 94% (103/109) of FDA and 93% (125/134) of MHRA. The degree of overlap between jurisdictions in terms of the subject of the medication safety letters was presented using a Venn diagram (figure 2).

Overlap in medication safety letters pertaining to medications available in all three jurisdictions issued in Canada between 1 July 2009 and 30 June 2015.
Comparison of medication warnings
Among the 227 unique medication safety letters that were identified in relation to a common set of medications available in all three countries, only 21 medication problems (9%) were the subject of letters released in all three countries; 40 (18%) in two countries and 166 (73%) in only one country (figure 2).
The 21 medication safety letters that were published by all three jurisdictions are presented in figure 3, along with differences in jurisdictional release dates using the Health Canada release date as a reference. No single jurisdiction was more likely than the others to publish first. The UK published first nine times, second six times and third six times. The USA published first eight times, second five times and third eight times, and Canada five, nine and seven times, respectively. Only 13 of the 21 medication safety letters that were common across all three jurisdictions were released within 6 months of each other (figure 3).

{kind=link}
{kind=link}
{kind=link}
Difference in release date (in months, relative to Canada) of UK and US medication safety letters.
The most extreme timing differences between jurisdictions related to: (1) elevated risks of cardiovascular-related events associated with the use of rosiglitazone released more than 3 years later in the USA than in Canada or the UK; (2) new dosage recommendations for simvastatin released in Canada 2.5 years after the UK and 1.5 years after the USA; (3) new warnings about renal risks associated with zoledronic acid released in the USA almost 1.5 years after the UK release, and 10 months after the Canadian release and (4) new dosing recommendations for zolpidem tartrate to reduce next-day impairment released in the UK 1.5 years after, and in Canada 1 year after, the US release.
Description of medication safety letter characteristics
Table 1 shows the prevalence of each of the 21 characteristics across the 318 medication safety letters that were analysed (excluding those included in the two additional 6 months ‘before and after’ periods, which were used only for the timing analysis). Some basic characteristics were common across jurisdictions. For example, 100% of letters analysed for each jurisdiction included the generic medication name, date of posting and name of the regulatory agency. None of the other 21 characteristics were present in all of the medication safety letters that were issued by each of the three jurisdictions. However, more than 85% of medication safety letters issued by each of the three jurisdictions included: the indications for the medication, the target population for the medication and the adverse effects associated with the medication.
There were differences between jurisdictions in what additional information was provided. Health Canada medication safety letters almost always included the author of the letter as well as the manufacturer, whereas these elements were rarely included in FDA letters and were consistently absent in MHRA letters. The FDA medication safety letters almost always included the scientific justification behind the letter (eg, a reference to a clinical trial or published research), the quantitative data about the adverse effects associated with the medication and links to additional information. These elements were included in less than 50% of the Health Canada and MHRA letters. The MHRA medication safety letters almost always included an introductory paragraph, whereas this was only found in two-thirds of Health Canada and less than a quarter of FDA letters. The MHRA and Health Canada medication safety letters also consistently included clear conclusions in the form of a summary paragraph or bullets, whereas the FDA letters included a clear conclusion in less than 20% of medication safety letters. Last, although present in a minority of letters, the MHRA medication safety letters were more likely than both Health Canada and FDA medication safety letters to include dosing information about the drug in question, and were more likely than Health Canada letters to describe the medication’s effectiveness in treating the indicated condition.
Discussion
Principal findings
Although one would anticipate that newly identified medication problems pertaining to medications already on the market in Canada, the USA and the UK would be relevant to healthcare providers and patients in all three countries, only 9% (21 out of 227) of these problems were the subjects of medication safety letters issued by all three regulatory health authorities during the time period considered for this study, and only 13 of those 21 letters (62%) were issued within 6 months of each other. These findings indicate that there is little overlap between what medication problems are chosen by different jurisdictions as warranting a medication safety letter, despite presumed availability of similar data.
Furthermore, our findings show evidence of significant time differences between jurisdictions for the issuance of warnings about some medications. This does raise questions about whether jurisdictions use different criteria and/or processes to decide when a medication safety letter is warranted, about how they communicate this information to each other and whether there are opportunities to standardise these decision-making processes across jurisdictions.
This is so despite existing communication mechanisms that are currently in place: For European countries that are part of the European medicines regulatory network, most of the transatlantic exchange of information is through the EMA which has regular teleconferences with FDA to share information on medicines safety.10 There are also interactions between the EMA and Canada.11
That said, while there have been substantial advances in collaboration across jurisdictions—for example, WHO Uppsala Monitoring Centre (https://www.who-umc.org/) provides access to monitoring data from the 127 countries that are members of WHO Programme for International Drug Monitoring, and the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use brings together regulatory authorities and pharmaceutical industry to discuss scientific and technical aspects of drug registration (http://www.ich.org/home.html)—with one exception (EU member states) regulatory agencies do not collaborate on licensing and communication of benefit and risks. This represents a substantial shortcoming of existing practice of pharmacovigilance. Our findings highlight that the current mechanisms of communication between regulatory agencies, although they exist, may be insufficient.
Furthermore, characteristics of medication safety letters issued by each of the three jurisdictions differed, indicating that there are differences in the format and content of medication safety letters issued by the different authorities. This raises questions about whether there are opportunities to better standardise the content and structure of medication safety letters across countries.
Strengths and weaknesses
Our study had a number of limitations. The abstraction tool we created, piloted and used has not been formally validated, and some readers may disagree with the characteristics included. Despite good inter-rater reliability, there remains a degree of subjectivity in assessing the characteristics that can have an impact on the results obtained. Nevertheless, this tool helped to demonstrate the variability of the content, format and timing of medication safety letters both within and across jurisdictions. Additionally, some of the domains identified in the abstraction tool would only be relevant to specific safety concerns, not others, and if the regulators differed in the safety concerns addressed, then there would be no real rationale for expecting them to cover the same types of safety concerns (eg, dosing, contraindications related to age, contraindications related to comorbidities, adverse effects, etc).
With respect to timing, a 6-month window was initially considered a reasonable time period for medication safety letters to be issued on the same topic in one or more of the three jurisdictions. Our findings indicate, however, that the actual time window is in fact much wider. It is possible that overlapping letters were issued outside the study time frame, as the secondary search to consider letters issued by each authority 6 months before and after the study time period, which was designed to correct for that possibility, did not significantly increase the degree of overlap between the three countries. Lastly, the study’s focus on Health Canada, FDA and MHRA medication safety letters may limit the broader international relevance of these results, particularly in non-English speaking countries. One would, however, expect, that overlap might be worse if comparisons were made across jurisdictions using different languages.
With respect to reproducibility, a further limitation arises from the fact that regulatory websites are regularly updated and restructured, and that older content is archived to repository databases. This makes it difficult to exactly reproduce search results for time periods that lie farther in the past. In our references to regulatory website data sources, we have endeavoured to provide links that are as specific and as current as possible, however, we are conscious that they may become obsolete in the future. Nonetheless, we think our study illustrates well the fact that consistency and communication about medication safety across jurisdictions remains a problematic issue worthy of further attention.
Comparisons with results of other related studies
We identified one study that examined the consistency of medication safety letters between countries within the EU with different languages and found substantial inconsistencies,12 but none that undertook a cross-jurisdictional analysis for countries sharing the same language. Studies examining the impact of medication safety letters have shown mixed results.13–15 Medication safety letters relating to dose changes and contraindications for citalopram and escitalopram issued in 2011 were studied by Schächtele et al, who found that simple information in a letter (the dose change) led to a change in prescribing habits, but more complex information (the contraindications) did not.16 An analysis of a series of medication safety letters relating to contraindications for the drug cisapride between 1995 and 2000 showed that the letter with explicit references to the contraindicated drugs was more effective at reducing prescriptions than the letter with example medications, which was, in turn, more effective than a letter listing implied medications.17 Additionally, in 2014, Thompson demonstrated that very few clinicians even recall receiving a medication safety letter,5 and Théophile et al demonstrated in 2011 that current medication safety letters are unlikely to change prescribing practices.4
Unanswered questions and future research
While it would seem reasonable to expect that regulatory health authorities in Canada, the USA and the UK might receive and disseminate similar information at similar times about newly identified medication problems associated with medications already available in all three markets, little is known about how regulatory health authorities determine why and when to issue a medication safety letter, or on what kind of information they base their decisions. This suggests that citizens may be put at risk if jurisdictions do not issue timely medication safety letters and/or jurisdictions may restrict treatment options with the potential for subsequent patient harm (and commercial implications) if they issue premature medication safety letters.
Although we are aware, through our informal networks and from the literature, that there is collaboration at different levels on a variety of topics between regulatory agencies, the present findings suggest potential opportunities for greater transparency in information-sharing and decision-making processes with respect to medication warnings. Future research should explore possibilities to standardise decision-making processes and optimise the content of medication safety letters to enhance the likelihood that providers act on these letters. In addition, further research would be needed to determine the extent to which collaboration between regulatory agencies is ongoing and effective. Finally, future research should examine the impact of different reporting priorities on (in)appropriate prescribing in each of these jurisdictions and, more broadly, on the practice of medicine and the protection of public health.
Conclusions
This study suggests that there are different decision-making processes and priorities between regulatory authorities in Canada, the USA and the UK regarding which medication problems warrant a medication safety letter, and a lack of consistency as to the content and timing, in particular, of advisories that are ultimately issued to healthcare providers. This indicates that healthcare providers in Canada, the USA and the UK may not have access to complete and timely information provided by their regulatory health authority about the medications they prescribe, relative to healthcare providers working in the other similar jurisdictions. There is a need—and a moral and ethical obligation—to ensure that policies and processes are in place so that healthcare providers have access to the information they need to prescribe or deprescribe, appropriately, and ultimately, to protect their patients from suffering avoidable adverse health effects related to the medications they use.
Acknowledgments
We would like to thank Katie Hood and Olivia Champagne for editorial support in the preparation of this manuscript.
Footnotes
Contributors LMB, DRM, JMG and MCW conceived of the idea and contributed to the development of the tool for the collection of data. LMB supervised the collection and analysis of data. SP, DdL, MH and CDB collected and analysed data. All contributed to the writing of the manuscript and its approval. In addition, all authors: 1. Contributed to drafting the work or revising it critically for important intellectual content; 2. Gave their final approval of the version to be published and 3. Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding DdL and SP contributed to this work with support from Undergraduate Research Opportunity Program (UROP) bursaries. For supervising their work, LMB also received some funding through UROP. Margaret Watson’s contribution was funded by a Leverhulme International Academic Fellowship and a Health Foundation Improvement Science Fellowship. JMG holds a Canada Research Chair in Health Knowledge Transfer and Uptake.
Disclaimer This study was otherwise unfunded and, therefore, no sponsors or funders had a role in the study design; collection, analysis or interpretation of data; writing of the report or in the decision to submit for publication.
Competing interests None declared.
Patient consent Not required.
Ethics approval This study did not involve human subjects and therefore did not require ethics approval. As this study was a review of publicly available literature/information, research ethics board (REB) approval was not necessary.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All available summary data have been included in this manuscript. PDFs of the actual medication safety letters are available on request from the corresponding author.
Author note Guarantor Statement: The lead author (guarantor) affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been explained.