Article Text

Abstract
Objective Compare vitamin D levels in opioid dependence and control population and adjust for relevant confounding effects. Nuclear hormone receptors (including the vitamin D receptor) have been shown to be key transducers and regulators of intracellular metabolism and comprise an important site of pathophysiological immune and metabolic dysregulation potentially contributing towards pro-ageing changes observed in opioid-dependent patients (ODPs).
Design Longitudinal prospective comparing ODPs with general medical controls (GMCs).
Setting Primary care.
Participants Prospective review comparing 1168 ODP (72.5% men) and 415 GMC (51.6% men, p<0.0001). Mean ages were 33.92±0.31 (mean±SEM) and 41.22±1.32 years, respectively (p<0.0001). Opioid use in the ODP has been previously reported and shown to be typical.
Interventions Nil. Observational study only.
Primary and secondary outcomes Serum vitamin D levels and relevant biochemical parameters.
Results Vitamin D levels were higher in the ODP (70.35±1.16 and 57.06±1.81 nmol/L, p<0.0001). The difference in ages between the two groups was handled in an age-matched case–control subanalysis and also by multiple regression. Sexes were analysed separately. The age:status (or age:time:status) was significant in case–control, cross-sectional and longitudinal analyses in both sexes (p<0.05). Modelled vitamin D was 62.71 vs 57.81 nmol/L in the two groups. Time-dependent mixed-effects models quadratic in age outperformed linear-only models (p=0.0377). ODP vitamin D was shown to vary with age and to correlate with alanine aminotransferase establishing it as a biomarker of age in this group. Hepatitis C seronegativity was significant in regression models (from p=0.0015).
Conclusion Vitamin D was higher in ODP in both sexes in bivariate, cross-sectional, case–control and longitudinal analyses and was robust to the inclusion of metabolic and immune biomarkers. That Hepatitis C seronegativity was significant suggests opioid dependence has an effect beyond simply that of its associated hepatitides. This finding may relate to the accelerated ageing process previously described in opioid dependence.
- vitamin D
- biomarker
- ageing
- opioid dependence
- heroin
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Strengths of this study included its large sample size, prospective and longitudinal design and real-world sampling in primary care.
The involvement of nuclear hormone receptor signalling in coordinating metabolic and immune systems provides an important insight into a major network of pathways which may contribute to the altered pathophysiological experience of drug dependent cohorts.
Study weaknesses included the unavailability of socioeconomic or occupational data which may impact on the amount of sun exposure derived from differing lifestyles and vocational exposure.
Vitamin D receptor assays and assays for the various vitamin D metabolites were also not available to this study.
Introduction
Vitamin D and its nuclear steroid receptor have been implicated in a wide range of physiological and developmental functions including skeletal, immunological, muscle strength and tendon function, metabolic syndrome and obesity, cardiovascular disease, endocrine disorders including diabetes, neuropsychiatric disorders, oncogenesis of several cancers, development and many cellular function.1–4 Many of these age-related morbidities are increasingly associated with opiate use.5–9 However, a literature search of the PubMed, Scopus and Ebsco Host online databases revealed no reports of the impact of opiate dependency on vitamin levels, other than a single report of its association with the adequacy of pain control in a cohort of patients with chronic pain.10
This whole area has recently been shown to be of enormous clinical importance by the increasing significance of vitamin D in multiple sclerosis11–17although this relationship remains controversial.18–20
The subject is of importance for several reasons. There are several reports of elevated rates of osteoporosis/osteopaenia in opioid-dependent cohorts.5 8 21 Higher levels of calcium, phosphate and their solubility product have previously been reported in opioid-dependent patients (ODPs).22
Increased vascular stiffness has also been reported in both male and female patients.7 23 It may be that higher levels of vascular stiffness—and vascular age—are causally associated with disruptions of vitamin D physiology. Moreover, a number of tumours have also been noted to be seen at higher incidence in ODPs24–26 which may relate to either altered nutritional, metabolic or immune factors. Chronic muscle and joint pain is also a common feature of opioid withdrawal which many dependent patients experience on a daily basis and is known not to respond to non-narcotic analgesics.10 27
The evidence from numerous sources is remarkably consistent and increasingly strong for a pattern of accelerated ageing in opioid dependence.7 23 Subcellular oxidative damage particularly arising from immune mechanisms is increasingly emerging as a principal determinant of ageing processes.28 29 As an important modifier of immune dysregulation,30–34 it is therefore plausible that vitamin D physiology may impinge on the ageing process in a clinically significant manner and may be of particular relevance to the immune dysregulation well described in opioid dependence35–39 and the accompanying syndrome of accelerated ageing.
Moreover, complex interactions are increasingly being documented between nutritional, immune, gastrointestinal and metabolic biomarkers40–42 making multiway interactions both analytically feasible and physiologically meaningful.43
The following study was therefore conducted prospectively to ascertain (i) the comparative levels of vitamin D in opiate-dependent and non-dependent clinical populations including sex differentials and comparative levels of hypovitaminosis D; (ii) to document the relationship of chronological age with changes in vitamin D status in dependent and non-dependent groups and therefore its role as a potential biomarker of ageing and (iii) to document significant associated changes in metabolic and innate and adaptive immune function with vitamin D levels. As our clinic sees significant numbers of both ODPs and non-dependent patients, we are ideally suited to compare opioid-dependent and non-dependent cohorts.
Methods
Patient selection
All ODPs and general medical controls (GMCs) attended a single metropolitan outpatient clinic, with data collected by retrospective review of patient records. All patients in whom a vitamin D assay was requested were included in the analysis. There was no selection of patients based on age. Hepatitis C serology was routinely only performed on opiate-dependent patients, and was used as a surrogate marker for retrospectively identifying opiate-dependent patients. Hence, patients were considered to be opioid dependent where the hepatitis C test was performed or the hepatitis C virus (HCV) RNA PCR test was positive. In a few cases, data were manually curated to correct anomalies. The two study groups are thus described as being ODPs and GMCs. Other blood tests were taken as clinically required in the process of routine medical care.
Pathology analysis
As a high rate of abnormally low vitamin D levels was quickly noted in all our patients, this test was ordered routinely on all patients who required clinical pathology to be performed. All clinical pathology was undertaken by the Queensland Medical Laboratory (QML) which is accredited by the National Association of Testing Authorities Australia to the Australian Laboratory standard AS-15189. QML is also accredited to the international standard ISO 9001 the international laboratory clinical standard. The form of vitamin D measured was 25-hydroxycholecalciferol. The calcium–phosphate solubility product was defined as is usual in chemistry as the product of the cube of the serum calcium concentration and the square of the phosphate concentration as previously described.22
Statistics
The pathology results were downloaded as an Excel spreadsheet from QML for the period 1995–2017. Data are listed as mean±SEM. Categorical data were compared in EpiInfo V.7.2.0.1 from Centres for Disease control in Atlanta, Georgia, USA using the adjusted Mantel-Haenszel statistic. Bivariate statistics were compared by categories in Statistica V.7.1 from Statsoft, Oklahoma, USA. Student’s test for t with separate variances was utilised as indicated by the Levene test. This is reported in table 1 as fractional df.
‘R’ V.3.3.2 was downloaded from the University of Melbourne Central ‘R’ Archive Network mirror. Multiple regression was performed in ‘R’ and graphs were drawn in R using the ggplot2 package. Loess (localised polynomial curves) were drawn at a span=0.95. Multiple regression model reduction was performed by the classical method with deletion of the least significant term until only significant terms remained. Deidentified confidential data may be made available to interested readers and researchers on written request to the authors. Continuous data of such as vitamin D, alanine aminotransferase (ALT), serum globulins and C-reactive protein were log transformed in multiple regression analyses as indicated by the results of the Shapiro test. Chronological age was not log transformed in the interests of improving model fit. Linear and polynomial models were compared using analysis of variance (ANOVA) tests in R. Missing data were case-wise deleted. All t-tests were two tailed. p Value <0.05 was considered significant.
Ethics
Strict patient confidentiality was maintained throughout the data analysis phase. The study was conducted in accord with the Declaration of Helsinki.
Results
In the period 1995–2017, 1583 patients had a vitamin D study performed on 2099 occasions. Of these, 1168 patients were treated for opioid dependence and 415 patients were treated for general medical conditions. It is noteworthy that 98% of this study was sampled prior to the introduction of universal coverage for hepatitis C treatment in Australia in March 2016.
Overall, there were 1061 men and 522 women. Out of 1168 ODPs, 847 (72.52%) were men and out of 415 GMCs, 214 (51.57%) were men (Mantel-Haenszel χ2=60.77, p<0.0001). In the longitudinal sample including repeat tests, 1031/1437 (71.75%) of opioid-dependent samples were from men and 350/662 (52.87%) of the general medical samples were taken from men (Mantel-Haenszel χ2=71.72, p<0.0001).
Patients were considered to be hepatitis C positive if either the HCV antibody or their serum PCR study was positive for hepatitis C RNA. Among the ODPs, 301 were hepatitis C antibody seronegative and 867 were antibody positive. Among the medical controls, 406 were untested, 1 was seronegative and 8 were positive. Hence, 74.23% of the ODPs were hepatitis C seropositive, compared with only 1.93% (8/415) of the GMCs (Mantel-Haenszel extended χ2 test for trend=12300.10, p<0.0001).
Table 1 gives the initial bivariate cross-sectional comparative data for selected laboratory parameters. In particular, one notes a significant difference in chronological age between the opioid-dependent and general medical groups 33.92±0.31 versus 41.22±1.32 years (mean±SEM, t=5.38, sep. var. df=194.71, p<0.0001). Several of the liver tests are higher in the opioid-dependent group. Some of the lipid parameters are lower likely reflecting a lower body weight as has previously been reported in patients from this cohort.7 Drug use data in this cohort have been previously reported.7 23 44–46
One notes that the vitamin D level is much higher in the ODPs 70.35±1.16 vs 57.06±1.81 mmol/L than in the GMCs (t=6.19, sep. var. df=334.41, p<0.0001). Low levels of vitamin D (<50 nmol/L) were less frequent in the ODP group than in the GMC group (27.48% vs 45.3%, OR=0.46, 95% CI 0.36 to 0.58, Mantel-Haenszel χ2=44.53, df=1, p<0.0001).
Vitamin D levels in the cohort is charted by age in figure 1A,B and by time in figure 2 (see the online supplementary figure 1) provides a similar plot to figure 1A but is drawn with loess curves which closely approximate straight lines, confirming the utility of linear modelling in this analysis. The effect of time is shown in the online supplementary figure 2, where it is shown that linear modelling approximates the effect of passing time less well.
Supplementary file 1
Supplementary file 2
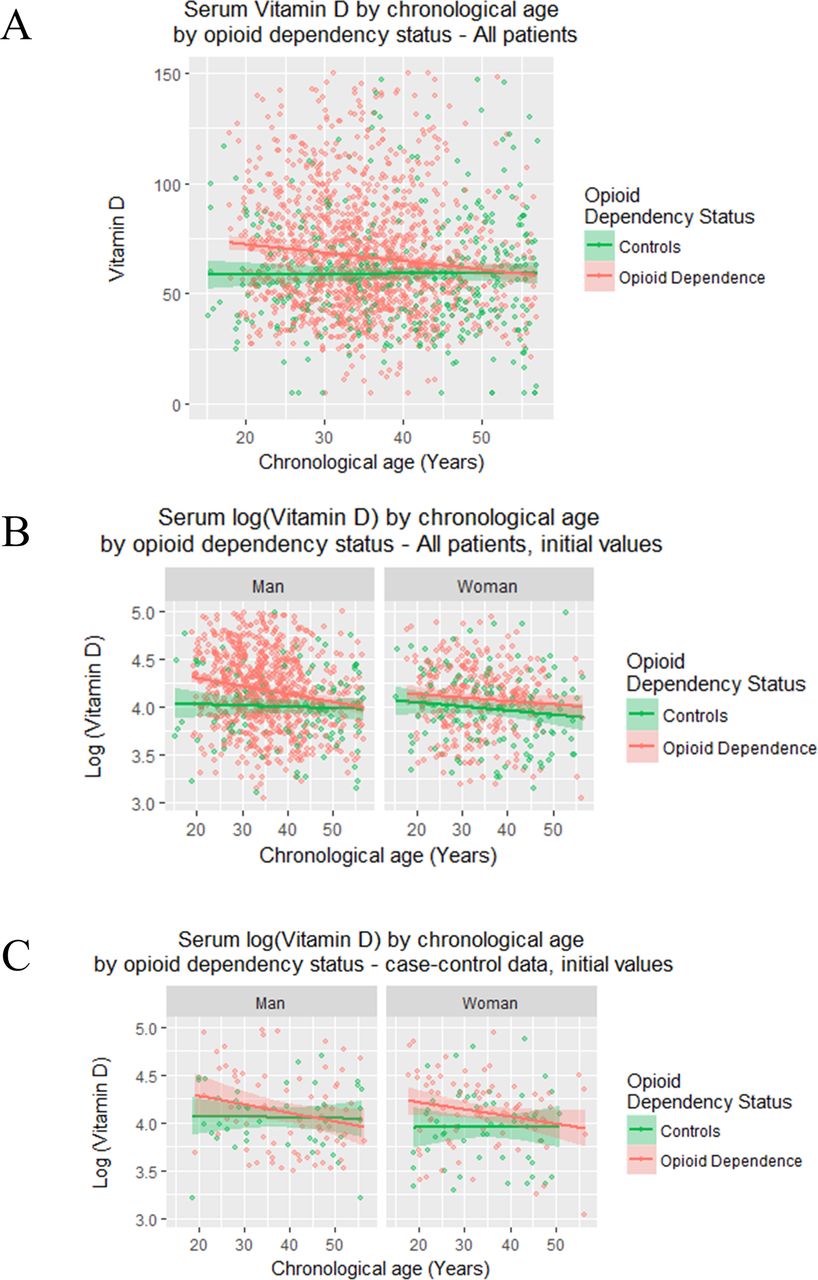
Vitamin D and log vitamin D by chronological age, opioid dependency and sex in (A) whole cohort, (B) initial values and in (C) case–control study.
ALT is a well-recognised clinical biomarker of metabolic ageing.39 47 (Log) vitamin D level was shown to correlate with the (log) serum ALT in opioid dependence both in the cross-sectional initial group (Spearman R=0.0951, t=3.26, df=1166, p=0.0011) and the longitudinal group (Spearman R=0.0984, t=3.75, df=1435, p=0.0002). This correlation was not significant among GMCs. Another biomarker, serum globulin, was not significantly correlated with vitamin D in any group.
These figures show a clear age effect. Hence, the very different ages in our two major groups may have had an effect on the parameter of interest. This age disparity was addressed in two ways. First by using a case–control comparison group from within the larger group, and second by using multiple regression and correcting for the effects of chronological age.

Serum vitamin D status by time in (A) first 3 years and (B) across whole period.
Case–control series
In the case–control study, it was possible to pair 331 GMCs with 331 ODPs by age. The age of the ODPs was 40.07±0.62 years and that of the GMCs was 40.34±0.64 years (Student’s paired t-test t=7.13, df=330, p<0.0001). The mean difference in ages was 0.26 years. However, the ages were not significantly different if a non-paired t-test was used (t=0.29, df=660, p=0.76). In 20 of the 331 pairs (7.5%) the age difference was >|1|; and in 49/331 pairs (14.8%) the age difference was greater than an absolute difference of |0.5|. The comparative age distributions are shown in superimposed histogram and contour plots (see the online supplementary figure 3).
Supplementary file 3
While the two groups had a similar sex ratio, being 50.76% and 51.36% men, respectively (Mantel-Haenszel χ2=0.2, p=0.87) they were not sex-matched at the single pair level (Wilcoxson W=53 464, p=0.82).
Bivariate comparisons—initial cross-sectional data
Selected bivariate parametric comparison from the case–control cohort are shown in the lower part of table 1.
The mean vitamin D in these two groups was 64.24±1.52 and 59.73±1.66, respectively (Student’s paired t-test t=5.57, df=330, p<0.0001). These values are charted for the initial cross-sectional group in figure 1C.
When the (log) vitamin D status was regressed against age in a linear regression model in each case the age: addictive status interaction was significant in all patients, and in women (top half of table 2). The age: status interaction approached significance in men (p=0.066). In a linear model quadratic in age, both the addictive status and the age squared:status interaction were significant (table 2). The model quadratic in age was superior to the model linear in age (F=3.422, df=3, p=0.0178).
When the (log) vitamin D level was regressed against age and time in a mixed-effects model using restricted maximum likelihood modelling techniques, the addictive status was significant both in its own right (p=0.0009) and in interaction with age (p=0.0180), as show in the top of table 3. In a model quadratic in age, the addictive status was significant (p=0.0004) and it was also significant in interactions with age and time (from p=0.0021). The model quadratic in age was superior to the model linear in age (log ratio=14.80, df=5, p=0.0112).
Multiple regression in the whole dataset
We then move on to the whole dataset first looking at the initial cross-sectional values. In these studies, the (log) vitamin D level is regressed against age and addictive status. These results are summarised in the lower half of table 2 which found significant differences by group and by sex.
The effect size between the two groups can be calculated from this model. When one enters the median age (35.83 years) for the cross-sectional dataset in the regression model, the modelled levels of vitamin D are 62.71 and 57.81 nmol/L in the ODP and GMC groups, respectively. This represents a 4.90 nmol/L difference or 8.47% advancement on the level in the control group.
Age-dependent linear regression cross-sectional analyses
A model quadratic in age was also calculated for the initial cross-sectional data with results shown in the lower half of table 2. However, on formal testing, it was not superior to the strictly linear model (F=1.7085, df=2, p=0.1815).
When all the data (n=2099) are considered in a time-dependent mixed-effects model, the results shown in the middle portion of table 3 are obtained. In these models, the (log) serum vitamin D levels is regressed against age, time and drug dependence status with the case number as the random effect. A similar model was calculated quadratic in age with results shown at the top of table 3. It was found to be superior to the linear model (log ratio=8.445, df=3, p=0.0377).
Mixed effects final longitudinal models
One notes that when sex is included in the model the age:time:status interaction is significant. Sex is included in one term in the final model. The age:status interaction is significant when all patients are considered together and in men and women separately. In women, this appears as an interaction between time, age and status. These results imply that vitamin D is a biomarker of age.
No correlation between vitamin D status and the calcium–phosphate solubility product in the whole sample was demonstrated (Pearson R=0.019, t=0.86, df=2044, p=0.39).
In previous studies, the serum globulins and ALT have been the most discriminative clinical pathological variables and these parameters also show marked age-dependent effects.39 48 49 Therefore, these results were included in time-dependent mixed-effects linear regression models for all patients and for each sex separately. The outcomes of these analyses are shown in the lower part of table 3. In each case, the addictive status is significant.
The demonstration that ALT and serum globulins are close correlates of the elevated vitamin D in opioid dependence raises the question of the possible relationship of liver disease with this observation. Preliminary analyses showed that the hepatitis B serostatus was less discriminatory than hepatitis C serostatus, so the analysis in this section focused on hepatitis C. Note that in this study, technical factors may blur the definitions of the opioid dependence status and hepatitis C serostatus as in the present work, as elsewhere,37–39 49–53 the opioid dependence status was defined in terms of the hepatitis serological results.
The results are as shown in figure 3 where the majority of the effect seems to reside with the hepatitis C-positive group. This is formally confirmed by regression analysis results shown in the first segment of table 4. However, as shown in the lower panels of figure 3, some of the data for the hepatitis C serostatus is apparently non-linear. Therefore, low-order models polynomial in age were compared with the linear model. The results of the model quadratic in age are shown in the lower section of table 4. Formal model comparison using ANOVA testing confirmed that the model quadratic in age was superior to the linear model (log ratio 19.83 on 5 df, p=0.0013). A similar model quadratic in time failed to converge. A model quadratic in both age and time also failed to converge.

![[bmjopen-2017-016806-SP1.jpg]](https://bmjopen.bmj.com/content/bmjopen/8/1/e016806/DC1/embed/inline-supplementary-material-1.jpg?download=true){kind=link}
![[bmjopen-2017-016806-SP2.jpg]](https://bmjopen.bmj.com/content/bmjopen/8/1/e016806/DC2/embed/inline-supplementary-material-2.jpg?download=true){kind=link}
{kind=link}
{kind=link}
![[bmjopen-2017-016806-SP3.jpg]](https://bmjopen.bmj.com/content/bmjopen/8/1/e016806/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
Logarithm vitamin D by hepatitis C serostatus by: (A) age and sex using linear lines of best fit; (B) age and sex using loess (localised polynomial) curves of best fit and (C) over the first 3 years by sex.
Mixed effects final longitudinal models by hepatitis C serostatus
A complete mixed-effects model of the multiple regression correlates of serum vitamin D was therefore constructed including age, time, ALT, globulins and hepatitis serostatus were included in the model and reduced by the classical model reduction procedure. Because of the superiority of the quadratic model in the more streamlined analysis described in the preceding paragraph, this model included a term quadratic in age. Sex was not included in the final model as it was not significant in the applicable preceding model as noted above. The final model derived by this procedure is shown in the third section of table 4. In this final model, the only parameter which was independently correlated with serum vitamin D was the serum ALT level. No quadratic term in age was significant in the final model. Interestingly, notwithstanding the inclusion of both globulins and ALT, the hepatitis C serostatus was significantly correlative and was included in 8 of the 12 terms in the final model. Terms including hepatitis C seropositivity were significant from p<0.0001 and terms including hepatitis C seronegativity were significant from p=0.0475.
This final model was shown to be superior to the preceding quadratic model without biochemical parameters included by ANOVA testing (log ratio=19.53 on df=9, p=0.0021).
Discussion
The main results of this prospective longitudinal study were that the serum vitamin D levels in ODPs were higher than that in the general medical controls both as a mean level overall and in multiple regression models by dependency status and/or by the age: dependency status interaction in both sexes. The advance in the modelled vitamin D level with age was shown to be 8.47%. The vitamin D level did not change with age in the control group, but it did fall significantly with age in the opioid-dependent group, making it a negative biomarker of ageing in this group. It was also shown to be significantly correlated with ALT, a well-recognised biomarker of age. Many differences exist between the ODPs and GMCs, however the effect appeared to be robust to adjustment for many of these features. While hepatitis C was an important predictor of the vitamin D level, it did not account for the effect of opiate dependency, as it was also observed in the HCV seronegative group. On multivariate analysis, vitamin D level was found to be significantly associated with interactive terms including ALT and measures of immune function such as serum globulins. The reasons for the higher levels of vitamin D in the opioid-dependent group are not clear and the present work is not designed as a mechanistic exploration. Unpublished data from this cohort show that the socioeconomic profile of the ODP and GMC groups is very different, with many more tradesmen and welfare-dependents in the ODP group which might be expected to have higher and lower than normal sun exposure, respectively. The primary analyte in this study was 25-hydroxyvitamin D. As the 25-hydroxylation reaction occurs photolytically in the skin, it may be that the higher vitamin D level in the ODP in this study reflects increased occupational exposure. It should be noted that the study was conducted in Queensland, Australia which has such a high incidence of skin malignancy that it is commonly referred to as the ‘melanoma capital of the world’.54 Opioids are well known to have various endocrine35 50 53 55–57 and immune potentiating actions35–38 49 51 58 which have been addressed elsewhere and it is possible that indirect effects on vitamin D metabolism may be mediated through such pathways. Moreover, the relationship with vitamin D status and the square of chronological age was fascinating and suggests a positive feed forward process as has been found for arterial stiffness in various drug dependencies.7 59 60
Although both elevated levels of vitamin D on the one hand (present report) and calcium and phosphate and their solubility products on the other hand22 have been noted in our patients in opioid dependency, as no correlation was established between the two sets of parameters, it is unlikely based on the present analysis that a direct relationship exists between them. However, as the vitamin D-binding globulin (VDBG) has not been measured in the present work, it may be that this provides the computational and mechanistic ‘missing link’ between the two groups of data. Moreover as the vitamin D binding globulin (VDBG, Group Specific Component Globulin, gc component, gc globulin) is generated in the liver61 62 and liver dysfunction has been well described both in opioid dependency and in HCV infection, this is an important issue for future workers in this area. At the time of writing however, we are not aware that such assays are available in this country. Parallel analyses have found that this situation is of particular relevance to the case of the circulating levels of sex hormones and their binding globulin in men and women in our cohort53 and it may well be the case therefore in the case of vitamin D physiology. It is important to underscore that the highly significant results obtained in the present analysis for the patients with hepatitis C seronegative opioid dependency imply that hepatic dysfunction alone is not likely to account for the observations reported herein. Biomarkers of ageing have been reported to be derived from any variable which changes with age.39 Such biomarkers can change in either a positive or negative direction with age. Both ALT and globulins rise dramatically with age and so have been described as positive age-related biomarkers.37 38 49 51 63 In the ODPs described in the present study, vitamin D levels fell with age which would make vitamin D a negative biomarker of age in the drug-dependent cohort (tables 2–4, figures 1 and 3A,B and see the online supplementary figure 1). Moreover, vitamin D status was also shown to correlate with ALT in drug dependence which is a well-established biomarker of ageing.
Interestingly very high levels of osteoporosis/osteopaenia have been noted in ODP groups by several authors.5 64–66 Clearly the higher levels of vitamin D seen in this study are not in accordance with such a finding. However, an inverse effect may be mediated by either a higher level of VDBG or a block to the metabolism of vitamin D to the active form 1,25-dihydroxycholecalciferol. Such a finding must await further studies. Moreover, the generally immunologically activated milieu of opiate dependence is now increasingly well characterised.35 37 39 49 63 It may be that the immune active environment, with higher levels of interleukin-1, interleukin-6, tumor necrosis factor-alpha and Monocyte Chemotactic Protein 1/Chemokine (C-C motif) Ligand 2 (MCP-1/CCL2) among other key cytokines,67 is the dominant force acting on bone mineralisation and overwhelms any relatively minor effect related to vitamin D metabolism. Interestingly melanocortin receptor-1 has been identified in the skin.68 P53-induced photoactivation of pro-opiomelanocortin synthesis has been shown to be linked with cutaneous β-endorphin release, elevated pain thresholds and naloxone-inducible withdrawal after sun exposure. It is therefore potentially possible that ODPs may be self-medicating the possibility of withdrawal by elevating their rate of sun exposure.69 Further intriguing conceptual possibilities emerge. Opioid dependence is characterised by a subtle disruption of normal metabolism39 70 to the extent where patients have been compared with prediabetics.50 56 71 72 Moreover, and in common with many addictions, opioid dependence is characterised by a marked immune stimulation36 37 39 58 73 and simulation or at least phenocopying of the ageing process.6 7 9 39 45 74 It turns out that nuclear hormone receptors (NHRs) of various classes facilely integrate such immunometabolic signalling.75–80 NHRs of the oestrogen, androgen, pregnane, peroxisome proliferator activator receptor, liver X receptor and rexinoids are involved along with the vitamin D receptor.75 78 79 Importantly, there is significant heterodimerisation and apparent promiscuity with many of these receptors81–83 including the vitamin D receptor84–90 and involvement of these pathways in diverse cell processes including stem cell regeneration,91–96 atherogenesis78 97–101 and cancer.83 102–106 As altered metabolism, immunosenescence, cancerogenesis and stem cell failure are all well described in the ageing literature,28 29 107–109 it would appear that pathophysiologically, phenotypically and clinically important processes may be impacted by the changes reported in the present paper.
This study had various strengths and limitations. The large sample size, prospective design, longitudinal nature and real-world sampling for the groups were major strengths. As the study was taken from ‘real-world participants’ and as the opioid use has previously been shown to be typical of that reported in many other clinical series, we feel that these results may be generalisable to opioid-dependent populations elsewhere. As the drug use data were not available in these patients, it was not possible to compare drug use levels with vitamin D status or calculate dose–response relationships. Similarly, anthropometric including body mass index data and sun exposure information is not available. The extent of vitamin D supplementation used by patients is also unknown, but it is believed that its use would be more widespread among controls than in ODP, thereby acting in the reverse direction. Socioeconomic and occupational data were also not available to the present study. While every attempt has been made to adjust the findings for measured confounding variables, the involvement of unmeasured confounding in the present results is not known. Nevertheless, the robustness of the present findings to various data manipulations including longitudinal and multivariate adjustment suggests that the finding is genuine. These findings could be supported by future mechanistic and interventional studies. The unavailability of VDBG assay or studies of vitamin D nuclear receptor to the present work were limitations.
In summary, the present work quantitated vitamin D status for the first time in a patient cohort dependent on illicit opioids and demonstrated higher vitamin D levels in the opioid-dependent group both as a group mean, in case–control and after adjustment for age, sex and selected laboratory markers in various linear regression models. The modelled level was 8.47% higher in the OPD than in controls. The effect was not simply attributable to hepatitis C infection. The cause of this elevation was not clear from the present report. Vitamin D levels fell with age in ODPs, making it a negative biomarker of ageing in this cohort. This finding is of interest due to the described involvement of NHRs (including vitamin D receptor) with inflammatory and metabolic pathways which may be of clinical significance and may relate to the well-described ageing phenotype observed in opioid-dependent populations. Future studies should consider including detailed parametric drug use histories, occupational exposure to sunlight and measurement of VDBG or vitamin D receptor activity and active vitamin D metabolites in further exploring this issue.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
Footnotes
Contributors ASR: designed the study, performed the analysis, prepared the figures and wrote the first draft of the paper. GKH: wrote and the final draft and assisted with the statistical analysis.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study was given ethical approval by the Human Research Ethics Committee of the Southcity Medical Centre which has been accredited by the National Health and Medical Research Centre.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data for this paper may be obtained from the authors upon specific request.