Article Text

Abstract
Objective To evaluate the effectiveness of a nurse-supported self-management programme to improve social participation of dual sensory impaired older adults in long-term care homes.
Design Cluster randomised controlled trial.
Setting Thirty long-term care homes across the Netherlands.
Participants Long-term care homes were randomised into intervention clusters (n=17) and control clusters (n=13), involving 89 dual sensory impaired older adults and 56 licensed practical nurses.
Intervention Nurse-supported self-management programme.
Measurements Effectiveness was evaluated by the primary outcome social participation using a participation scale adapted for visually impaired older adults distinguishing four domains: instrumental activities of daily living, social-cultural activities, high-physical-demand and low-physical-demand leisure activities. A questionnaire assessing hearing-related participation problems was added as supportive outcome. Secondary outcomes were autonomy, control, mood and quality of life and nurses’ job satisfaction. For effectiveness analyses, linear mixed models were used. Sampling and intervention quality were analysed using descriptive statistics.
Results Self-management did not affect all four domains of social participation; however. the domain ‘instrumental activities of daily living’ had a significant effect in favour of the intervention group (P=0.04; 95% CI 0.12 to 8.5). Sampling and intervention quality was adequate.
Conclusions A nurse-supported self-management programme was effective in empowering the dual sensory impaired older adults to address the domain ‘instrumental activities of daily living’, but no differences were found in addressing the other three participation domains. Self-management showed to be beneficial for managing practical problems, but not for those problems requiring behavioural adaptations of other persons.
Trial registration number NCT01217502; Results.
- dual sensory loss
- long-term care
- licensed practical nurses
- self-management
- social participation
- geriatric nursing
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- dual sensory loss
- long-term care
- licensed practical nurses
- self-management
- social participation
- geriatric nursing
Strengths and limitations of this study
Recently, many studies have confirmed the increasing incidence of dual sensory impairment among the ageing population; however, the psychosocial interventions aimed at supporting these older adults in daily activities have not been evaluated.
The power of this study lies in the interaction and alignment between dual sensory impaired older adults and their familiar nurse when addressing the problems perceived by the older adult in their daily lives.
The two types of diaries kept by the nurses gave the research team an overview of the performance of the intervention in daily care situations.
Rapidly changing policies for admission in long-term care facilities challenged the recruitment of participants in this study, leading to a high incidence of dual sensory impaired older adults who were unable to participate due to their advanced stage of cognitive problems.
Background
We are currently seeing a rapid growth in the prevalence of dual sensory impairment (DSI) in long-term care (LTC) populations in Europe; from 12% in 2007 to 33.9% in 2016.1 2 The co-occurrence of an age-related hearing and visual impairment predominantly affects people aged 80 years and above.3 4 DSI is highly associated with social participation problems.5 6 Barriers in communication and access to information reduce the ability of those with DSI to participate and align with others. It makes it difficult for them to interact, to make choices and to undertake activities. Consequently, DSI is a threat for the social health of older adults,7 and it increases the risk that they withdraw within themselves and become dependent on others.8
Usual care focuses on either hearing or visual impairment, and mostly comprises medical treatment, technical device provision and psychosocial rehabilitation interventions. Unfortunately, the extent to which usual care succeeds in addressing sensory impairment in old age is limited.9 The literature shows however, that in LTC, the occurrence and impact of hearing and visual impairment are often overlooked.10 11 Moreover, living in LTC causes a variety of conditions that negatively affect the participation of hearing and visual impaired persons, such as the multiplicity of people, noise, confusing social encounters and logistics.12 13
Despite the increasing prevalence of DSI, psychosocial interventions to support DSI older adults are still scarce. Two studies aiming to improve hearing aid or sensory-specific service use among DSI older adults showed a modest beneficial effect on handling hearing aids, and on facilitating access to the appropriate hearing technologies and rehabilitation services, respectively.14 15 However, there is a lack of intervention studies aiming to improve DSI older adults’ social participation and alignment with others in daily life. Research showed that self-management interventions had beneficial effects on social participation among patients with chronic illnesses.16 A systematic review of controlled intervention studies showed beneficial effects of self-management interventions for older people with visual impairment.9 The review also showed that self-management interventions using a problem-solving approach had a modest beneficial effect on quality of life of the visually impaired older adults,17 18 whereas educational approaches showed no effect.19 20 In self-management interventions using a problem-solving approach, older adults are encouraged to discuss strategies for the problems that bother them most, and to explore solutions that fit them and their personal circumstances.21 In contrast, in self-management interventions using an educational approach, experts teach individuals to recognise the negative symptoms of their disease and to choose from a package of alternative solutions.22
In the Netherlands, LTC homes offer a sheltered care and living environment to older adults who suffer from physical and/or cognitive conditions and who are in need of professional care and on-site surveillance at frequent intervals throughout the day. Usual LTC care as defined by the government covers four domains: physical well-being, mental well-being, a safe living environment and participation. The latter aims at providing attractive opportunities to participate in personal hobbies and interests, and to enable a social life with other residents and the social network. Nurses in usual care have two mediating roles in social participation, by bringing residents together, based on the rationale that proximity creates opportunities for contact and participation, and by scheduling volunteers who support the older adults with their hobbies.23 In the once-a-year or twice-a-year care plan meeting, the person’s individual wishes and needs are noted for each domain. Licensed practical nurses, under supervision of registered nurses, provide the majority of assistance with activities of daily living and on-site surveillance. Their frequent daily encounters with DSI older adults place the licensed practical nurses in an outstanding position to provide psychosocial support. However, they are taught very little about how best to provide this type of support when at school or at work.24 This in turn can lead to less pleasure in their work and a higher rate of job loss.25
There is a need to investigate how DSI older adults can be supported to address their barriers in social participation and alignment with others in daily life. To respond to this need, we developed the nurse-supported Self-Management Programme for Dual Sensory Impaired Older Adults (SMP-DSI). In addition, we developed an SMP-DSI training programme for licensed practical nurses, aiming to train and coach the nurses to support the DSI older adults using the SMP-DSI. Thereafter, we set up a cluster randomised controlled trial (cRCT) to compare the effectiveness of the SMP-DSI versus usual care in LTC. Due to the multiple and competitive demands placed on LTC nurses, psychosocial interventions such as self-management performed in routine care settings are sensitive to implementation errors, which can impact the intervention quality.26 Therefore, in parallel with this cRCT, we conducted a process evaluation evaluating the sample and intervention quality of the trial. Finally, as the training programme may influence the job satisfaction of the participating nurses, we added job satisfaction as an outcome for the nurses.
We hypothesised that the SMP-DSI would positively affect social participation of the DSI older adults.
Methods
Study design
The study was designed as a cluster randomised, single-blind controlled trial, comparing the effectiveness of the SMP-DSI programme to usual care. Thirty LTC homes (clusters) spread across the Netherlands participated in the cRCT. DSI older adults living in the LTC homes were linked to a familiar licensed practical nurse. Nurses in the intervention group were trained to support the self-management of the DSI older adults using the SMP-DSI. To avoid possible contamination arising from control group nurses coming into contact with DSI older adults or nurses of the intervention group, randomisation took place at the level of LTC homes. The primary outcome was social participation, and the Activity Card Sort (ACS)27 was chosen as the most important primary outcome to measure this, so the study was powered for this end point. The remaining end points were considered as supportive outcomes. Further details of the methods of the cRCT are described in the study protocol.28 The study was approved by the Dutch Committee on Research involving Human Subjects region Arnhem-Nijmegen, ABR 26192.091.08. Written informed consent was obtained from all older participants. Nurses invited for participation in the cRCT gave verbal consent.
Recruitment
Participating DSI older adults and nurses were recruited among LTC homes spread across the Netherlands. The older adults were assessed for eligibility prior to randomisation of the homes. Inclusion criteria for the DSI older adults were (1) aged 55 years or over, (2) a hearing impairment measured by pure tone audiometry of ≥40 dB (best ear, mean of frequencies 1000, 2000 and 4000 Hz), and a visual impairment with a best-corrected visual acuity ≤0.3 diopter or, if additional visual problems were present, a visual acuity of ≤0.5 diopter, following the criterion standards for hearing and visual impairment29 30 and (3) written informed consent. Exclusion criteria were (1) prelingual deafness, (2) a DSI acquired before the age of 50 years and (3) inability to complete interviews due to cognitive problems. The online supplementary file 1 gives details of the assessment procedure used to detect eligible older adults among the LTC residents.
Supplementary file 1
Inclusion criteria for nurses were (1) at least twice-weekly direct daily care contact with the participating older adult, and (2) qualified as a licensed practical nurse, that is, a 3-year basic nursing vocational training at secondary level. Nurses were invited for participation by their manager, and gave verbal consent. Each nurse was linked with one or two DSI older participants.
Randomisation and masking
Due to planning issues in the LTC homes and the availability of the trainers, the LTC homes were recruited in consecutive blocks. An independent statistician randomised the LTC homes in blocks using a computer-generated random sequence. The aim was to randomise a minimum of 14 and maximum of 20 homes, expecting to include a total of 132 DSI older adults. The control group received care as usual, the intervention group received the SMP-DSI and the nurses linked to the DSI older adults of the intervention group were trained to implement the SMP-DSI. The study was single blinded. Research assistants involved in the preinterview and follow-up interview were blinded to the allocation of the LTC homes. Older adults, nurses and trainers of the intervention group were aware of the allocation, but were blinded to the result of any previous assessments.
Self-management programme and SMP-DSI training programme
The SMP-DSI was developed as a five-step interview including problem identification (step 1), collecting alternatives (step 2), choice and planning (step 3), execution (step 4) and reflection (step 5). Table 1 reflects the key features of the SMP-DSI, including the nurses’ supportive questions.
Key questions of the Self-Management Programme for Dual Sensory Impaired Older Adults and nurses’ supportive questions
The SMP-DSI was based on D’Zurilla and Goldfried’s problem-solving therapy,21 Lorig and Holman’s core self-management skills,22 and Bakker-de Pree’s constructional behaviour therapy.31 The aim was to empower the older adults to develop feasible solutions and to cope with possible social or physical constraints, using familiar strategies and by reflecting on recent successful behaviour. In conformance with the problem-solving approach, the older adults were not asked to restrict problems to DSI-related problems only, nor to justify choices, even if it was a choice not to take further action.
The licensed practical nurses were asked to introduce the SMP-DSI to the DSI older adults in daily encounters when they observed that the older adult had a problem or request. However, at the start of the training programme, nurses stated that they were unaware of possible problems or needs among the DSI older adults. Therefore, nurses were encouraged to use open questions, for example, by asking the DSI older adult if there were things he/she would like to change.
As the performance of the SMP-DSI required the licensed practical nurses to adopt new skills, a training programme was developed and implemented based on Grol and Wensing’s implementation model for psychosocial interventions.32 Nurses received a total 16.5 hours training spread over nine sessions in 5 months, consisting of three successive rounds of (1) a 3-hour group training session, (2) a 1-hour individual coaching session on the job and (3) a 1.5-hour group supervision session. The training sessions were offered in parallel to the intervention period, allowing the nurses to improve and deepen their insights and skills in using the SMP-DSI. Nurses were asked to practice using the SMP-DSI at least once during the 2-week to 3-week interval between each training session. As the performance of the SMP-DSI was dependent on the initiative of the nurses in daily care situations, they were asked to keep track of their SMP-DSI interviews by using two separate semi-structured diaries. In the intervention diary, nurses literally quoted the older adults’ verbal responses, either immediately or during the SMP-DSI interview; in the coaching diary, nurses reflected on and evaluated their own behaviour. Both diaries were used as coaching tools and handed over to the trainer at the end of each individual coaching session. Moreover, they gave the research team an overview of the performance of the intervention. Online supplementary file 2 provides an overview of the SMP-DSI training programme and trainers’ roles.
Supplementary file 2
In total, 3 hours of the group training sessions were dedicated to offering nurses insights into the problems and needs associated with DSI and deafblindness. Based on both the literature and practical experience, the problems and solutions towards communication, information access, daily activities and mobility were described and discussed. These discussions included the need for technical and rehabilitation resources, and psychosocial supportive measures for DSI older adults, such as one-to-one conversations, elimination of background noise and the use of shapes, contrast and lighting.6
Nurses who met the training attendance criterion (a minimum of seven of the nine training sessions) and who completed the diaries criterion (a minimum of seven intervention diaries per nurse per older adult), received a certificate.
Data collection
The primary outcome measure for older adults was social participation, measured by the ACS.27 The ACS identifies a person’s activity pattern in social participation and its four domains: instrumental activities of daily living (IADL), social-cultural activities, high-physical-demand leisure activities and low-physical-demand leisure activities. The ACS has been adapted for use in visually impaired older adults and has been validated in a number of samples of older adults.33–35 The weighted scores of each of the four domains range from 0% to 100%, higher scores are indicative of higher levels of participation. As the ACS did not explicitly cover social participation problems as a result of hearing impairment, we chose the Hearing Handicap Questionnaire (HHQ) as an addition to the primary outcome.36 The HHQ is a 12-item questionnaire that identifies participation restrictions related to hearing impairment. Total scores range from 12 to 60, with lower scores being indicative of higher levels of participation. Secondary outcomes were autonomy, mood, perceived control and quality of life, measured using the Patient Autonomy Questionnaire (PAQ),37 the Centre for Epidemiology Studies Depression Scale (CES-D),38 the Pearlin Mastery Scale (PMS)39 and the Rand Short-Form 36 Health Survey, respectively.40 At nurse level, the outcome measure was job satisfaction, measured by the Maastricht Job Satisfaction Scale for Healthcare (MJSSH).41 Research assistants collected the data for baseline in month 1 and for post-test in month 10. The intervention period started in month 3 and ended in month 7, leaving 3 months between the end of the intervention period and the post-test. Initially, post-test was planned within the month after the end of the intervention period (month 8);28 however, the nurses needed more time to get familiar with the intervention. As a longer implementation period might add to the success of psychosocial interventions,42 we moved the post-test to month 10 in the intervention and control group.
For process analysis, we used the framework by Leontjevas et al.43 We evaluated sampling quality (recruitment and reach) and intervention quality (treatment delivery, adherence, relevance and feasibility). Sampling quality was evaluated using qualitative data collected from the research data base. Intervention quality was evaluated using quantitative and qualitative collected from the research data base and from the intervention and coaching diaries. Treatment delivery was evaluated using quantitative data retrieved from the intervention diaries: (1) the number of diaries reflecting the number of sessions between the DSI older adults and their nurse, (2) the number of problems addressed, (3) the number of problems discussed by each pair and (4) the extent to which these problems were addressed using the SMP-DSI steps. We evaluated adherence using quantitative data retrieved from the research data base: (1) the extent to which the nurses met the attendance criteria and (2) the extent to which the nurses met the diaries criteria. Relevance and feasibility as perceived by the nurses were evaluated using qualitative and qualitative data from the coaching diaries. Our findings on relevance and feasibility have been reported in a separate qualitative study.44 In addition, we analysed the collection of problems addressed with the SMP-DSI in this cRCT; these were reported in a second separate qualitative study.45
The intervention and coaching diaries were handed over by the nurses to the trainer at the end of each individual training session; the trainer then posted the diaries to the research team.
Data analysis
Older adults’ outcomes were analysed using a linear mixed model accounting for clustering of older adults within LTC homes (random effect for home) and repeated measurements (random effect for an older adult within a home). As a consequence, the estimated effect was corrected for baseline value of the outcome of interest. As more than half of the nurses only had one older adult, the data did not provide sufficient information to estimate variation of older adults within nurse, that is, models including nurse as level, so no estimates could be made for ‘within older adult, within nurse, within home’ due to computational non-convergence. Therefore, the intermediate level of nurse was omitted from the analyses. Nurses’ outcomes were similarly analysed (random effect for home and for nurses within home). The ACS was chosen as the most important primary outcome end point, and the study was powered for this end point. The HHQ and the secondary end points were considered as supportive outcomes. As previous research has shown that the effectiveness of a self-management intervention among visually impaired older adults was significantly greater for subjects suffering from depressive feelings than for subjects without depressive feelings,46 effect-modification was planned for the outcome mood, measured using the CES-D scale.
We used descriptive statistics to evaluate sampling and intervention quality.
Results
Recruitment and reach
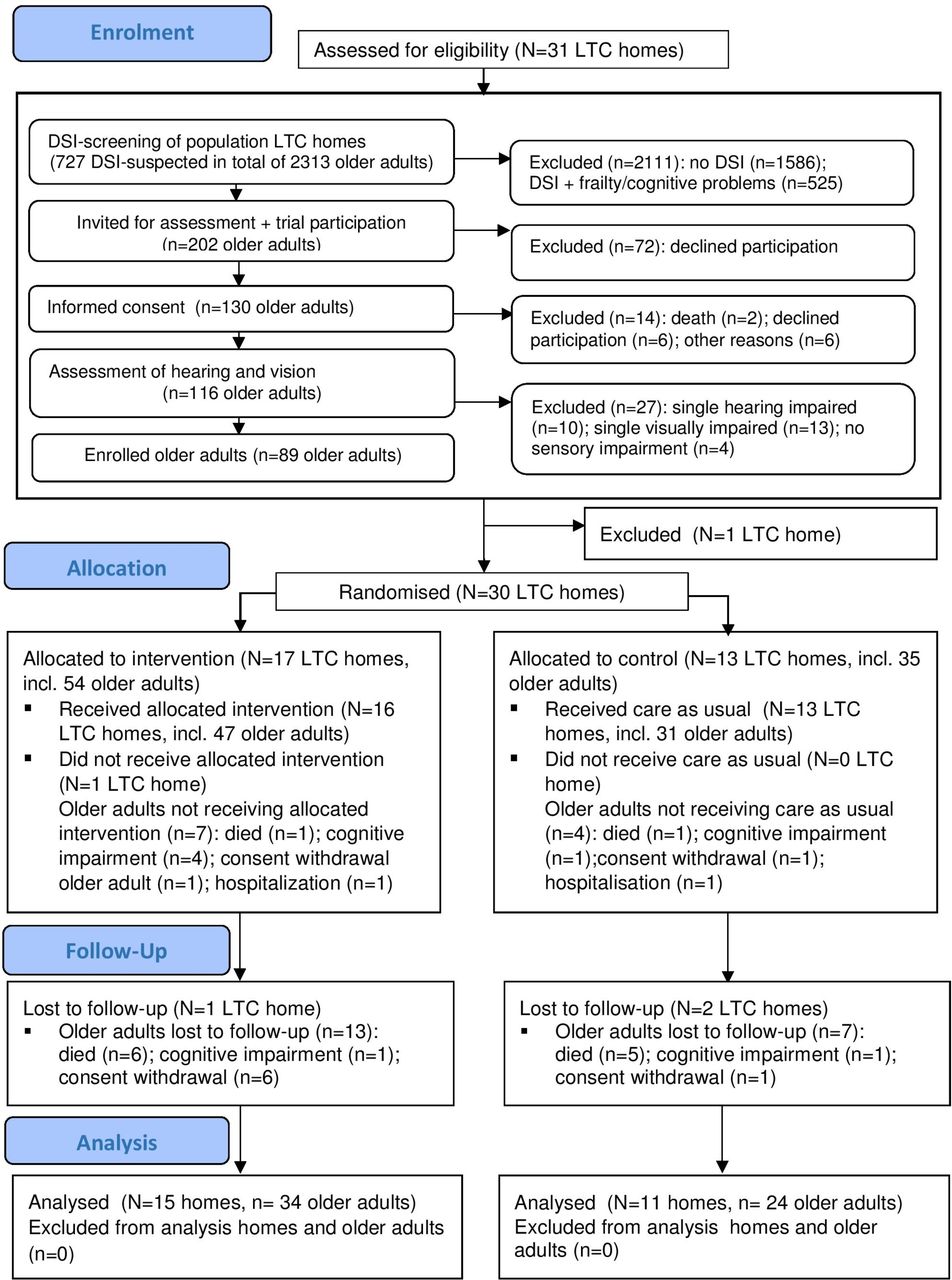
Between April 2011 and June 2014, 67 LTC homes spread across all regions of the Netherlands were approached for participation. Consent for participation was received from 31 LTC homes (46%), however in one home, no eligible older adults were found. The 30 remaining homes (clusters) were successively randomised, spread over seven blocks (n1=8 LTC homes; n2=7; n3=2; n4=5; n5=4; n6=2; n7=2); 17 to the intervention arm (54 older adults) and 13 to the control arm (35 older adults). The average size of the homes was 78 beds (minimum 32, maximum 124). Figure 1 presents the Consolidated Standards of Reporting Trials flow diagram, including the enrolment of eligible older adults prior to the randomisation of the LTC homes.

{kind=link}
Consort flow diagram enrolment. DSI, dual sensory impairment; LTC, long-term care; N, number of LTC homes; n, number of older adults.
At the 31 selected homes, 2313 residents were screened using the Severe Dual Sensory Loss screening tool.47 Figure 1 shows that 727 (31%) were screened as possibly having DSI, of whom 525 (72%) were excluded either due to severe cognitive problems (n=352; 67%), or because LTC professionals judged that they were too frail to be interviewed (n=173; 33%). The average number of older participants per home was three (minimum 1, maximum 9). Seven of the eligible 54 older adults dropped out after randomisation but before the start of the intervention, as did 4 of the 35 older adults of the control group. This resulted in 16 homes where the intervention started, including 47 older adults linked with 34 nurses, and 13 homes in the control group, including 31 older adults linked with 22 nurses.
Treatment delivery and adherence
A total of 258 intervention diaries were collected, addressing 122 different problems, showing that the overall extent of programme performance was fair. Over the 5-month intervention period, each pair of nurse and older adult discussed two to three problems and spent two to four sessions addressing a single problem. Of the 122 problems, 57 (46.7%) were fully addressed using all five steps of the SMP-DSI, and 65 (53.2%) were interrupted after step 2 or 3.
Twenty-seven (80%) of the 34 nurses who started the training programme met the criteria on attendance and the diaries assignments, and received a certificate. Seven nurses (20%) did not receive a certificate as they were unable to meet the criteria due to staffing problems (five nurses), death (one nurse) or unknown reason (one nurse). In the case of those nurses who did not meet the criteria, two colleague-nurses who were already involved in the intervention took over, two other nurses were lost for follow-up and the other three nurses remained involved in the intervention.
Baseline comparison
Table 2 presents the baseline characteristics of the intervention and control group. Control for potential confounders showed no relevant change in the intervention estimate, that is, the differences in baseline characteristics did not confound the intervention effect.
Baseline characteristics of older adults and nurses in intervention group and control group (n=89 older adults, 56 nurses)
Effect outcomes
Table 3 presents the effect outcome results, showing no statistical significant differences in social participation between the intervention and control group as measured by ACS-total (0.3; 95% CI −3.4 to 3.9) and by HHQ (−1.3; 95% CI −5.7 to 3.0). The ACS-domain IADL had an effect in favour of the intervention group. Measured from baseline to follow-up, the IADL in the control group had an estimated decline of 6.7 points (P≤0.001; 95% CI −9.9 to −3.5), while the intervention group showed a 4.3-point lower decline than the control group (P=0.04; 95% CI 0.12 to 8.5).
Means (SD) and estimates from the repeated measurements model for primary and secondary outcomes (n=89)
Secondary outcome measurement on autonomy (PAQ), perceived control (PMS) and mood (CES-D) showed no significant differences between the intervention and control groups. Analysis of effect-modification showed no significant differences between the DSI impaired older adults suffering from depressive feelings and the older adults without depressive feelings. The nurses’ outcomes showed no significant changes over time regarding job satisfaction (MJSSH).
Discussion
This study evaluated the effectiveness of a Self-Management Programme for Dual Sensory Impairment older adults (SMP-DSI) in long-term care (LTC). We found no positive effect in social participation as measured by the ACS-total, nor in three domains of the ACS; social-cultural, high-physical-demand and low-physical-demand leisure activities. However, we found a beneficial effect on the ACS-domain IADL as the decline significantly slowed down. In contrast to previous research among visually impaired older adults, no differences in effectiveness were found between the older adults suffering from depressive feelings and the older adults without depressive feelings.
Evaluation of the sampling and intervention quality showed that the trial was carried out adequately. The consent rate of LTC homes (46%) is acceptable, and in line with other studies.48 The consent rate of DSI older adults (64%) is satisfactory and is comparable with the 62% obtained by Leontjevas et al,49 but should be interpreted with caution, as recruitment and reach figures have seldom been fully described in psychosocial intervention studies on LTC residents. Overall, treatment delivery was fair. When compared with the findings of the parallel study analysing the problems addressed with the SMP-DSI,45 we observed differences in treatment delivery: problems in controlling personal space were addressed to a greater extent than were the problems requiring behavioural involvement of others. Of the problems in controlling personal space, 27 of the 44 (61.3%) were fully addressed using all five SMP-DSI steps. Of the problems requiring behavioural involvement with others, only 30 of the 78 problems (38.4%) were fully addressed.
A comparable contrast in the effectiveness of addressing IADL versus social leisure and cultural activities has been reported in earlier studies of older adults with disabilities.50 The large and positive effect on the ACS IADL domain (>60% reduction of the decline) and the higher rate of treatment delivery for problems in controlling in personal space (61.3%) suggest that the older adults were able to self-manage concrete daily living problems such as budgeting or medication management with the support of their nurse. Two factors may have contributed to this positive result. First, the self-management intervention was offered in the everyday environment of the older adult, the problems were identified by the older adults themselves, and solutions were explored within that same everyday environment. This is in line with research findings showing that ‘real-world’ interventions stimulate cognitive, social and physical activity among older adults.51 Second, the problems were concrete and assignable, which may have endorsed the feeling of mutual partnership between nurse and older adult to engage in and explore possible practical and concrete solutions together. This aligns with research findings showing that the creation of trust and partnership between the healthcare worker and patient is an important factor in the success of self-management interventions.52
However, the interventions had no effect on the ACS domains leisure and social-cultural activities. This lack of effectiveness on these domains and the low rate of treatment delivery of the participation problems requiring behavioural involvement of other persons (38.4%), seem to align with research findings that the social network of older adults steadily decreases due to age-related life events.53 However, by identifying their participation problems and searching for alternative solutions (steps 1 and 2 of the SMP-DSI, respectively), the DSI older adults showed that they were eager to alter those problems. Treatment delivery showed that they tended to ‘give up’ when choices and plans had to be made requiring interactive routes. A factor that might have provoked this reluctance is that they felt no partnership with the LTC professional caretakers who were targeted. Mudge et al 54 showed that healthcare professionals felt tense and unfamiliar when forming a partnership with patients, and dedicating time to practice reciprocity in communication style. At the start of the intervention period, we observed a similar lack of partnership between the DSI older adults and their nurse.44 The feelings of partnership only developed after nurses and older adults started a dialogue based on the SMP-DSI steps.
This study faced several challenges regarding recruitment due to the rapidly increasing incidence of advanced stages of cognitive problems and frailty among DSI older adults in Dutch LTC homes. The study suffered from a large exclusion rate, as 72% of older adults were unable to participate due to cognitive problems or frailty. This had been partially anticipated, as earlier studies noted an increased risk of comorbidities in DSI older adults.55 56 However, the increased prevalence of DSI in LTC and the large exclusion rate may be partly explained by the rapidly changing LTC home population resulting from recent policy changes introduced by the Dutch government. After the start of our trial, the admission to LTC homes became restricted to only those older adults who needed intensive care or 24 hours surveillance due to their advanced stage of cognitive impairment. As recruitment per cluster was lower than planned, we recruited more clusters than planned. However, the statistical power of the study may therefore have been smaller than originally planned. Another limitation was that we did not calculate the cost-effectiveness of the intervention. Future research should review costs, based on resource and time calculations, involved in the evaluation.
A possible risk for bias was that nurses did not voluntarily present for participation. After inclusion of the older adults, the manager invited nurses who were familiar with the participating older person to join the trial. This was mainly due to practical reasons, although the degree of health professionals’ voluntary participation has been shown to contribute to the success of an intervention.57 Since the number of eligible nurses per team was limited, the risk that the managers’ invitation would create a bias is limited. However, nurses’ changing perceptions in the course of the intervention, starting from fairly negative to positive perceptions (as reported in our parallel study), might have negatively affected the results.44
As this is one of the first intervention studies on DSI among care-dependent older adults, lessons can be learnt for practice and research for frail older adults in LTC as well as for community living DSI older adults. First, the generalisability of the SMP-DSI intervention itself to other care organisations or healthcare systems has been challenged. The performance of the SMP-DSI requires qualitative conditions, such as partnership and connectedness, which are not obviously present in usual care. The SMP-DSI is an intervention that fits in the (inter)nationally changing focus in healthcare from physical health to social health, from taking care of the care recipient and aiming at physical well-being, to care offering psychosocial support aiming at social well-being. However, as such psychosocial interventions are still scarce, a great deal of its implementability, strengths and barriers, remain unexplored. The findings of nurses’ changing perceptions in our study illustrated the cultural clash that occurs when both aims meet each other. Regarding generalisability of the SMP-DSI, the strength of this study is in the identification of those psychosocial intervention elements that were shown to be working elements. This demonstrated that the combination of longitudinal, ongoing nurse–older adult interactions with self-reflective coaching was an important positive working element to take these cultural hurdles.
Second, the SMP-DSI requires mental capacities in executive functioning that probably makes the intervention difficult to implement among older adults suffering from moderate-to-severe cognitive impairment. Yet the increasing DSI population with cognitive impairment in LTC reaffirms the need to develop psychosocial support for these care-dependent older adults. Findings from this study such as the need of client-aligning attitudes and skills among nurses, and the problems identified by the DSI older adults with no or only mild cognitive problems, may offer researchers and programme developers opportunities to develop observational and behavioural tools aimed at providing support to cognitive impaired DSI older adults.
Finally, the SMP-DSI was developed as an empowering instrument for care-dependent DSI older adults, whether they were community dwellers or LTC residents. As home care organisations were not able to meet our inclusion criterion that familiar nurses could meet the older adults at least twice a week, the SMP-DSI could not be tested among community dwelling DSI older adults. However, taking the findings on the relevance and feasibility of the SMP-DSI in LTC into account, we recommend implementing and testing the SMP-DSI in home dwelling environments in a lower once-a-week meeting frequency of the familiar nurse with the older adult, which would possibly be more implementable and might be feasible in home dwelling environments. Another option is to involve voluntary welfare professionals who visit these DSI older adults at home, and who have been coached in the SMP-DSI method by trained coaches (eg, nurses or other care or welfare professionals). However, this should be investigated in future research.
In summary, this study demonstrates that the nurse-supported SMP-DSI was not successful in addressing problems related to social-cultural and leisure activities in DSI older adults, but it does show beneficial effects in addressing IADL problems. By combining the results of the effect study with the qualitative process findings, we explored barriers and solutions, and show that the participation of DSI older adults can benefit from enhanced dialogues and partnership with their LTC professionals.
References
Footnotes
Contributors LMR-M, SUZ, MJFJV-D, GIJMK and MJLG performed the study concept and design, LMR-M and PGJMH the acquisition of participants and ST and LMR-M the data analysis. All authors were involved in revising the manuscript and read and approved the final version of the manuscript. The corresponding author and all coauthors had full access to the study data and had final responsibility for the decision to submit for publication.
Funding This study was financially supported by the Joannes de Deo Foundation and the Mother Catharina Fund, the Netherlands.
Disclaimer The sponsors had no role in the design, methods, subject recruitment, data collections, analysis or preparation of the report.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study design and protocol has been approved by the Dutch Committee on Research involving Human Subjects region Arnhem-Nijmegen, ABR 26192.091.08. Informed consent was completed by all participants before starting the assessments and interventions.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The dataset and statistical code are available from the Data Archiving and Networking Service (DANS). https://easy.dans.knaw.nl/ui/datasets/id/easy-dataset:65449.