Article Text

Abstract
Objectives While increasing attention is paid to the rising prevalence of chronic diseases in Africa, there is little focus on chronic kidney disease (CKD). This systematic review assesses CKD burden among the general population and high-risk groups on the entire African continent.
Design, setting and participants We searched Medline and PubMed databases for articles published between 1 January 1995 and 7 April 2017 by sensitive search strategies focusing on CKD surveys at the community level and high-risk groups. In total, 7918 references were evaluated, of which 7766 articles were excluded because they did not meet the inclusion criteria. Thus, 152 studies were included in the final analysis.
Outcome measurement The prevalence of CKD in each study group was expressed as a range and pooled prevalence rate of CKD was calculated as a point estimate and 95% CI. No meta-analysis was done. Data were presented for different populations.
Results In the community-level studies, based on available medium-quality and high-quality studies, the prevalence of CKD ranged from 2% to 41% (pooled prevalence: 10.1%; 95% CI 9.8% to 10.5%). The prevalence of CKD in the high-risk groups ranged from 1% to 46% (pooled prevalence: 5.6%; 95% CI 5.4% to 5.8%) in patients with HIV (based on available medium-quality and high-quality studies), 11%–90% (pooled prevalence: 24.7%; 95% CI 23.6% to 25.7%) in patients with diabetes (based on all available studies which are of low quality except four of medium quality) and 13%–51% (pooled prevalence: 34.5%; 95 % CI 34.04% to 36%) in patients with hypertension (based on all available studies which are of low quality except two of medium quality).
Conclusion In Africa, CKD is a public health problem, mainly attributed to high-risk conditions as hypertension and diabetes. The poor data quality restricts the validity of the findings and draws the attention to the importance of designing future robust studies.
- CKD
- Africa
- systematic review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This systematic review assessed the chronic kidney disease (CKD) burden among the general population and high-risk groups on the entire African continent based on studies that covered all of Africa from 1 January 1995 until 7 April 2017.
The quality of the included articles was assessed based on standard criteria dealing with clinical trials, diagnostic studies and observational studies. The articles were assessed based on the population sampling and precision, sampling technique, response rate and exclusion rate.
No meta-analysis was conducted in this review due to the huge discrepancy in the definition used to identify CKD, the methods of creatinine measurement, urine protein assessment and in the quality of the reporting.
There is paucity of information about CKD prevalence in age and gender groups, which affects the accuracy of the pooled prevalence estimated from each group.
The prevalence of CKD reported in this review should be interpreted with caution due to the low quality of the majoirty of studies in Africa, the bias introduced from the heterogeneity between studies, analytical and methodological issues, sample size, and study population selection.
Introduction
Chronic kidney disease (CKD) is an emerging global public health problem.1 The disease is a component of a new epidemic of chronic conditions that replaced malnutrition and infection as leading causes of mortality during the 20th century.2 Age-standardised death rates due to CKD have increased during the last 23 years. CKD has shifted from the 36th cause of death in 1990 to the 19th cause in 2013.3 The worldwide increase in CKD and kidney failure—necessitating renal replacement therapy—and the high rate of cardiovascular mortality and morbidity attributable to CKD are poised to reach epidemic proportions over the next decade. CKD complications represent a considerable burden on global healthcare resources and only a small number of countries have sufficiently robust economies to meet the challenge posed by this disease. Socioeconomic differences in health exist and individuals of lower socioeconomic status (SES) have a higher risk for mortality and morbidity compared with those of higher SES.4 A change in the global approach to CKD from the treatment of end stage renal disease (ESRD) to intensive primary and secondary prevention is therefore considered an absolute public health priority.5
Africa is the second largest continent in the world, with a population of over 1 billion; 961.5 million people live in sub-Saharan Africa and 195 million in Northern Africa.6 Africa now faces the dual challenge of infectious illnesses and chronic diseases. Africa’s chronic disease burden is secondary to various factors, including increased life expectancy, changing lifestyle practices, poverty, urbanisation and globalisation.7 The World Health Assembly advocated the Global Action Plan for the Prevention and Control of Non-Communicable Diseases 2013–2020. One of its targets is to reduce premature mortality from chronic diseases by 25% in 2025. These actions have the potential to make a significant impact on the burden of CKD.8 Unfortunately, CKD problem remains underestimated on the entire continent due to lack of epidemiological information from different African countries. There exists only a single systematic review conducted in sub-Saharan Africa, which concluded that CKD is a prevalent and potentially escalating disease across sub-Saharan Africa, with both communicable and non-communicable risk factors.9 Strategies aimed at managing CKD epidemics in Africa critically depend on a reliable assessment of the burden of the problem and the establishment of affordable early detection programmes. Previous studies reported the prevalence of CKD among the general population or the specific prevalence of this condition in diseases that are recognised as drivers of renal damage (eg, diabetes mellitus). These estimates have varied across studies due to differences in the methods of glomerular filtration rate (GFR) measurement, background risk (general population vs high-risk groups) or demographic characteristics (eg, age, gender).10
With this background in mind, this review aimed to increase the systematic information on the burden of CKD in the general population and high-risk groups of the entire African continent and provide an estimate of the prevalence of CKD in different regions of Africa.
Materials and methods
Data source and search strategy
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.11 A systematic literature search was performed in the PubMed and Ovid Medline databases by two authors (DB and SA) to identify articles reporting epidemiology data on CKD in the adult population in any geographical area of the African continent. This employed focused, highly sensitive search strategies (online supplementary table 1). The search covered the time frame from 1 January 1995 to 7 April 2017. Papers without language and study design restrictions were located and screened. References from relevant studies were screened for supplementary articles.
Study selection and data extraction
Titles and abstracts were screened independently by two authors (SA and GD), who discarded studies that were not relevant to the topic. Case reports, reviews, editorials, letters and studies focusing on African–Americans not living on the African continent, conducted entirely among children, or dealing with acute kidney injury or kidney transplantation were excluded. Two authors (SA and ED) independently assessed the retrieved abstracts and the full texts of these studies to determine eligibility according to the inclusion criteria. Disagreements were resolved through discussion and consensus, or through consultation with a third reviewer (DB), who solved these differences based on study judgements. Furthermore, screening of reference lists of all of the retrieved studies was conducted to check for relevant articles, and a supplementary scan of the reference lists of the systematic reviews was performed to identify any additional studies. Data were extracted from full-text articles and registered using a specifically designed form. These data included study design, geographical area, sample size, the definition of CKD used, prevalence of CKD, age, gender, GFR measurement, type of creatinine assay, proteinuria, the method of outcome assessment, and associated comorbidities such as diabetes mellitus and hypertension. Data extraction was performed by one reviewer (SA) and independently verified by another reviewer (DB).
Data extraction and analysis
Studies were categorised according to the reference population as follows: (1) studies dealing with the general population and (2) studies focusing on particular diseases such as diabetes, hypertension, lupus and HIV, or settings, for example, hospital-based surveys and occupational studies.
Information on the assessment of kidney function was collected, including the equation adopted for GFR estimation (Cockroft-Gault (CG), Modification of Diet in Renal Disease (MDRD), Chronic Kidney Disease-Epidemiology Collaboration (CKD-EPI)), the type of creatinine assay (Jaffe, standardised or unknown), and the type of proteinuria or albuminuria assay used (semiquantitative assessment by urinary strips or quantitative in urine samples or 24-hour collection). When the study included two or three GFR equations, we defined the CKD prevalence based on the CKD-EPI equation whenever this information was provided. Otherwise, we considered the MDRD equation and lastly the CG equation. In the case of ethnicity correction,12–14 we included the equation that corrected for ethnicity. Information on the definition of CKD used in each study was also included (either the internationally accepted definition as Kidney Disease Outcome Quality Initiative (KDOQI), or other ways of defining CKD).
Quality assessment
Two independent authors (SA and DB) appraised each article independently and assessed its quality based on standard criteria described into details in previous methodology reviews dealing with clinical trials,15 diagnostic studies16 and observational studies.17 The articles were assessed based on the subject sampling and precision, sampling technique, response rate, method of assessment of kidney function and exclusion rate.
Statistical analyses
The principal demographic and clinical data for each study were summarised as the mean and SD or as absolute number and percentage, as appropriate. The age range in each study was also recorded. The range of the CKD prevalence for each study group was reported. The pooled prevalence rate of CKD was expressed as a point estimate and 95% CI. The prevalence from each study was weighed by the sample size, then the pooled prevalence was categorised by the African region. The inter-rater agreement for inclusion and quality assessment was determined using Cohen’s kappa (κ) coefficient.18 The percentage of the different causes of CKD was weighed by the sample size of each study done among patients with CKD. Then we simply summed the number of patients for each aetiological factor and divided it by the total sample size from the whole included studies. No meta-analysis was conducted in this study. Data were appropriately presented for different populations (general population and patients with CKD). Patients’ data were stratified by the type of underlying condition, that is, hypertension, diabetes mellitus, HIV or systemic lupus erythematosus. All calculations were conducted using SPSS for Windows V.21.
Results
Search results
The flow diagram of the selection process is depicted in figure 1. In total, 7897 potentially relevant references were initially retrieved. Twenty-one additional citations were found through a personal search. By screening titles and abstracts, a total of 7534 citations were excluded because of search overlap, dealing with the wrong population (African–American, acute kidney injury (AKI), cancer or post-transplant patients) or not providing actual data on CKD. Review articles, case reports, editorials or letters were also excluded. Among the 384 studies selected for full-text examination, 232 were excluded because they dealt with a population different from that specifically targeted in this systematic review, such as paediatric populations (122 studies), transplant patients (n=44) or others (n=46) (eg, Africans living in non-African countries), or because only narrative data were provided (n=20). A total of 152 articles were therefore reviewed in detail and included in the analysis. The main characteristics of these studies are summarised in table 1. The inter-rater agreement for inclusion wa-s κ=0.90 and for the quality assessment was κ=0.85.

Flow diagram of the study selection.
Characteristics of the study population included in the analysis
Study characteristics
Among the 152 studies reviewed, 29 were general population studies (table 2). One hundred and twenty-three studies focused on selected groups, of which 42 included patients with HIV (table 3), 18 studied patients with diabetes (table 4), 9 included hypertensive subjects (table 5) and 12 were conducted in other populations (table 6), including one study in patients with lupus,19 one study in patients with rheumatoid arthritis,20 one study among patients with sickle cell anaemia,21 two in specific occupational settings (silica exposure22 and exposure to the nephrotoxic hair-dye, paraphenylenediamine23) and seven studies in family practice24–26 or hospital-based27–30 surveys. Forty-two studies were conducted among patients with CKD (online supplementary table 2).31–72
Studies on CKD among the general population
Studies on CKD among patients with HIV
Studies on CKD among patients with diabetes
Studies on CKD among patients with hypertension
Studies on CKD among other populations
The studies that were included covered all regions of Africa. The highest number of the studies came from the Western macro-area (n=54), followed by the Eastern macro-area (n=32) and Southern macro-area (n=25). Twenty studies were retrieved from Northern Africa, and eight studies from each of the Central macro-area and the Central-Western macro-area. Three studies were conducted in both the Eastern and Southern regions and two studies in the sub-Saharan region.
Assessment of kidney function impairment
Urinary markers for kidney disease were assessed in 78 (71%) among 110 studies conducted in the general population, high-risk groups, occupational or hospital-based studies. Proteinuria was assessed by a semiquantitative method (urinary strips) in 28 studies.21 24 26 29 73–96 Twenty studies used dipstick with confirmation by quantitative methods, nine of which used dipsticks to identify proteinuria/albuminuria with confirmation by 24-hour proteinuria,25 97–104 whereas 11 studies used dipstick with confirmation by the protein-to-creatinine ratio or albumin-to-creatinine ratio.105–115 Quantitative methods for the assessment of proteinuria/albuminuria (24-hour proteinuria or albuminuria, Protein to Creatine Ratio (PCR), immunoassay or Albumin to Creatinine Ratio (ACR) were applied in 29 studies.19 27 28 30 116–140 In one study, the method of proteinuria assessment was not mentioned.141
Serum creatinine was measured in 95 studies (86%). The Jaffe assay was used in 30 studies,29 30 76 80 82 83 86 90 95 97 102 105 111 113 124 126 130 131 136 142–152 whereas the isotope dilution mass spectrometry (IDMS)-calibrated method was used in 15 studies.12 14 21 26 115 117 132–134 141 153–157 In nine studies, both the Jaffe assay and the calibrated serum creatinine were used.13 20 25 91 98 99 106 112 158 The remaining 41 studies provided no information on the method of creatinine measurement.19 24 27 28 78 79 81 84 85 87–89 93 94 96 100 101 104 109 114 116 118–122 125 127 135 137–139 159–167 With respect to the formula used for estimating GFR, the MDRD equation was used in 30 studies24–26 28 29 94–97 105 106 111 113 116 117 121 122 126 130 133 134 136 141 146 149 153 154 158 159 164 and the CG equation was used in 18.19 76 81 86–88 93 100 102 114 119 124 138 143 145 150 162 167 The other 14 studies used both the CG and the MDRD equations,78–80 83–85 98 99 101 144 147 152 161 163 whereas 15 studies estimated GFR by the CG, MDRD and the CKD-EPI methods.12–14 20 82 90 91 109 112 115 139 142 155 156 160 Six studies used MDRD and CKD-EPI131 132 137 148 151 157 and two studies used CKD-EPI.21 166 In other two studies the formula was not mentioned.30 135
Definition of CKD
Thirty-one studies defined the presence of CKD as an estimated glomerular filtration rate (eGFR) below 60 mL/min/1.73 m2,12 14 20 80 93–96 111 117 119 139 146 148–159 161–164 166 167 with chronicity confirmed by repeated testing in four other studies.142–145 Moreover, 28 studies reported CKD prevalence based on eGFR below 60 mL/min/1.73 m2 and/or the presence of proteinuria or albuminuria.21 24 26 76 78 82–84 86 91 99 100 105 106 109 112–114 121 130–137 141 Proteinuria/albuminuria was used alone to identify CKD in 14 studies.73–75 77 87 92 107 108 110 123 128 129 138 140 KDOQI staging168 of CKD was used in 13 studies.13 25 29 79 85 90 97 98 115 116 122 124 126 The serum creatinine level (either doubling, or an increase above a certain threshold) was considered to be a marker of the presence of CKD in four studies.89 104 120 165 In 16 studies, the definition of CKD was either not mentioned or was defined in various ways, including personal history, creatinine clearance (CrCl) ≤50 mL/min, clinical manifestations, the presence of albuminuria, elevated serum creatinine and the average of two measurements of eGFR <90 mL/min/1.73 m2.19 27 28 30 81 88 101–103 118 125 127 147 160 169 170
Paper quality
Paper quality was high in 16 studies.13 25 75 90 91 97 98 105 106 112 116 132–134 148 155 Thirty-five studies were of medium quality.12 14 26 29 73 74 77–79 81 82 96 110 111 115 117 128 130 131 137 141 143–145 150–152 154 157 159–161 163 166 167 The rest of the studies were of low quality.
Prevalence of CKD
The included medium-quality/high-quality studies in the general population in Africa provided estimates of CKD prevalence by disparate criteria (table 2). The prevalence of CKD ranged from 2% to 41% (pooled prevalence: 10.1%; 95% CI 9.8% to 10.5%). The prevalence was reported to range from 2% to 41% (pooled estimate: 16.5%) in the West/Central-West, followed by the Central region where the prevalence ranged from 12% to 17% (pooled estimate: 16%), in the Southern where the CKD prevalence range was 6%–29% (pooled estimate: 12.2%), in Eastern where the prevalence ranged from 7% to 15% (pooled estimate: 11.0%), and in the North where the prevalence ranged from 3% to 13% (pooled estimate: 4%) (figure 2). In sub-Saharan Africa, the prevalence ranged from 2% to 14% (pooled prevalence: 14.02%; 95% CI 13.5% to 14.5%). In studies defining CKD as eGFR <60 mL/min, the prevalence of CKD ranged from 7% to 29% (pooled estimate: 13.2%), while in those who adopted the combined criterion GFR <60 mL/min/1.73 m2 and/or the presence of proteinuria or albuminuria, the prevalence ranged from 3% to 22% (pooled estimate: 5.6%). When defined according to KDOQI, the prevalence ranged from 2% to 28% (pooled estimate: 10.8%). Finally, in studies reporting on proteinuria/albuminuria only, the prevalence ranged from 3% to 41% (pooled estimate: 18.9%). The CKD prevalence for each age or gender group was not reported in the majority of the studies. In online supplementary figure 1 we show graphically the relationship between gender and age and CKD prevalence in the medium-high-quality studies of this systematic review.

Prevalence of chronic kidney disease among the entire general population. Estimates from this figure should be presented with caution as it is bound to be imprecise and inaccurate due to its tentative way of estimation.
Among patients with HIV (table 3), the prevalence of CKD in the 18 medium-quality studies ranged from 1% to 46% (pooled prevalence: 5.6%; 95% CI 5.4% to 5.8%). The prevalence of CKD in the West/Central West macro-areas, which ranged from 9% to 39% (pooled estimate: 11.6%), and the East macro-areas, where the prevalence ranged from 1% to 46% (pooled estimate: 11.2%), had seemingly similar figures, which were higher than in the South (3.5%) macro-areas. Based on the treatment status, the prevalence of renal dysfunction ranged from 1% to 47% (pooled prevalence: 9.9%; 95 % CI 9.4% to 10.4%) among patients with HIV not receiving treatment, while it ranged from 7% to 33% (pooled prevalence: 5.2%; 95 % CI 5.0% to 5.4%) among patients with HIV on antiretroviral therapy. The prevalence was reported to be 5.7% (range: 3.1%–7.2%) among the three studies done in both the East and South macro-areas and 2.5% from the study done in the sub-Saharan area. According to the definition, the prevalence of CKD ranged from 1% to 18% (pooled estimate: 4.7%) in studies that defined CKD as eGFR <60 mL/min. In studies that defined CKD as eGFR <60 mL/min/1.73 m2 and/or the presence of proteinuria or albuminuria, the CKD prevalence ranged from 9% to 21% (pooled estimate: 5.6%). There are other four studies that defined CKD based on either the presence of proteinuria, KDOQI, CrCl <50 mL/min, or albuminuria and serum creatinine. In these four studies, the prevalence of CKD ranged from 3% to 46% (pooled estimate: 12.6%). The CKD prevalence for each age or gender group was not reported in the majority of the studies. In online supplementary figure 1 we show graphically the relationship between gender and age and CKD prevalence among patients with HIV in the medium-high-quality studies.
Among patients with diabetes (table 4, all studies are of low quality except for four with medium quality), the prevalence of CKD ranged from 11% to 90% (pooled prevalence: 24.7%; 95% CI 23.6% to 25.7%). The highest prevalence was in the Eastern, which ranged from 18% to 84% (pooled estimate: 46.9%), followed by the Central, where the CKD prevalence ranged from 30% to 66% (pooled estimate: 40.8%). In the West/Central-West, CKD prevalence ranged from 18% to 90% (pooled estimate: 27.7%), while in the South the CKD prevalence ranged from 18% to 66% (pooled estimate: 23.0%), and in the North CKD prevalence ranged from 11% to 20% (pooled estimate: 18.9%). One study done in sub-Saharan reported that the prevalence was 13%. Among patients with diabetes, CKD prevalence ranged from 11% to 83% (pooled estimate: 51.8%) when CKD was defined as eGFR <60 mL/min/1.73 m2 and/or the presence of proteinuria or albuminuria. When CKD was defined based on proteinuria/albuminuria, CKD prevalence ranged from 26% to 51% (pooled estimate: 36.3%). In patients with diabetes who had CKD based on eGFR <60 mL/min/1.73 m2, the prevalence ranged from 13% to 30% (pooled estimate: 16.6%). When KDOQI was used to define CKD, the prevalence of CKD ranged from 19% to 66% (pooled estimate: 34.2%). The CKD prevalence for each age or gender group was not reported in the majority of the studies. In online supplementary figure 1 we show graphically the relationship between gender and age and CKD prevalence among patients with diabetes in the included studies.
The prevalence of CKD among patients with hypertension (table 5, 9 studies; all of low quality except for two with medium quality) ranged from 13% to 51% (pooled prevalence: 34.5%; 95% CI 34.04% to 36%). The highest prevalence was reported from one study in the East macro-area (39.5%), followed by the West/Central-West, where the prevalence ranged from 13% to 51% (pooled estimate: 37.7%). In South Africa, the CKD prevalence reported from one study was 25.4%. No data were found for other African macro-areas. In studies that defined CKD as eGFR <60 mL/min/1.73 m2, the prevalence of CKD ranged from 38.5% to 40% (pooled estimate: 38.9%). When serum creatinine was used to define CKD, the prevalence ranged from 30% to 51% (pooled estimate: 40.3%). When CKD was defined according to albuminuria/proteinuria, the prevalence of CKD ranged from 15% to 25% (pooled estimate: 23.6%). In one study, CKD was defined according to KDOQI criteria and it was prevalent among 47% of patients with hypertension. The CKD prevalence for each age or gender group was not reported in the majority of the studies. In online supplementary figure 1 we show graphically the relationship between gender and age and CKD prevalence among patients with diabetes in the included studies.
Among other patient populations (studies reported in table 6), almost three-quarters of patients with lupus had CKD (prevalence=72.0%) based on low-quality study.19 Hospital-based surveys revealed that (the calculation was based on the total prevalence reported from all studies including three of high-medium quality and four of low quality in the same table) more than one-third of patients attending either primary care centres or tertiary hospitals had CKD (range: 11%–57%, pooled prevalence: 36%, 95% CI 34.4% to 37.7%). In hospital-based studies, when CKD was defined as eGFR <60 mL/min/1.73 m2 and/or the presence of proteinuria or albuminuria, the prevalence ranged from 10% to 14% (pooled estimate: 12.4%), while the prevalence ranged from 49% to 57% (pooled estimate: 45.1%) when CKD was defined according KDOQI. CKD was prevalent among almost 39% of patients with rheumatoid arthritis20 or sickle cell.21 The study (low quality) conducted among hairdressers exposed to paraphenylenediamine104 reported that 26.4% of these subjects had renal impairment. Of note, 100% of silica-exposed workers experienced proteinuria (reported from low-quality study).129
Causes of CKD
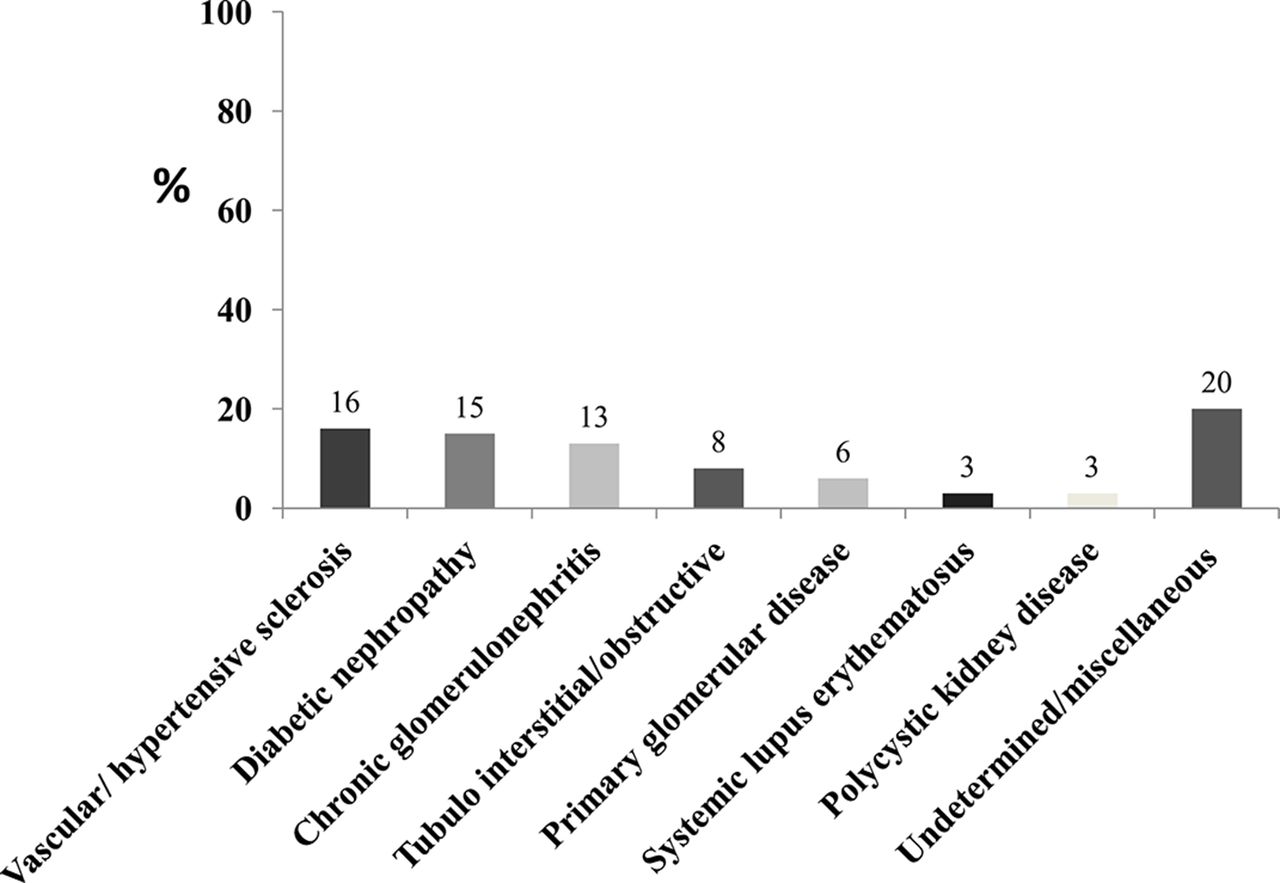
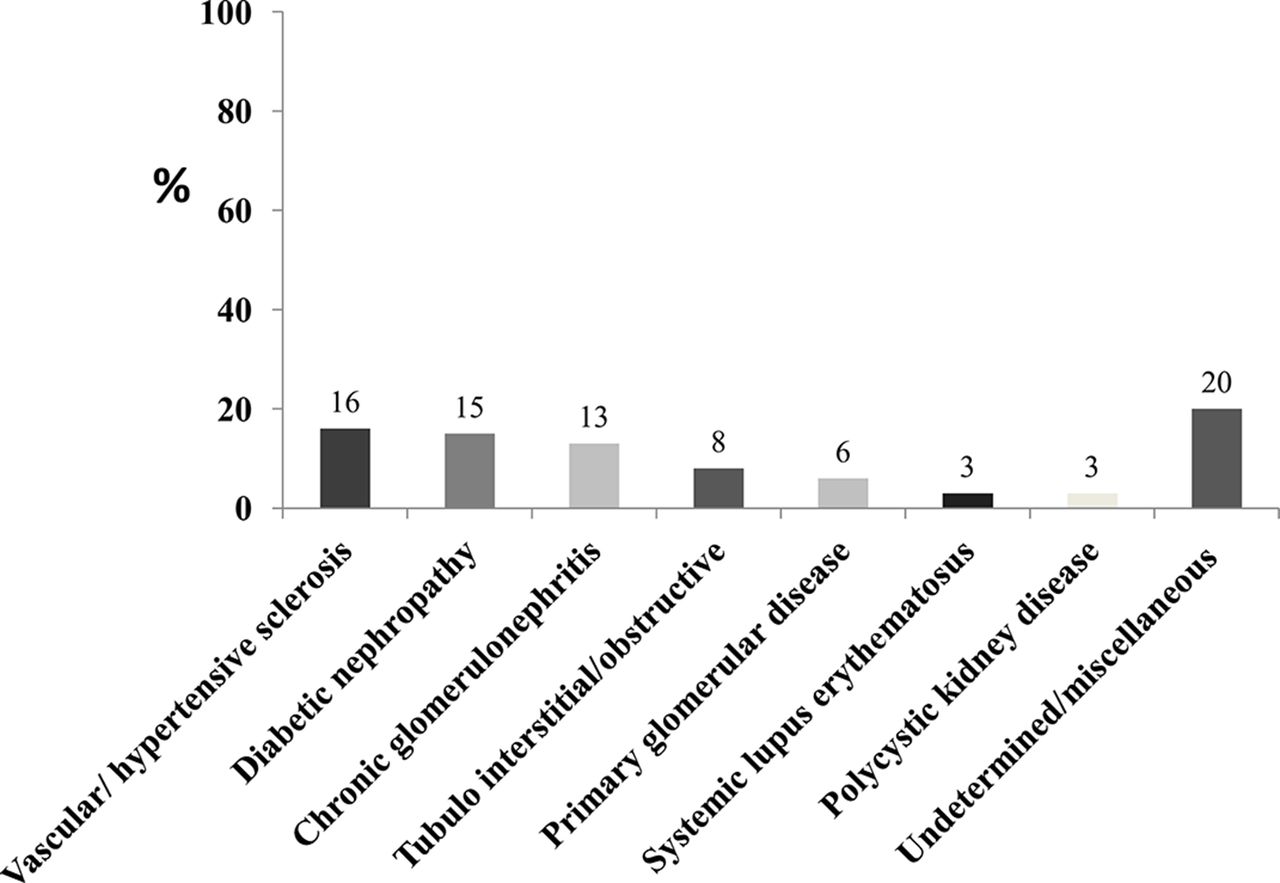
Forty-two studies were conducted specifically to clarify the underlying cause of CKD31–72 (online supplementary table 2). The diagnosis was biopsy-proven in 17 studies.33 39 41 43–45 48 54 55 58 60 63 67–70 72 Vascular/hypertensive sclerosis was the main cause of CKD (16%), followed by diabetic nephropathy (15%), chronic glomerulonephritis (13%), tubulointerstitial/obstructive (8%), primary glomerular diseases (6%), systemic lupus erythematosus (3%) and polycystic kidney disease (3%). The causes of CKD were undetermined/miscellaneous causes in one-fifth of the patients (20%) (figure 3).
{kind=link}
![[bmjopen-2016-015069-SP3.jpg]](https://bmjopen.bmj.com/content/bmjopen/8/1/e015069/DC3/embed/inline-supplementary-material-3.jpg?download=true){kind=link}
{kind=link}
{kind=link}
Main causes of chronic kidney disease.
Discussion
This systematic review focuses on the burden of CKD on the entire African continent. We assessed 152 papers published between 1 January 1995 and 7 April 2017 reporting the epidemiology of CKD in the general population and in specific chronic conditions in Africa. The CKD prevalence reported in our review should be interpreted with caution. Our estimates may be affected by the analytical heterogeneity used to measure creatinine and albuminuria. Serum creatinine concentrations are affected by intraindividual variability with over 20% changes within a 2-week period171 and most Jaffe assays overestimate serum creatinine.172 The resulting bias could vary according to the creatinine concentration, specific assay, manufacturer and calibration material used. Although the IDMS calibration standardisation has reduced the bias and improved the inter-laboratory comparability,173 the number of studies reported using IDMS was low in Africa. Moreover, CKD prevalence may additionally be influenced by albuminuria assays, which are affected by inter-laboratory differences.174 The different equations used to estimate GFR could be a source of bias. The systematic underestimation of measured GFR at higher estimated GFR by the MDRD equation is well known, and may reflect higher creatinine generation in healthy individuals compared with individuals with CKD in whom the MDRD equation was derived. This bias is reduced substantially, but not completely, by the CKD-EPI equation, which was derived from studies including people without CKD.175 In addition, differences in sample size, demographics and clinical characteristics are all significant limitations in this systematic review for making accurate estimates of the prevalence of CKD in African countries. Age and gender are well-known determinants of the risk of CKD development, progression and complication. While the prevalence of CKD tends to be higher in women, the disease is more severe in men, who also have a higher risk of all-cause and cardiovascular disease (CVD) mortality across different levels of renal function. However, the risk relationships of reduced eGFR and higher albuminuria with mortality were steeper in women than in men. Moreover, the risk of progression to ESRD at a given eGFR rate and urinary albumin-to-creatinine ratio seemed equivalent in men and women.176 177 The lack of information on the prevalence of CKD by age and gender in studies included in this systematic review—only 11% of the included studies reported CKD prevalence by either age or gender groups—limits the value and the reliability of pooled estimates of CKD prevalence in Africa and in its macro-areas. To circumvent this limitation, we showed the prevalence of CKD in the various studies in relationship to the proportion of men and age in the same studies. However the number of studies is too small for reliably capturing the effect of age and gender on CKD prevalence in Africa. Furthermore, only five studies79 142–145 assessed the KDOQI chronicity criterion, which is a fundamental element of the current definition of CKD by this organisation. A single elevated serum creatinine, reduced eGFR or an abnormal urinalysis should initially be viewed as a screening test, and the diagnosis of CKD should be confirmed with repeated tests, additional work-up and clinical judgement.178 Thus, estimates in this review should be seen as a pragmatic attempt to evaluate the dimension of CKD as a public health issue on the African continent.
CKD is now considered to be an important component of the epidemic of non-communicable diseases in economically developed and low–income/middle-income countries alike. In a seminal meta-analysis published in 2014, Stanifer et al 9 for the first time drew attention to the public health relevance of CKD in the sub-Saharan Africa, a vast area comprising 85% (947.4 million) of the whole African population.9 In the present systematic review, the lowest prevalence of CKD (4%) was reported in the Northern Africa macro-area, including Egypt, Libya, Tunisia, Algeria, Morocco, the Western Sahara and Mauritania, and the highest (16.5%) was observed in West/Central West Africa, which includes Benin, Burkina Faso, the island nation of Cape Verde, Gambia, Ghana, Guinea, Guinea-Bissau, Ivory Coast, Liberia, Mali, Mauritania, Niger, Nigeria, Cameroon, the island of Saint Helena, Senegal, Sierra Leone, São Tomé and Príncipe and Togo. The average prevalence in the entire African continent was 10.1%. The global CKD prevalence was reported to be 13.4%.179 In sub-Saharan Africa in Stanifer et al’s meta-analysis, the prevalence of CKD was 13.2%,9 which is close to that reported in the same area in our review (14.02%). Among the general population of economically developed countries, CKD has 13.6% prevalence in the USA.180 In Europe, the reported prevalence is lower and more homogeneous, being 8.9% in the Netherlands, 6.8% in Italy, 5.2% in Portugal, 4.7% in Spain and 3.3% in Norway.181 CKD prevalence in some Asian countries was higher than the estimates in the USA and in Europe, being 17.5% in Thailand,182 15% in India,183 13% in Japan,184 11.9% in Taiwan185 and 9.9% in China.186 Overall, the estimated prevalence of CKD at the general population level in African countries appears to be comparable and possibly even higher than that reported in other continents. This may be at least in part due to the low-quality data for the prevalence of CKD in Africa related to poor sampling techniques, unreliable kidney function measurements and the different definitions used.
In our review, the prevalence of CKD in surveys based on hospitals or primary care centres (36%) is close to that in Swiss primary care centres (36%).187
Poverty-related factors such as infectious diseases secondary to poor sanitation, inadequate supply of safe water, environmental pollutants and high concentrations of disease-transmitting vectors continue to play an important role in the development of CKD in low-income countries. Although rates of diabetic nephropathy are rising, chronic glomerulonephritis and interstitial nephritis are among the principal causes of CKD in many countries.188
In Africa, infectious diseases such as HIV, bilharziasis, malaria, hepatitis B and C represent an almost unique cluster of risk factors responsible for CKD.189 HIV/AIDS is pandemic in Africa, with a prevalence ranging from 0.5% in Senegal190 to 27.4% in Swaziland.191 The global success in bringing effective antiretroviral treatment (highly active antiretroviral therapy (HAART)) to HIV-infected patients in Africa has determined the emergence of chronic medical illnesses such as HIV-related CKD.192 Up to 50% of kidney diseases in HIV-infected persons result from a wide array of non-HIV-associated nephropathy pathologies, ranging from glomerulonephritis to diabetic nephropathy.193 We found that 5.6% of patients with HIV complained of renal dysfunction. This figure is lower than that reported in economically developed countries such as France, USA, China, Spain and Brazil.194–198 CKD was higher among patients with HIV not receiving HAART compared with those on HAART. Variation in the proportion of patients with HIV affected by CKD depends on the heterogeneity in the definition used to determine renal dysfunction, the proportion of the study population on HAART, diverse ethnicities, the associated comorbidities and the nutritional status of the study population. Patients with HIV are more prone to nutritional deficiencies due to malabsorption, impaired oral intake and the wasting syndrome. Increased availability of HAART has led to some improvement of the nutritional status of patients. However, for certain individuals, undernutrition and weight loss persist despite therapy. Malnutrition exacerbates side effects, alters drug pharmacokinetics and impinges on adherence, thereby limiting the beneficial effects of the therapy.199 Furthermore, differences in HIV clades or strains in African patients200 and genetic factor201 may influence the replication capacities within the isolated renal reservoir and thus lead to a diversity in clinical presentations.80
Regarding systemic autoimmune diseases such as lupus, a study conducted among patients with lupus from Senegal showed that almost three-quarters (71.0%) of the patients with this disease had evidence of renal involvement.19 This isolated figure is higher than that reported in other countries.202–204 More than one-third (39%) of patients with rheumatoid arthritis had CKD,20 which is higher than that reported from Taiwan.205
Even though there are no sufficient data to precisely reconstruct historical trends, the profile of CKD causes has changed during the last decades. Interstitial nephritis and glomerulonephritis were the main causes of CKD in North Africa,206 and CKD was principally caused by chronic glomerulonephritis and hypertension in East and Tropical Africa.207 208 Today, the spectrum of causes of CKD in Africa is dominated by diabetes mellitus and hypertension.209 We found that the prevalence of vascular/hypertensive and diabetic nephropathies as a cause of CKD (16% and 15%, respectively) exceeded that caused by chronic glomerulonephritis (13%).
Our review has both strengths and limitations. The major strengths include a thorough systematic search of electronic databases and the inclusion of all comprehensive studies with a transparent assessment of CKD prevalence by two independent reviewers. The fact that our literature search was limited to PubMed and Ovid Medline but did not include the African Index Medicus, like it was done by Stanifer et al in the meta-analysis of CKD in sub-Saharan Africa9, is a limitation of our study. Because there was a huge discrepancy in the definitions used to identify CKD, the methods of creatinine measurement, urine protein assessment and in the quality of the reporting, we decided to adopt an inclusive strategy. Our primary interest was to identify all studies conducted among different population groups in Africa providing information on CKD and to reconstruct a tentative scenario of the epidemiological dimension concerning disease in the entire African continent. Methodological limitations notwithstanding this review compiled estimates suggesting that the CKD burden in Africa is at least as concerning as that in economically developed countries. The lack of a consistent definition of CKD makes it difficult to compare the burden of CKD across studies in various countries. Moreover, the failure to demonstrate chronicity when defining CKD is a common limitation of studies investigating CKD prevalence in Africa. It was reported that a single test in time has an extremely poor positive predictive value for confirmation of CKD compared with repeated testing 3 months later. Failure to repeat testing may lead to a significant overestimation of CKD prevalence and underestimation of the burden of CVD in CKD.210 In addition, observational studies are subject to bias and residual confounding, which are difficult to account for and there are limitations due to the heterogeneity that arises from differences in age and sex distributions. This poor data quality reported in different studies is considered as a cumbersome problem limiting the accuracy in assessing the burden of CKD in Africa.
In conclusion, CKD in Africa appears to be at least as common as in other continents, and as such it constitutes a true public health priority with major cost burden to healthcare systems worldwide. Targeted screening of high-risk groups (including those patients with with hypertension, diabetes mellitus and HIV, and persons with occupational exposures) should likely be instituted as the first step in kidney disease prevention whenever and wherever affordable and feasible. Education to increase awareness of CKD among healthcare workers and patients, and the promotion of healthy lifestyles, should be engrained in preventive programmes. The treatment of hypertension and diabetes mellitus is of obvious relevance. Nurses and other health workers should be trained to manage these conditions at the local level if we are to curb the incidence of CKD and to avert the added burden of CKD complications to diabetes, hypertension and infectious diseases, the deadly trio of risk factors underlying the CKD epidemic in Africa.
Acknowledgments
We would like to thank the following professors and physicians for their help in providing the articles we evaluated in our review:
Professor Olutayo Alebiosu, Professor Ahmed Donia, Professor Rashad Barsoum, Professor Carel IJsselmuiden, Professor Laurent Forcard, Professor Anatole Laleye, Professor Nestor Pakasa, Professor Imaobong Etuk, Professor Ifeoma Ulasi, Professor Abubakr Abefe Sanusi, Professor Gbenga Ayodele, Professor Raida S Yahya, Professor Mohammed Benghanem Gharbi, Professor Fatma Ben Moussa, Dr Ikechi Okpechi, Dr Alaya Akram, Dr Adebowale Ademola, Dr Oluyombo Rotimi, Dr KS Nayak, Dr Guy Neild, Dr Rasheed Gbadegesin, Dr Sidy Mohamed Seck, Dr Amr El-Husseini Mohamed, Dr Fasika M Tedla, Professor Adewale Akinsola, Professor Olanrewaju Adedoyin, Dr Halle Marie Patrice, Dr Emmanuel Agaba, Professor Miriam Adhikari, Dr BT Bello and Dr Zidane Djelloul.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.↵
- 157.↵
- 158.↵
- 159.↵
- 160.↵
- 161.↵
- 162.↵
- 163.↵
- 164.↵
- 165.↵
- 166.↵
- 167.↵
- 168.↵
- 169.↵
- 170.↵
- 171.↵
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.↵
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.↵
- 186.↵
- 187.↵
- 188.↵
- 189.↵
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.↵
- 199.↵
- 200.↵
- 201.↵
- 202.↵
- 203.↵
- 204.↵
- 205.↵
- 206.↵
- 207.↵
- 208.↵
- 209.↵
- 210.↵
Footnotes
Contributors SA, DB and CZ: conceptualised and designed the study. SAE, GD and ED: participated in revising the articles included in the review and retrieved the necessary information. DB and GT: supervised the data capture and analysis. SAE, DB and GT: analysed and interpreted the data. SAE, DB and CZ: drafted and critically revised the manuscript. All of the authors read and approved the final manuscript.
Funding SA was granted a European Renal Association-European Dialysis and Transplantation Association (ERA-EDTA) fellowship at CNR-IFC/IBIM, Clinical Epidemiology and Physiopathology of Renal Disease and Hypertension of Reggio Calabria, Italy, and this work was completed during her training. This article was written in the framework of the Advisory Program of the ERA-EDTA YNP (Young Nephrologists’ Platform), which is an official body of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association). SA was an advisee of ERA-EDTA YNP Adviser-Advisee Program (Adviser: DB).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are published in the manuscript.