Article Text

Abstract
Objectives The aim of this systematic review was to assess incidence rates of laboratory-confirmed influenza (LCI) outcomes among infants under 6 months of age.
Design Systematic literature search and review of indexed studies in PubMed, EMBASE, the Cochrane Library and CINAHL Plus from inception to 19 April 2017.
Setting Population-based estimates from community or hospital settings.
Participants Infants under 6 months of age.
Primary and secondary outcome measures LCI illness in ambulatory care settings, LCI hospitalisation, LCI intensive care unit admission and LCI death. Only studies with population-based incidence data were included.
Results We identified 27 primary studies, 11 of which were from the USA, four were from other non-US high-income settings and the remaining were from lower-middle-income or upper-middle-income countries. Most studies (n=23) assessed incidence of LCI hospitalisation, but meta-analysis to pool study-specific rates was not possible due to high statistical and methodological heterogeneity. Among US studies, the reported incidence of LCI hospitalisation ranged from 9.3 to 91.2 per 10 000 infants under 6 months for seasonal influenza, while the only US-based estimate for pandemic H1N1 influenza was 20.2 per 10 000 infants. Reported rates for LCI hospitalisation for seasonal influenza from other countries ranged from 6.2 to 73.0 per 10 000 infants under 6 months, with the exception of one study with an estimated rate of 250 per 10 000 infants. No events were reported in five of the nine studies that evaluated LCI death among infants under 6 months.
Conclusion Our review of published studies found limited data on LCI outcomes for infants under 6 months, particularly from non-US settings. Globally representative and reliable incidence data are necessary to fully evaluate influenza disease burden and the potential impact of maternal influenza immunisation programme on morbidity and mortality in young infants.
- influenza
- hospitalisation
- infant
- systematic review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This review of laboratory-confirmed, population-based estimates of influenza incidence highlights the relative lack of studies that specifically report influenza outcomes among infants under the age of 6 months.
The majority of data identified in this review originate from the USA, deriving primarily from just two influenza surveillance systems, posing challenges for estimating the impact of maternal influenza immunisation programmes on infant influenza outcomes, particularly for low-income and middle-income countries.
We were unable to perform any meta-analyses due to high methodological and statistical heterogeneity.
Introduction
The influenza virus is a common pathogen identified in young children with acute lower respiratory infections, such as pneumonia and bronchiolitis,1 globally accounting for approximately 10% of all respiratory hospitalisations in children under 18 years2 and approximately 3% of postneonatal deaths.3 Influenza virus infection can also manifest in various other conditions including seizures, wheezing, croup, otitis media and occasionally encephalitis and encephalopathy,4–7 and it can progress to secondary bacterial pneumonias or exacerbate underlying chronic medical conditions.
Infants under 6 months of age are considered to be at high risk for severe influenza and associated complications due to documented high rates of influenza-associated hospitalisation8–12 and mortality.7 However, since influenza vaccines are not licensed for use in this age group due to poor immunogenic responses to the vaccine,13 protection of newborns and young infants from influenza virus infection and related complications requires alternate strategies.14 One such strategy is immunisation of pregnant women with influenza vaccine, which has been shown to reduce influenza virus infection among young infants through transplacental transfer of maternal anti-influenza antibodies.15–17
A 2011 systematic review and meta-analysis by Nair et al 1 estimated the global incidence of influenza outcomes among children under the age of 5 years and concluded that influenza in young children results in significant utilisation of health services, particularly among infants younger than 1 year. However, age-specific estimates for infants under 6 months were not reported.1 There is a paucity of published data on incidence of influenza outcomes among children in this younger age group,14 yet these data are necessary for informing evidence-based decision making regarding vaccination programmes, provision of appropriate health services and prioritising future research. In 2014, the WHO formed a working group18 to systematically review the evidence and estimate incidence rates of laboratory-confirmed influenza (LCI) outcomes among infants less than 6 months of age.
Methods
In consultation with the WHO influenza working group,18 we developed a systematic review protocol (available on request). This manuscript was prepared following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses recommendations.19
Search strategy and study selection
Our search strategy was developed by an experienced medical information specialist based on the review protocol (available from author on request) and informed by the approach used by Nair et al in their systematic review of the global influenza burden among young children.1 We searched PubMed, EMBASE, the Cochrane Library and CINAHL Plus with Full Text from inception to 19 April 2017. Our strategies used a combination of controlled vocabulary (eg, ‘Influenza, Human’, ‘Infant Mortality’ and ‘Incidence’) and keywords (eg, influenza, neonate and rate). No language or date restrictions were applied but animal-only and opinion pieces (eg, comments, editorials and interviews) were removed from the initial search results where possible. No unpublished data were pursued or included. Specific details regarding the search strategies appear in online supplementary appendix 1.
Supplementary file 1
We used Reference Manager V.12 to download our search results and remove duplicates. Abstracts were then exported to Abstrackr (http://abstrackr.cebm.brown.edu/) for screening and data abstraction. Two teams of two reviewers independently screened all titles and abstracts to identify potentially relevant articles for full-text review. Disagreements between reviewers were resolved through discussion and consensus. The same two teams of reviewers carried out full-text screening to identify studies that met all the inclusion and exclusion criteria for data extraction and quality assessment. While extracting data, the reviewers also examined the reference lists to identify potentially relevant articles that may have been missed during screening.
We included studies that reported original data on population-based incidence rates for the following LCI outcomes among infants under 6 months of age: LCI illness in ambulatory care settings, LCI hospitalisation, LCI intensive care unit (ICU) admission and LCI death. We excluded studies that did not ascertain LCI outcomes either throughout at least one full influenza season in geographic settings with defined seasonality, or otherwise for at least one full year. We also excluded studies if influenza was not examined as a primary outcome, but rather as a co-infection in a study population identified on the basis of another infectious disease (eg, influenza co-infection in a cohort of hospitalised measles cases20). Finally, studies that used a case definition that was not clearly defined or consistently applied, and those that were not population based or had a population denominator of fewer than 500 infants under 6 months of age were excluded. We included data from the comparator group of any randomised controlled trials (RCTs) on influenza immunisation during pregnancy if the study otherwise met our inclusion criteria.
Data extraction and quality assessment
Data from each included study were abstracted by one of two reviewers using a standardised data extraction form which was first pilot-tested to ensure a high level of agreement between reviewers. We extracted the following, where available, from each study: author; publication year; study design; study country; study population and size; age ranges studied; subject selection criteria; length of surveillance period and influenza season (particularly specifying the 2009–2010 pandemic vs other seasons); circulating influenza virus strains; definition and type of outcomes included in the study; methods for ascertaining cases (eg, active vs passive surveillance); criteria used for influenza testing; laboratory assay used to confirm influenza diagnosis; influenza vaccination coverage in pregnant women in locations where the studies were conducted. We also extracted information, where available, on the numerator and denominator for each incidence rate; any statistical analyses performed, including variables used to compute adjusted rates; crude and adjusted incidence rates for each outcome with 95% CIs or other measures of variance; any sensitivity analyses presented in the paper. Study authors were contacted as needed to clarify data or methods. Two independent reviewers evaluated the quality of each study. Since all included studies were case series or surveillance studies that did not include comparative analyses, we used a modification of the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Descriptive/Case Series to assess individual study quality.21 This checklist assesses four items: clearly defined case inclusion criteria, objective assessments of exposure and outcome, and sufficient follow-up time for outcome ascertainment. In addition, we assessed the quality of evidence across studies using an adaptation of the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.22 23 For each outcome, we determined a GRADE rating of high quality, moderate quality, low quality or very low quality for each outcome according to criteria such as study design and limitations, inconsistency in study findings and imprecision.22 23
Data synthesis and analysis
We qualitatively summarised individual study characteristics in descriptive tables. For each outcome, we extracted the incidence rates and 95% CIs as reported by the primary study when they were provided, and otherwise computed them using raw study data where possible. We estimated the numerator or denominator values when an unadjusted incidence rate was reported along with only one of the other two data points. We interpreted incidence rates (computed using person-time denominators for infants under 6 months) and incidence proportions (computed using the estimated size of the population of infants under 6 months) as approximately equivalent. No attempt was made to mathematically convert one to the other since most studies that reported an incidence proportion used the total number of infants under the age of 1 year and divided in half, which would approximate 6 months of person-time follow-up assuming a static population with no losses to follow-up. We used Stata SE software V.12 (Stata-Corp LP) to generate pooled incidence estimates for LCI hospitalisation via random effects meta-analyses24 and the I2 statistic to quantitatively assess statistical heterogeneity.25 Pooled incidence estimates were not reported when statistical heterogeneity was high (ie, I2 >75%); however, qualitatively, we explored sources of heterogeneity in subgroups to augment our interpretation. A priori, we hypothesised that heterogeneity would likely arise due to differences in pandemic versus seasonal influenza, study population, case ascertainment methods and study quality. We generated forest plots using the R package ‘ggplot2’ (R Foundation for Statistical Computing).
Results
Study selection
We identified 9298 records through our initial electronic literature searches; following de-duplication, 5998 went through initial title and abstract screening. We identified 150 potentially relevant articles and excluded 125 after full-text review, leaving 25. Most manuscripts (81/125; 65%) were excluded because they lacked age-specific data on infants under 6 months. During full-text screening, we added two articles that had originally been excluded by our systematic query but were subsequently identified through a hand search of reference lists.16 26 This brought the total number of primary studies included in our review to 27 (figure 1).
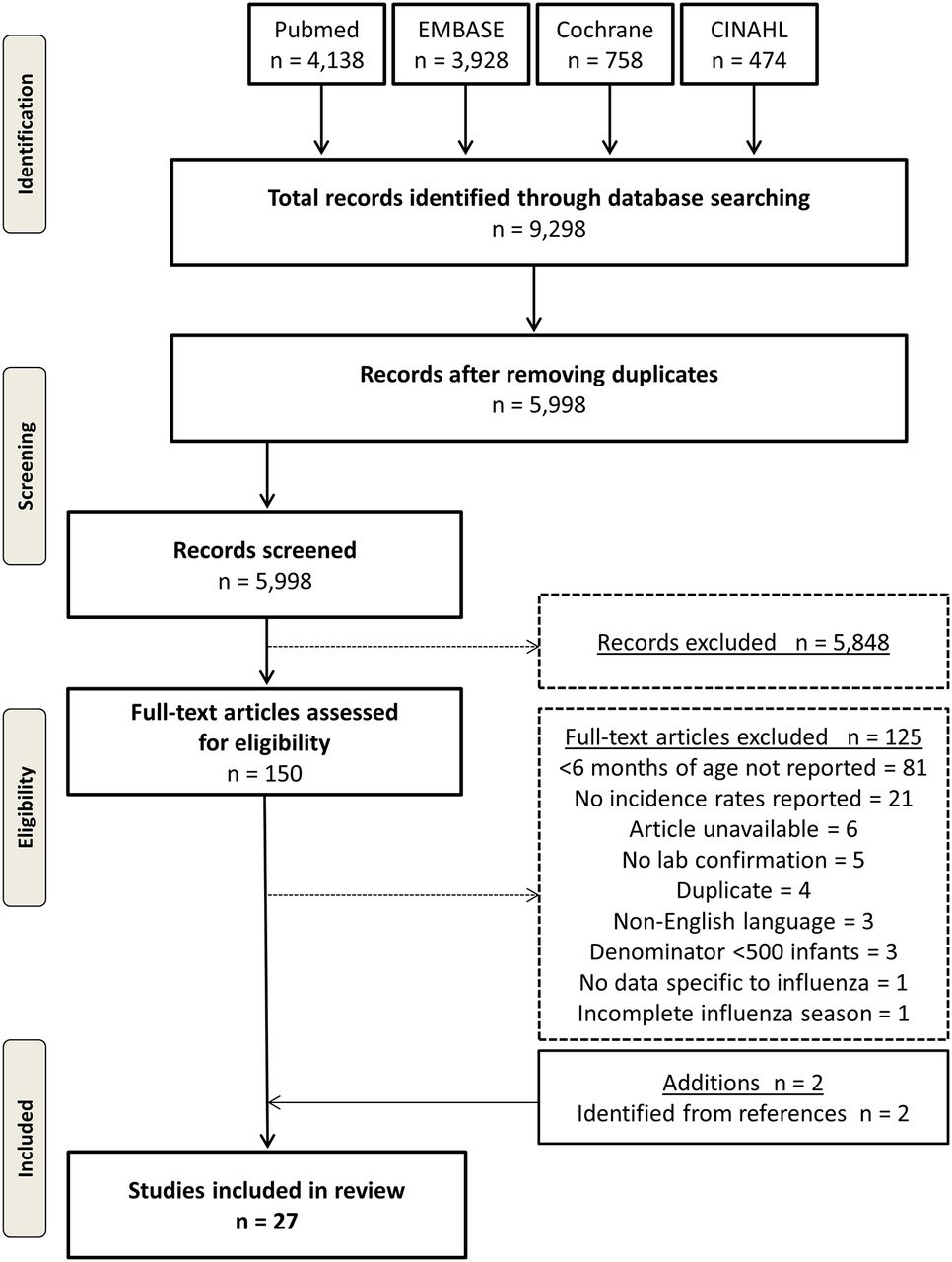
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram showing selection of studies.
Study characteristics
Nearly half (11/27) of the studies originated from the USA,7–9 26–33 and the remaining were from lower-middle-income (n=5),11 17 34–36 upper-middle-income (n=7)16 37–42 and other non-US high-income settings (n=4)43–46 (table 1). There were no studies from low-income countries. Twenty-three studies assessed LCI hospitalisation,8 9 11 16 17 26–33 35 36 38–41 43–46 six studies assessed LCI illness in ambulatory care settings,9 16 17 34 37 42 seven studies reported LCI ICU admission9 26 32 39 40 45 46 and nine assessed LCI deaths7 11 16 17 26 28 35 40 44 (table 1). All studies were published in 2004 or later and reported data from influenza seasons between 2000 and 2014. Two studies exclusively reported influenza outcomes from the 2009 H1N1 pandemic time period,40 46 six reported data from the 2009 pandemic time period along with other influenza seasons27 35–37 43 44 and the remaining reported LCI outcomes from seasonal influenza epidemics. Most studies used reverse transcription (RT) PCR laboratory testing methods, either alone or in combination with other methods, to confirm influenza from patient samples (online supplementary table S1). Four of the 25 non-randomised trials included in this review39 41 44 45 provided some contextual information on uptake of maternal influenza immunisation in their study population, but none provided specific rates (online supplementary table S2). We were able to obtain additional clarifying data from four16 27 40 42 of six studies by contacting study authors. Only two studies received a score lower than 4/4 on the modified JBI Critical Appraisal Checklist—one such study did not assess all influenza outcomes using objective criteria44 and the other did not clearly document the case definition.46 Applying the modified GRADE assessment,23 the quality of evidence for incidence rates of LCI hospitalisation of infants under 6 months of age was deemed to be moderate, while the quality of evidence for the other three outcomes was considered low (online supplementary appendix 2). In large part, this determination was based on high heterogeneity in incidence rates across studies, partly due to variability in surveillance methodologies and methods used to compute rates. Moreover, other than hospitalisation, the number of studies reporting data for the other outcomes of interest was small.
Supplementary file 2
Characteristics of the primary studies and LCI outcomes assessed
LCI illness in ambulatory care settings
Six studies, two of which were from lower-income or lower-middle-income countries, assessed LCI illness in ambulatory care settings9 16 17 34 37 42 (table 2). Five of the studies used RT-PCR to confirm influenza virus infection, and one used either RT-PCR or viral culture9(online supplementary table S1). In a community-based prospective cohort study conducted between 2009 and 2011 in the Cajamarca region of Peru, researchers conducted active household surveillance to identify infants with symptoms of acute respiratory illness for confirmatory influenza laboratory testing. In this study, the adjusted incidence of LCI illness among infants less than 6 months of age was 35 per 100 person-years of follow-up (95% CI 26 to 48).37 Using similar active surveillance methods, the RCT from South Africa reported an incidence of LCI illness among infants born to non-HIV infected women in the placebo group of 3.6 per 100 infants (95% C: 2.6 to 5.0),16 and the RCT from Mali reported an incidence of 8.3 per 100 person-years among infants in the control arm.17 In a study conducted over three influenza seasons in the Suzhou District of China, the incidence of LCI illness among infants under 6 months ranged from 2.3 per 100 in 2013–2014 to 2.9 per 100 in 2012–2013.42 Finally, data from the New Vaccine Surveillance Network (NVSN), a population-based active sentinel surveillance programme operating in three regions of the USA (Davidson County, Tennessee; Hamilton County, Ohio; and Monroe County, New York), estimated a rate of LCI illness based on outpatient clinic visits among infants under 6 months of 2.8 per 100 infants (95% CI 0.7 to 11.1) in 2002–2003 and 5.9 per 100 infants (95% CI 2.8 to 12.8) in 2003–2004.9 We did not consider statistical meta-analysis of this outcome due to the variable geographic settings and methodologies employed by the studies. For instance, the latter NVSN study estimated incidence rates from population-based surveillance of outpatient clinic visits,9 while the study from Peru used community-based surveillance including a household component,37 and the two RCTs employed active surveillance with weekly contact with study participants.16 17
Incidence estimates of laboratory-confirmed influenza illness in ambulatory care settings among infants under 6 months of age
LCI hospitalisation
Graphical and tabular summaries of individual estimates originating from the 23 studies that reported incidence rates of LCI hospitalisation can be found in figure 2 and online supplementary table S3. Ten of the 23 studies originated from the USA; six of those reported data from one of two population-based active surveillance programme: the Emerging Infections Program (EIP)27 28 or the NVSN.8 9 29 32 Two additional US studies led by Grijalva et al reported estimates using capture–recapture methods based on surveillance data from both the EIP and NVSN systems,30 31 and the remaining two US studies reported data from separate systems.26 33 In the USA, estimated rates of LCI hospitalisation of infants less than 6 months of age during seasonal epidemics varied from a low of 9.3 per 10 000 infants (95% CI 7.9 to 10.9) in 2006–200728 to a high of 91.2 per 10 000 infants (95% CI 67 to 145)30in 2003–2004. The only US-based estimate for the 2009 pandemic H1N1 time period was 20.2 per 10 000 infants (95% CI 18.1 to 22.5).27

{kind=link}
{kind=link}
Incidence estimates of laboratory-confirmed influenza (LCI) hospitalisation among infants under 6 months of age. Heterogeneity I2: 100%. All estimates can be found in online supplementary table S3.
The 13 non-US studies (four from high-income countries, six from upper-middle-income countries, two from lower-middle-income countries and one from a low-income country) reported similar LCI hospitalisation rates for seasonal influenza. Most incidence rates for seasonal influenza ranged from 6.2 per 10 000 infants (95% CI 3.1 to 9.3) in China in 200739 to 73.0 per 10 000 infants (95% CI 40.6 to 121.7) in Spain in 2003–2004.11 However, a higher estimated rate was reported from one postpandemic study of seasonal influenza from China (250 per 10 000 infants under 6 months in 2010–2011, 95% CI 213 to 292).41 The highest estimate from non-US based studies from the 2009 pandemic H1N1 influenza time period was 259 per 10 000 person-years (95% CI 97.0 to 689) in Kenya.36
Although 10 studies from the USA presented incidence rates of LCI hospitalisation of infants under 6 months, there was overlap in a number of seasons among the eight studies using data from the EIP and NVSN surveillance programmes (table 3). For instance, two studies reported the same rate from the NVSN system for the 2000–2001 season (24.0 per 10 000 infants),9 32and similar combined season rates for 2000–2004 from the NVSN system (reported as 43.0 per 10 000 infants29 and 45.0 per 10 000 infants9). In addition, estimates are available from both the EIP and the NVSN for several years. In such instances, incidence rates from the NVSN system were consistently higher in magnitude than the EIP estimates. Moreover, in two studies, Grijalva et al combined data from the EIP and NVSN surveillance systems using a capture–recapture methodology30 31—a surveillance method that attempts to estimate the extent of under-ascertainment of cases using information from two or more data sources.47 This methodology yielded a higher combined incidence rate of LCI hospitalisation than was provided by either system alone.30 31For instance, in 2003–2004, which was a more severe influenza season, individual EIP and NVSN estimates were 29.6 per 10 000 infants (95% CI 26.7 to 32.8)28 and 72.0 per 10 000 infants (95% CI 53.0 to 92.0),9 respectively. Using the combined data from both systems, the revised estimate was 91.2 per 10 000 infants (95% CI 67.0 to 145.0).30
Incidence estimates of laboratory-confirmed influenza hospitalisation among infants under 6 months of age from US-based influenza surveillance systems
LCI ICU admission
LCI ICU admission rates for infants under 6 months are available from seven studies9 26 32 39 40 45 46 (table 4). However, all rates shown in table 4 were computed by review authors, either due to non-reporting in the original study9 22 28 33 34 37 or due to graphical presentation of rates in a figure only.46 Estimated rates of LCI ICU admission for seasonal influenza ranged from a low of 0.5 per 10 000 infants (95% CI 0.8 to 16.5) between 2000–2001 and 2003–2004 in the Salt Lake City area of the USA9 to a high of 3.5 per 10 000 between 2001 and 2004 in the surveillance counties covered by the NVSN (95% CI 1.7 to 6.4).26 The absolute number of LCI ICU admissions of infants under 6 months was very low in all study populations (from a low of zero32 to a high of 12 admissions40). Two studies were conducted during the 2009 H1N1 pandemic time period—in Argentina, Libster et al reported a rate of LCI ICU admission of 2.9 per 10 000 infants (95% CI 1.6 to 5.0)40 and in Israel, Stein et al reported a similar rate of 2.5 per 10 000 infants (95% CI 0.79 to 6.0).46
Incidence estimates of laboratory-confirmed influenza ICU admission among infants under 6 months of age
LCI death
Nine studies included LCI death among infants under 6 months of age as an outcome.7 11 16 17 26 28 35 40 44 In six of the nine study populations, surveillance for LCI deaths was conducted, but none were identified11 16 26 35 44 (table 5). Bhat et al reported data from enhanced national-level surveillance of paediatric LCI deaths in the USA during the 2003–2004 season.7 In this study, there were 18 deaths of infants under 6 months of age, corresponding to a rate of 0.88 per 100 000 infants (95% CI 0.52 to 1.39), which was the highest among all paediatric age groups up to 18 years. In a smaller US surveillance study using data from the EIP system operating in 10 states, three influenza deaths of infants under 6 months were recorded during 2003–2004 to 2007–2008 combined, with a corresponding rate of 0.41 per 100 000 person-years (95% CI 0.11 to 1.12).28 Among all nine studies, the highest rate of LCI deaths in infants was reported in Buenos Aires, Argentina, for the 2009 pandemic H1N1 time period; two deaths were recorded, and the LCI mortality rate was 5 per 100 000 infants (95% CI 0.82 to 16.1).40
Incidence estimates of laboratory-confirmed influenza death among infants under 6 months of age
Discussion
In this systematic review, we provide a summary of published data up to April 2017 regarding the incidence of LCI outcomes among infants under 6 months of age. Our review of 27 studies covering 14 influenza seasons demonstrates a relatively wide range of estimates in incidence rates for several LCI outcomes in this age group. This broad distribution is likely associated with biological variability of influenza clinical disease and epidemiology and host immunity, as well as methodological factors of the studies themselves, including differences in care provider practices for influenza testing and hospital admission. In particular, estimates of rates for LCI hospitalisations, the most frequently reported and best-described outcome among these studies, ranged 10-fold, from 9.3 to 91.2 per 10 000 infants, within the USA alone, and varied even more widely in other settings. The incidence of LCI hospitalisations was generally higher during the 2009 pandemic H1N1 time period (20 per 10 000 infants40 to 25936 per 10 000 person-years) than during seasonal influenza years, though few estimates from the H1N1 pandemic time period were available. Our work also highlights the relative lack of studies that specifically report influenza outcomes in this vulnerable age group and the limited information included in studies that do include such findings. LCI outcomes other than hospitalisation, such as ICU admission and death, were even less commonly assessed and varied markedly in the level of detail described. Moreover, the majority of data identified in this review come from the USA, deriving primarily from just two influenza surveillance systems, indicating the constrained geographic coverage of the collected datasets. These limitations pose challenges for estimating the potential impact of maternal influenza immunisation programmes on infant influenza outcomes, particularly for low- and middle-income countries.
Our review methodology used a comprehensive search strategy that emphasised high sensitivity to capture a broad set of articles for screening. We subsequently restricted our review to laboratory-confirmed, population-based estimates of influenza incidence, ensuring greater consistency and stability of rates across studies. Our review also benefits from a number of strengths regarding the original studies identified through our search. First, the majority of the data come from well-established surveillance systems that cover several seasons and include additional evaluations (eg, capture–recapture methods30 31) to confirm the validity of their findings. This consistency adds to the stability of the range of estimates reported here and provides a better understanding of the effects of seasonal variation on annual burden estimates. Second, the included studies generally obtained high scores in the quality assessment tool providing some assurance that they met at least minimum quality criteria.
Nevertheless, there are several important limitations. Among the primary studies, the different surveillance methodologies (eg, passive versus active surveillance; different sensitivity of diagnostic tests; recruitment only in a subset of days per week; different denominators or methods to calculate incidence rates; surveillance only during part of the year; rate adjustment for various factors) contributed to the heterogeneity of the results. Moreover, some studies reported only a small number of seasons or a limited geographic area which may not provide a fully representative assessment of typical influenza incidence. Although none of the non-randomised studies specifically reported the uptake of maternal influenza immunisation in their study population, the majority were either studies from the USA during pre-2009 pandemic seasons when rates were low,48 or were from settings without recommendations for influenza immunisation during pregnancy; consequently, this was unlikely to be an important contributor to the heterogeneity in incidence rates. We were unable to include several studies that aggregated data from infants under 6 months within larger age strata, thus not reporting data specific to this policy-relevant age group. Future surveillance studies should report data for infants under 6 months, even if only as supplementary data, to facilitate future pooling and meta-analyses. The reports themselves were incomplete at times, lacking numerator data, denominator data or precision estimates, precluding the ability to perform meta-analysis. Even with full reporting of the data, key factors may have influenced the accuracy and completeness of specific surveillance approaches. Importantly, Grijalva et al 30 31 demonstrated that the two US surveillance systems each underestimate the incidence of LCI hospitalisations. In both 2003–2004 and 2004–2005, the incidence of LCI hospitalisation was higher using the combined capture–recapture methodology47 than when estimated using either NVSN or EIP data alone. Finally, several of the US-based studies described overlapping seasons across multiple reports, thus contributing to a risk of some duplicate reporting.
Although we evaluated studies that included a narrower age range compared with the review by Nair et al,1 our results are generally consistent with the findings presented in that review, which reported rates of severe acute lower respiratory infection (corresponding to influenza hospitalisation) ranging from 10 to 170 per 10 000 person-years among infants under 1 year of age. These consistent findings support the overall interpretation that influenza has a significant role in early infant respiratory morbidity. Of note, the incidence rates reported for influenza hospitalisation in the control arms of the randomised clinical trials included in this review16 17 were at the lower end of the range of estimates (one infant LCI hospitalisation in each trial, corresponding to a rate of 9.8 per 10 000 infants in South Africa (personal communication: M Nunes, 7 December 2016), and 10.8 per 10 000 person-years in Mali [personal communication: M Tapia, 15 Dec 2016]). These low rates compared with other estimates could be due to the epidemiological characteristics of the particular influenza seasons or due to the close observation of subjects and opportunity for treatment and follow-up afforded by the active surveillance in the trials. Using prospective active surveillance methods, these two trials likely provide the best estimates of the incidence of LCI illness in an ambulatory setting among infants under 6 months: 3.6 per 100 infants16 and 8.3 per 100 person-years of follow-up.17 Another recent trial of maternal influenza immunisation in Nepal, published subsequent to our literature search, documented an incidence rate of LCI illness in an ambulatory setting of 18.1 per 100 person-years of follow-up among infants in the placebo group.49
In conclusion, our systematic review demonstrates that existing data on LCI outcomes among infants under 6 months of age are sparse, of varying quality, and heavily weighted towards high-income populations. More research is needed in key regions to obtain a more globally representative picture of the incidence of influenza outcomes among young infants. In particular, estimates are required from the low-income and low-middle-income countries of Asia and Africa where, in absolute numbers, the majority of cases occur. Higher quality data will be essential in order to allow global and country-level policymakers to make evidence-based decisions that appropriately prioritise interventions, such as maternal influenza immunisation for reducing influenza disease in young infants who are, themselves, not eligible for influenza vaccination.
Acknowledgments
We acknowledge members of the WHO Taskforce to Evaluate Influenza Data to Inform Vaccine Impact and Economic Modelling, a working group of the WHO Initiative for Vaccine Research, for their contributions through early discussions about this study. We are grateful to Glen Zinck (PATH) for his help with project organisation, to Dr. Corinne Riddell (McGill University) for her assistance with producing Forest plots, and to Laura Walsh (University of Ottawa) for her assistance with updating the data extraction. We additionally thank Dr. Kevin Pottie (University of Ottawa), Dr. Michael Gravett (University of Washington) and Dr. Dayre McNally (University of Ottawa) for their thoughtful reviews of an earlier version of this manuscript.
Acknowledgments
We acknowledge members of the WHO Taskforce to Evaluate Influenza Data to Inform Vaccine Impact and Economic Modelling, a working group of the WHO Initiative for Vaccine Research, for their contributions through early discussions about this study.
We are grateful to Glen Zinck (PATH) for his help with project organisation, to Dr. Corinne Riddell (McGill University) for her assistance with producing Forest plots and to Laura Walsh (University of Ottawa) for her assistance with updating the data extraction. We additionally thank Dr. Kevin Pottie (University of Ottawa), Dr. Michael Gravett (University of Washington) and Dr. Dayre McNally (University of Ottawa) for their thoughtful reviews of an earlier version of this manuscript.
References
Footnotes
Contributors NB, KMN and JRO designed the study protocol. BS designed and ran the systematic search strategy. JJ, ZM and MAK screened the articles, extracted the data and assessed the quality of individual studies. DBF, ZM, MAK and JRO contacted study authors for additional information. DBF interpreted the data and wrote the first draft of the manuscript. All authors critically revised the manuscript for intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding This work was supported by the Bill & Melinda Gates Foundation through the WHO. The research was coordinated by PATH. DBF and MAK received financial support from the WHO’s Initiative for Vaccine Research. The authors also acknowledge the Centers for Disease Control and Prevention, which provides financial support to the WHO’s Initiative for Vaccine Research (U50 CK000431).
Disclaimer JRO is an employee of the WHO. The authors alone are responsible for the views expressed in this publication and they do not necessarily represent the decisions, policy or views of the WHO.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data set is available on request from the corresponding author.