Article Text

Abstract
Objectives This study aims to provide a comprehensive description of noise levels in operating rooms (ORs) in a tertiary care hospital in China. Additionally, the study aims to examine the deviation in noise levels from international and internal standards as well as the differences in noise levels by category of surgery and day of the week.
Methods We monitored noise levels in 23 ORs in a tertiary care hospital in China between August 2015 and March 2016. Dosimeters were used to determine noise levels. The noise data collected in the dosimeter were downloaded to an IBM computer for subsequent analysis. One-way analysis of variance and Student’s t-test were used to examine the differences in noise levels.
Results The noise level in the ORs ranged between 59.2 and 72.3 dB(A), with 100% of the measurements exceeding the recommended hospital noise standards. There was substantial similarity in noise levels from Monday to Friday (F=1.404, p=0.234), with a range between 63.7 and 64.5 dB(A). The difference in noise levels by category of surgery was significant (F=3.381, p<0.001). The results of the post hoc analysis suggested that ophthalmic surgery had significantly higher noise levels than otolaryngological surgery or general surgery.
Conclusions Ophthalmic surgery had significantly higher noise levels than otolaryngological or general surgeries. High noise levels were identified in all evaluated ORs during weekdays, and these levels consistently exceeded the currently accepted standards. These findings warrant further investigation to determine the harmful effects of noise on both patients and staff in ORs.
- noise
- operating room
- hospital
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This investigation is the first time dosimeters which have been used to monitor noise levels in operating rooms. Dosimeters have real-time monitoring metrics that provide more precise measurements of noise levels than the tools used in previous studies.
This study used dosimeters to measure noise over an extended period during a wide range of surgical procedures. This approach allows the readings to be saved and the noise-level distribution to be identified, including the examination of noise levels versus surgical time, location and category.
One limitation of this study was that specific events, such as the use of noisy tools, could not be directly linked to the recorded noise levels.
Introduction
The finding that noise represents an established health hazard has been demonstrated in hospitals and particularly in operating rooms (ORs). Excessive noise may have negative effects on patient care and safety. Noise in the OR may also affect the health and performance of staff. WHO, Environmental Protection Agency (EPA) and the country of China have established guidelines and standards for safe noise levels in hospitals and ORs. WHO recommends that noise levels should not exceed 35 dB(A).1 The EPA guidelines state that noise levels should not exceed 45 dB(A).2 In China, regulations assert that noise levels in ORs should not exceed 50 dB(A).3 These standards stress that OR noise should be maintained at levels that are as low as possible.
Notwithstanding these standards or guidelines, hospitals are never quiet places. Busch-Vishniac and colleagues conducted a review of previous studies that examined noise levels in hospitals and determined that noise measurements consistently exceeded the recommended levels by an average of 20–40 dB(A).4 A corresponding significant linear increase in hospital noise levels has been identified since 1960, with increases averaging 0.38 dB per year during the day and 0.42 dB per year at night. Within hospitals, researchers are specifically concerned with noise in ORs, in which the mean noise level ranges between 51 and 75 dB(A).5 Previous studies have measured noise levels produced by tools used primarily during conventional surgeries.6–10 Several studies have reported the sound pressure levels for a particular surgery or specific surgeries.11–16
However, it is difficult to characterise noise in the OR based on these published articles. Previous studies were limited to surgical tools and specific surgeries; thus, it is not surprising that the typical patterns in sound pressure levels over the course of a workday within an OR cannot be characterised. In addition, based on these data, the distribution of noise levels cannot be identified, including noise levels versus time and category of surgery. In this study, we measured noise levels in 23 ORs according to the types of surgery performed with the aim of providing a comprehensive description of noise levels in ORs in a tertiary care hospital. We aimed to compare the deviation in noise levels from the currently accepted standards and compare the differences in noise levels across the day of the week and type of surgery.
Methods
Overview
This cross-sectional study was approved by the Institutional Review Board (IRB) of our hospital. The requirement for written informed consent was waived by the IRB because patient and staff data were not collected. We obtained permission from the hospital administration to place noise-monitoring equipment in the ORs. The investigator conducted non-documented observations to identify sources of noise originating from personnel, equipment, etc. All personnel were unaware of the ongoing noise monitoring, and no changes were made that would control noise levels or disturb staff routines throughout the study. This manuscript adheres to the applicable Equator guidelines. This cross-sectional study was conducted in a tertiary care hospital located in a densely populated district in the city of Beijing, China. The study was conducted between August 2015 and March 2016. During the first period, noise levels were monitored in 17 ORs in the surgical building. All types of surgeries with the exception of ophthalmological and otolaryngological surgeries were included. During the second period, noise levels were measured in seven rooms in the ophthalmology and otorhinolaryngology departments. Decibel measurements of various noise sources were not undertaken due to the lack of an instrument to identify specific sources of noise.
Instrument
Personal noise dosimeters (Aihua, Model AWA5610B, Hangzhou, China) were used to determine noise levels. The dosimeter meets the International Electrotechnical Commission Standard (IEC) 61 672-2002 class 2 and Chinese National Standards (GB) GB/T15952-1995 class 2. The A-weighted scale, dB(A), was used in this study to measure noise levels. This scale is frequently used in clinical practice because it filters out the very low and very high frequencies to which humans are insensitive. The dosimeter provided a direct sound pressure reading and detected sound levels that ranged from 45 to 140 dB(A) with an accuracy of less than ±1 dB(A) over a temperature range of 0°C–40°C. Before measurements were obtained, each dosimeter was calibrated using a Model AWA6221A Sound Level Calibrator (Aihua Instruments), which complied with IEC 60 942-2004 class 1 in a controlled environment at a 94.0 dB sound pressure level from a single-point source with a 1 kHz frequency.
Procedure
Measurements were obtained during weekdays to ensure that surgical action would occur within the rooms. Before measurements were obtained, the dosimeters were fully charged and calibrated. Noise levels were automatically measured and monitored in our study setting. In general, noise measurement commenced on the investigator’s way to the OR at, on average, 06:50 to 07:30. The instruments were placed in the ORs under study before the staff entered the ORs for operation preparation at 08:00. In general, the staff were unaware of the instrument placement and noise monitoring to ensure that they would work as usual. No behavioural changes were made, including controlling conversation or abstaining from the playing of music.
The instrument was placed inside each room throughout the full-shift period from before 08:00 to anaesthesia emergence and transportation of the last patient out of the OR at, on average, 17:00. In each room, the instrument was positioned so that it did not interfere with the surgical schedule and was outside of the sterile field. The instrument was placed within 2 m of the anaesthesia machine at a height of 1.5 m from the floor. The noise data collected in the dosimeter were downloaded to an IBM computer for subsequent analysis.
The sample interval was 2 s; that is, 2 s of A-weighted equivalent continuous sound levels (LAeq,2s) were collected every 2 s. The LAeq,2s measurements were plotted against time using time-series plots to facilitate their graphical summarisation. An A-weighted equivalent sound pressure level in dB, as measured over the noise assessment period T (LAeq,T), was calculated for each room. The LAeq,T was calculated as follows17:

where T represents the entire noise assessment period and n represents the total readings that occurred over the period. The noise measurement in an OR from 08:00 to 17:00 allowed for the collection of 16 200  readings; therefore, T equalled 32 400 s, and n equalled 16 200.
readings; therefore, T equalled 32 400 s, and n equalled 16 200.
We obtained permission to view the surgical logs to identify operations that occurred within the measurement period. The surgery log provides a detailed description of the nature of each procedure and the division of surgery. In general, the same types of surgeries were performed in the same room on the same day. Using the data obtained from the dosimeters and logs, noise levels in each OR were calculated.
Statistical analysis
Data were exported from the dosimeters using their proprietary software and were subsequently analysed using MATLAB V.7.7 (R2008b) and SPSS for Windows, V.20.0 (SPSS). The distribution of LAeq,T across all ORs was graphically summarised using a histogram. One sample Student’s t-test was applied to examine the deviation in noise levels from international and internal standards. One-way analysis of variance was applied to examine the differences in noise levels among groups for categorical parameters (days of the week and category of surgery). The post hoc analysis used Bonferroni methods. All reported p values were two tailed, and p<0.05 was established as the level of significance.
Results
The study area was a surgical building in a tertiary care hospital in which annual operations number in the tens of thousands. According to the available data, 56 000 surgeries were performed in this hospital in 2015. Under the assumption that 1 year comprises 250 weekdays, 225 operations were performed each day. When this number was divided by the 48 ORs, it was estimated that nearly five consecutive surgeries belonging to the same category (eg, neurology and gynaecology) were conducted in a given room per day. Consecutive surgeries were defined as conditions in which the completion of one surgery resulted in the initiation of the next operation on the operating list. Based on our observations, the ORs varied in size from 10 to 20 m2. All rooms had hard surfaces and furnishings with no material added for sound absorption.
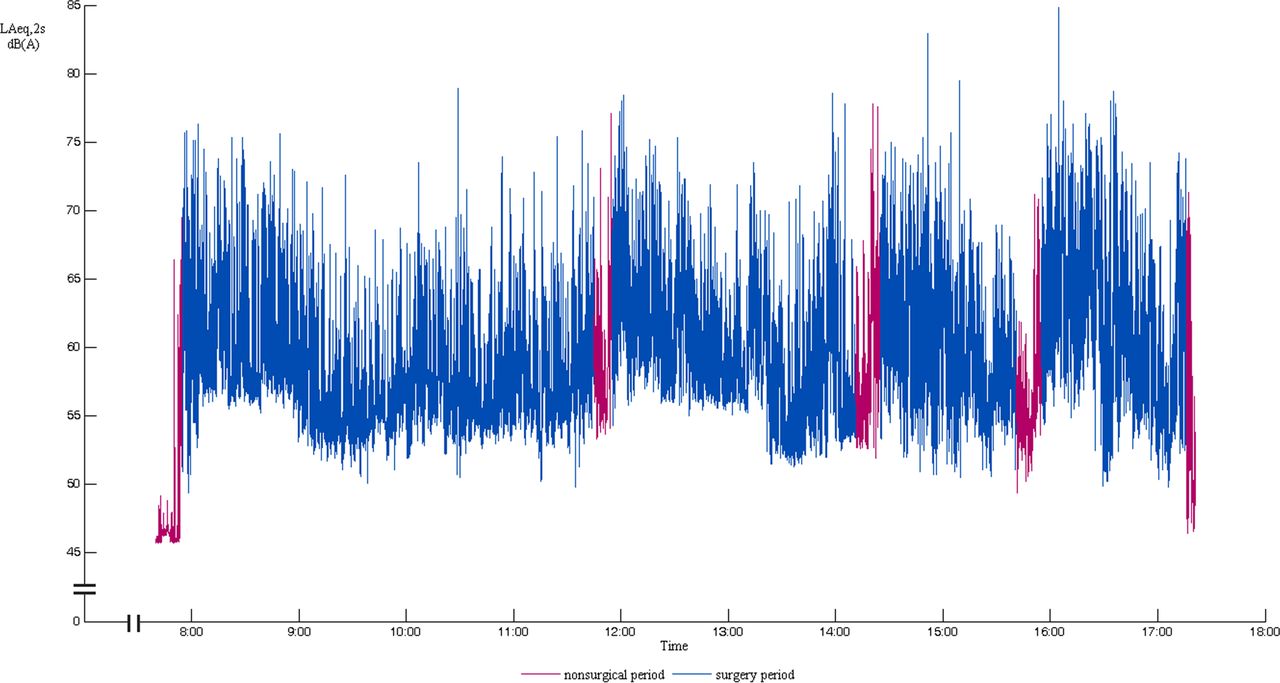
The plot for the LAeq,2s vs time (07:30 to 17:30) within an OR during the performance of gynaecological surgeries is shown in figure 1. Figure 1 presents a typical trace of the LAeq,2s vs time for an OR. With the passage of time, considerable variation in noise levels was identified. The noise level was below 50 dB(A) when the OR was unoccupied. The noise level incrementally increased with the entry of staff and patients, with a range of Leq from 50 to 85 dB(A). We identified the performance of four different surgeries during the measurement period, with a very short non-surgical interval between adjacent operations. The first surgery was performed from 07:55 to 11:44, the second surgery was performed from 11:55 to 14:10, the third surgery was performed from 14:25 to 15:40 and the fourth surgery was performed from 15:55 to 17:15. At the beginning of each surgery, noise levels were relatively high, with a range from 55 to 75 dB(A). The noise level gradually decreased, with a range from 50 to 70 dB(A) at the end of the surgery.

A-weighted equivalent sound pressure level measured in an operating room for gynaecological surgeries over a 10 hours period. The red line indicates the non-surgical period, and the blue line indicates the surgery period.
Noise data were collected in 23 ORs, with multiple measurements obtained in each OR, generating 225 LAeq,T data points. The distribution of the data is shown in figure 2. The horizontal axis represents the LAeq,T measurements, and the actual measured frequencies are presented on the vertical axis. The results indicated a noise level that ranged between 59.2 and 72.3 dB(A). None of the measured LAeq,T values complied with WHO, EPA or Chinese guidelines, with 100% of the measurements exceeding these standards. The mean noise level was 64.2 (±2.1) dB(A), which was 29.2 dB(A) higher than WHO standard (t=211.3, p<0.001), 19.2 dB(A) louder than the 45 dB(A) recommended by EPA (t=138.9, p<0.001) and 14.2 dB(A) higher than the Chinese standards (t=102.7, p<0.001). In addition to the overall distribution of the LAeq,T, the average noise levels across the different ORs ranged from 61.8 to 66.7 dB(A). The averages were calculated by averaging the multiple measurements for each OR.

{kind=link}
{kind=link}
The distribution of A-weighted equivalent sound pressure level measured in all operating rooms. The horizontal axis represents the LAeq,T measurements, and the actual measured frequencies are presented on the vertical axis.
The ORs were occupied on weekdays, and noise data were collected during these periods. As shown in table 1, each result was represented as an average over multiple measurements that were typically obtained in more than one OR. There was substantial similarity in noise levels from Monday to Friday (p=0.234).
Operating room noise levels on weekdays
Table 2 summarises the noise-level measurements by category of surgery (eg, neurology and gynaecology). The difference in noise levels detected in the ORs by category of surgery was significant (p<0.001). The post hoc analysis suggested that ophthalmic surgery (65.4 dB(A)) had higher noise levels than otolaryngological surgery (63.3 dB(A)) and general surgery (63.4 dB(A)).
Operating room noise levels by category of surgery
Discussion
The results indicated a noise level that ranged between 59.2 and 72.3 dB(A), which was substantially louder than the guidelines recommended by China, WHO and EPA. The recorded noise levels (64.2±2.1 dB(A)) indicated that ORs are noisy environments, a finding that is in line with other studies that have examined noise levels in ORs (51–75 dB(A)).5 11–16 No previously published results have shown noise levels in ORs that comply with WHO guidelines or other standards for hospital noise. Thus, the problem of excessive noise in the OR appears to be universal regardless of the type of hospital or geographical location.4 These findings clearly raise questions regarding the significance of these guidelines because the data imply that the current standards for hospital noise do not apply in the OR. The establishment of guideline values for sound pressure levels in the OR warrants future research.
The results suggested that ophthalmic surgery had significantly higher noise levels than otolaryngological surgery and general surgery. We did not obtain sound recordings; thus, we cannot identify the causes of the difference. Based on our observations, there was music playing in the ophthalmic surgery room, which may have accounted for the higher noise levels. This assumption warrants further investigation.
These data indicated that there was no discernible pattern that distinguished the noisiest OR from the least noisy OR. Based on our discussion with OR staff, their perception of noise is consistent with the observed narrow variation across the ORs. This warrants further study to investigate the staff’s perception of noise with a questionnaire or qualitative interviews.
In addition, there was substantial similarity in noise levels detected from Monday to Friday. This similarity may be largely attributed to the similarity in noise sources. Based on our observation, noise originated from both staff and equipment. Staff-related activities and conversations were a major component of OR noise. The functioning laminar airflow system generated steady noise over the period. The anaesthetic monitors generated many distracting alarms and alerts (on average, one to two alarms within several minutes). The surgical instruments (eg, power drills) generated instantaneous, sudden and distinct noise with a duration of several seconds. Further research is necessary to determine the decibel measurements of various noise sources within ORs and to estimate the degree of contribution of these sources to noise levels.
Excessive noise may be a threat to patient comfort and safety. Evidence suggests that more than one-third of patients perceive ORs as noisy, and 16% of patients feel stressed by the noise in this environment.18 The stapedius muscle, which normally contracts and protects the cochlea when exposed to loud sounds, may be weakened by anaesthetic drugs.19 Thus, we are concerned that patient hearing may be at risk when this natural reflex mechanism is abolished.
Excessive noise may also have detrimental effects on staff health. Evidence suggests that high noise levels (greater than 55 dB(A)) are associated with adverse events, such as hypertension, fatigue, annoyance, burn-out, stress and headaches.1 All LAeq,T values measured in the present study were greater than 55 dB(A), which suggests that excessive noise may pose a potential health risk to OR staff. Previous studies have suggested that anaesthetists are particularly susceptible to the hazards associated with excess noise14 because of their continuous presence in the room, their close proximity to noisy equipment and the finding that noise in the OR is louder during the critical anaesthesia components of care, such as induction and emergence, than at other critical points. Particular attention should be paid to the mental and physical health of anaesthetists.
Noise in the OR may also interfere with work progression. Surgeons, nurses and anaesthetists are engaged in complex mental activities that require a high degree of concentration. Staff members, particularly anaesthetists, may be at risk of being disturbed by noise. In one study, 84% of anaesthetists complained that noise levels in the OR negatively affected their work.14 In addition, significant worsening in mental efficiency and short-term memory test results have been identified in anaesthetists after exposure to prerecorded OR noise.20 OR noise may cause a decrease in auditory processing function.21 Researchers have also reported that noise has a negative effect on the ability of resident anaesthetists to detect changes in oxygen saturation with pulse oximetry.22 However, these studies were conducted in controlled settings. Future work is necessary to consider the impact of noise on anaesthetists under real working conditions.
In the OR, it is vital to ensure effective and high-quality communication among surgeons, nurses and anaesthetists. However, conversational ability may often be hindered by high levels of noise. To ensure speech communication, the signal-to-noise ratio should be at least 15 dB.1 With a normal voice level of 50 dB(A), the background level should not exceed 35 dB(A). The noise level in the OR ranged between 59.2 and 72.3 dB(A); staff members need to raise their voices to ensure good communication, thereby creating more noise. This noisy environment poses a potential risk of miscommunication, which may lead to unacceptable medical errors.
The adverse effects of noise within ORs may be ameliorated by the implementation of measures to minimise noise levels. The oversized return air inlet and poor design of the air exhaust contributed to noise levels. Specific attention should be paid to factors related to noise when decisions are made concerning air supplies and OR design. Consideration should be given to determine the minimum volume on the premise that surgeons and anaesthetists perceive auditory changes in equipment, and staff members subsequently adjust the volume to appropriate decibels. Efforts should be directed toward establishing systems for interpersonal communications and educating staff to reduce staff-related noise. Further research is required to demonstrate the impact of these measures by monitoring noise levels before and after their implementation.
This investigation is the first time dosimeters have been used to monitor noise levels in ORs. Dosimeters have real-time monitoring metrics, which provide more precise measurements of noise levels than the tools used in previous studies. The readings can be saved and the distribution of noise levels can be identified, including the examination of noise levels versus surgical time, location and category.
One limitation of this study was that specific events, such as the use of noisy tools, could not be directly linked to the recorded noise levels. In subsequent work, we intend to document these events, including their time and duration. Thus, it may be possible to identify noisy processes using qualitative records and time-series plots that examine changes in the LAeq,2s over time. The measurements described in this study were limited to ORs in a tertiary care hospital in China. Further work is required to determine noise levels in ORs in other hospitals.
Acknowledgments
We thank Liwei Wang, Yongzheng Han, Jiao Geng, Chunyi Wang and Pengxian Li (Resident, Department of Anesthesiology, Peking University Third Hospital, Beijing, China) for their help with the data analysis. Their contributions are sincerely appreciated.
References
Footnotes
Contributors XW collected and analysed noise data. LZ designed the study and provided interpretive analysis. GL and MX commented on the study plan and provided critical revision. BW and YL collected surgery logs and provided critical revision on the discussion. NL, LT and HZ discussed the results and provided critical revision. XG and YZ conceived the work, organised and coordinated the study, and commented on the manuscript. All authors participated in the review, drafting and final approval of the manuscript.
Funding The project was not supported by any organisation. The noise meters were purchased during the process of a cooperative programme with the State University of New York at Plattsburgh. The project was completed in 2011 and supported by grant number 1-R01-OH-002317 from the National Institute for Occupational Safety and Health in the USA.
Competing interests None declared.
Ethics approval The Institutional Review Board (IRB) of Peking University Third Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional unpublished data are available.