Article Text

Abstract
Objectives Poorly controlled type 2 diabetes mellitus (T2DM) is a major international health problem. Our aim was to assess the effectiveness of healthcare interventions, specifically targeting patients with poorly controlled T2DM, which seek to improve glycaemic control and cardiovascular risk in primary care settings.
Design Systematic review.
Setting Primary care and community settings.
Included studies Randomised controlled trials (RCTs) targeting patients with poor glycaemic control were identified from Pubmed, Embase, Web of Science, Cochrane Library and SCOPUS. Poor glycaemic control was defined as HbA1c over 59 mmol/mol (7.5%).
Interventions Interventions were classified as organisational, patient-oriented, professional, financial or regulatory.
Outcomes Primary outcomes were HbA1c, blood pressure and lipid control. Two reviewers independently assessed studies for eligibility, extracted data and assessed study quality. Meta-analyses were undertaken where appropriate using random-effects models. Subgroup analysis explored the effects of intervention type, baseline HbA1c, study quality and study duration. Meta-regression analyses were undertaken to investigate identified heterogeneity.
Results Forty-two RCTs were identified, including 11 250 patients, with most undertaken in USA. In general, studies had low risk of bias. The main intervention types were patient-directed (48%) and organisational (48%). Overall, interventions reduced HbA1c by −0.34% (95% CI −0.46% to −0.22%), but meta-analyses had high statistical heterogeneity. Subgroup analyses suggested that organisational interventions and interventions on those with baseline HbA1c over 9.5% had better improvements in HbA1c. Meta-regression analyses suggested that only interventions on those with population HbA1c over 9.5% were more effective. Interventions had a modest improvement of blood pressure and lipids, although baseline levels of control were generally good.
Conclusions This review suggests that interventions for T2DM, in primary care, are better targeted at individuals with very poor glycaemic control and that organisational interventions may be more effective.
- diabetes & endocrinology
- organisation of health services
- primary care
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of the study
This systematic review adds to the evidence regarding the effectiveness of healthcare interventions, which specifically target patients with poor glycaemic control of type 2 diabetes mellitus, in community settings.
There is no specific definition for ‘poor control’ diabetes in the literature, but by including all studies that had patients with a HbA1c ≥59 mmol/mol (7.5%), we captured the full range of poor glycaemic control and also examined other key risk factors such as blood pressure and lipids.
Data were pooled from 42 studies across four continents, enhancing the generalisability of the findings.
We did not account for medication use in the studies, but given that all included studies were randomised controlled trials, which would balance out delivery of medications, we think that differences in underlying medication usage may relate to how different interventions promote intensification of medications.
An individual patient data meta-analysis may answer further questions not possible in this review.
Introduction
Worldwide, type 2 diabetes mellitus (T2DM) is rising in prevalence and will exceed 4.4% of the world's population or 366 million by 2030.1 Despite a wealth of evidence regarding the importance of risk factor control in T2DM, many patients continue to have poor control of HbA1c, blood pressure and lipids. Up to 60% of the patients fail to meet target HbA1c levels.2 Similarly, over one-third of the patients with T2DM have inadequate blood pressure control.3 Poorly controlled T2DM—and its associated microvascular and macrovascular complications—is associated with higher morbidity, higher mortality, poorer quality of life and substantial economic burden.4
Several studies have examined interventions designed to support the delivery of diabetes care in the community to improve glycaemic and cardiovascular risk factor control.5–11 A 2011 review of community-based interventions including all patients with T2DM, comprising 68 studies, showed that only one-third had a statistically significant improvement in one of the relevant clinical outcomes for diabetes: HbA1c, blood pressure or lipids.8 The majority of the included studies targeted all patients with T2DM without focussing on those with poor control. Although no overall effect was noted, combining organisational with professional (multifaceted) interventions was concluded to be more beneficial than single interventions and the highest quality multifaceted randomised controlled trials (RCTs) tended to include decision support interventions and elements. A 2013 review looked at 48 cluster RCTs, assessing the effectiveness of quality improvement (QI) strategies on the management of diabetes (both T1DM and T2DM).11 It suggested that QI interventions, which intervened at a system level on diabetes management, were associated with the largest benefits in glycaemic control and that the effectiveness of interventions targeting healthcare practitioners varied with baseline glycaemic control, being more effective with patients with worse control.11 A 2016 review, of T1DM or T2DM in primary care, looked at the effects of Clinician Education, Clinician Reminders, Team Changes, Case Management, Electronic Patient Registry, Telemedicine and Audit and Feedback.10 Including 30 studies, it concluded that multifaceted interventions on multidisciplinary teams were most effective. Interventions targeting family physicians were only effective if computerised feedback on insulin prescribing was provided.
Four large RCTs from North America and the UK have investigated the effects of intensive management of hyperglycaemic and cardiac risk factors on mortality in T2DM across all settings.12–17 Uncertainty remains regarding intensive glycaemic management for all patients with T2DM, with concerns about aggressive reductions in HbA1c.18 Targeted reductions in cardiovascular and glycaemic risk factors in certain vulnerable populations (cognitively impaired, disabled and frail) have been advocated.19 Interventions that specifically target those with very poor control of risk factors may be more beneficial than those targeting all patients, achieving the benefits of cardiovascular and glycaemic control, but without the potential risks of intensively lowering HbA1c in all persons with T2DM. The effect of interventions specifically targeting patients with poorly controlled T2DM in primary care is unknown.
Our aim was to assess the effectiveness of healthcare interventions delivered in primary care and community settings, targeting poorly controlled T2DM, which seek to improve glycaemic control, blood pressure and lipids.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to standardise the conduct and reporting of the research and the protocol was registered on PROSPERO.20
Data sources and searches
We searched articles in all languages from the Cochrane Library, Pubmed, Embase, Web of Science and SCOPUS from 1990 to 31 December 2016. Reference lists of all included papers were searched. Secondary searching of all references from included studies was also conducted. Online supplementary appendix 1 outlines the search string.
supplementary appendix 1
Study selection
We considered RCTs, controlled clinical trials, controlled before and after studies and interrupted time series analyses meeting the Cochrane Effective Practice and Organisation of Care (EPOC) quality criteria.21 Studies published in all languages were eligible.
Population
Individuals with ‘poorly controlled’ T2DM were our population of interest. Though there is a broad consensus about the importance of achieving good glycaemic control for the reasons described, there are no validated cut-offs, which define ‘poor-control’ of T2DM for targeted interventions. Poorly controlled T2DM has been defined based on elevated glycated haemoglobin levels in the literature, with different thresholds of HbA1c described, from over 59 mmol/mol (7.5%), over 64 mmol/mol (8.0%) to over 75 mmol/mol (9.0%).22–24 In this review, we considered participants to have poorly controlled T2DM if their HbA1c was over 59 mmol/mol (7.5%) (or if over 80% of the population in a study had a HbA1c over 59 mmol/mol). Similarly, there is no defined cut-off as to what defines ‘poorly controlled’ blood pressure. We identified studies primarily based on poor glycaemic control and also included participants in these studies who had uncontrolled hypertension or elevated cholesterol/lipids, if the risk factor level was above that of an accepted international target, as designated by the study authors. Where studies included patients with ‘poor control’ based on a range of risk factor profiles, for consistency, we only included a study if 80% of the population had a HbA1c over 59 mmol/mol (7.5%).
Interventions
We included interventions delivered by healthcare professionals specifically aiming to target patients with poor control of T2DM, based in primary care or community settings. The primary healthcare setting was defined as providing ‘integrated, easy to access, healthcare services by clinicians who are accountable for addressing a large majority of personal healthcare needs, developing a sustained and continuous relationship with patients and practicing in the context of family and community’.25 We excluded drug trials though interventions could have involved treatment intensification. Interventions were defined as simple if they had one identifiable component and multifaceted if they had more than one element. We excluded trials performed within the hospital or the hospital-outpatient setting. The Cochrane EPOC taxonomy of interventions was used and the predominant intervention type was defined using five categories including organisational, patient-centred, regulatory, financial and professional. Examples of these intervention types are provided in online supplementary appendix 2.21
supplementary appendix 2
Comparison
Comparison groups were included if they received usual care in that setting for T2DM. Controls were also included if they received minor enhanced elements of care, such as education leaflets, which the study authors believed did not go beyond usual care in most settings.
Outcome measures
Primary outcomes included glycaemic control (HbA1c), blood pressure (systolic or diastolic) and lipid levels, but if studies did not include HbA1c, they were excluded. Secondary outcomes included patient-reported outcome measures (PROMs) (eg, health-related quality of life), utilisation of health services, behavioural outcomes such as medication adherence, provider behaviour, acceptability of service to patients and providers, economic outcomes and adverse events.
Data extraction and quality assessment
Two reviewers (MEM and RG) read the titles and/or abstracts of the identified references and eliminated irrelevant studies. Studies that were deemed eligible for inclusion were read in full and their suitability for inclusion in the systematic review was independently determined by two reviewers. Disagreements were managed by a third, independent reviewer (SMS). The following information was extracted: (a) details of intervention, (b) participants, (c) clinical setting, (d) study design, (e) outcomes, (f) author information. We contacted authors for missing data.
Risk of bias in articles was assessed using the Cochrane Handbook for systematic reviewing and EPOC criteria.26 Two review authors independently assessed the risk of bias of each included study against the criteria described in the Cochrane risk of bias tool. We explicitly judged each of these criteria using: low risk of bias, high risk of bias or unclear risk of bias (either lack of information or uncertainty over the potential for bias). We resolved disagreements by consensus and consulted a third review author to resolve disagreements if necessary. An overall assessment of a study's risk of bias was determined using EPOC guidance, with judgement and consensus reached between two reviewers (MEM and SMS).26
Data analysis
For continuous data, we calculated the treatment effect using mean differences (MDs) and 95% CIs. No binary outcomes were included. Revman software was used to perform the analysis, determine heterogeneity and produce forest plots to illustrate pooled estimates.21 Stata version 13 was used to investigate publication bias by creating funnel plots and using Egger's test to assess funnel plot asymmetry.27 A random-effects analysis was performed and heterogeneity across the studies was quantified using the I2 statistic. The I2 statistic describes the percentage of the variability in effect estimates which is due to heterogeneity rather than sampling error (chance).28 If the I2 statistic was >50%, it was deemed that there was significant heterogeneity between the studies.
Subgroup analyses were performed for primary outcomes based on a priori assumptions, as per the PROSPERO protocol.20 For HbA1c, we explored the possible effects of subgroups: (a) the type of intervention based on the EPOC taxonomy (see online supplementary appendix 2); (b) study quality and (c) baseline HbA1c in the study populations (HbA1c 7.5%–9.4% or ≥9.5%). After reviewing, the included studies we also included study duration as a subgroup (<12 months or ≥12 months), as a wide range in study duration was found. Subgroup analyses for systolic blood pressure (SBP) and diastolic blood pressure (DBP) explored the effects of intervention-type based on the EPOC taxonomy.
When important heterogeneity was identified, we investigated its causes using meta-regression. Meta-regression is an extension to subgroup analysis that allows the effect of continuous, as well as categorical, characteristics to be investigated.29 Meta-regression was performed to explore the effects of: (a) study quality (using the overall assessment risk of bias); (b) study population characteristics (eg, gender, age and baseline HbA1c and SBP); (c) intervention type (EPOC taxonomy) and (d) study duration on the primary outcomes.29 Random effects meta-regression was performed using Stata version 13.27
Results
Overall 18 829 titles were screened and 42 full text articles met the inclusion criteria (figure 1: PRISMA flow diagram). All 42 studies were RCTs, encompassing 50 interventions in total, comprising 11 250 patients.22–24 30–68 No other eligible study designs were identified.
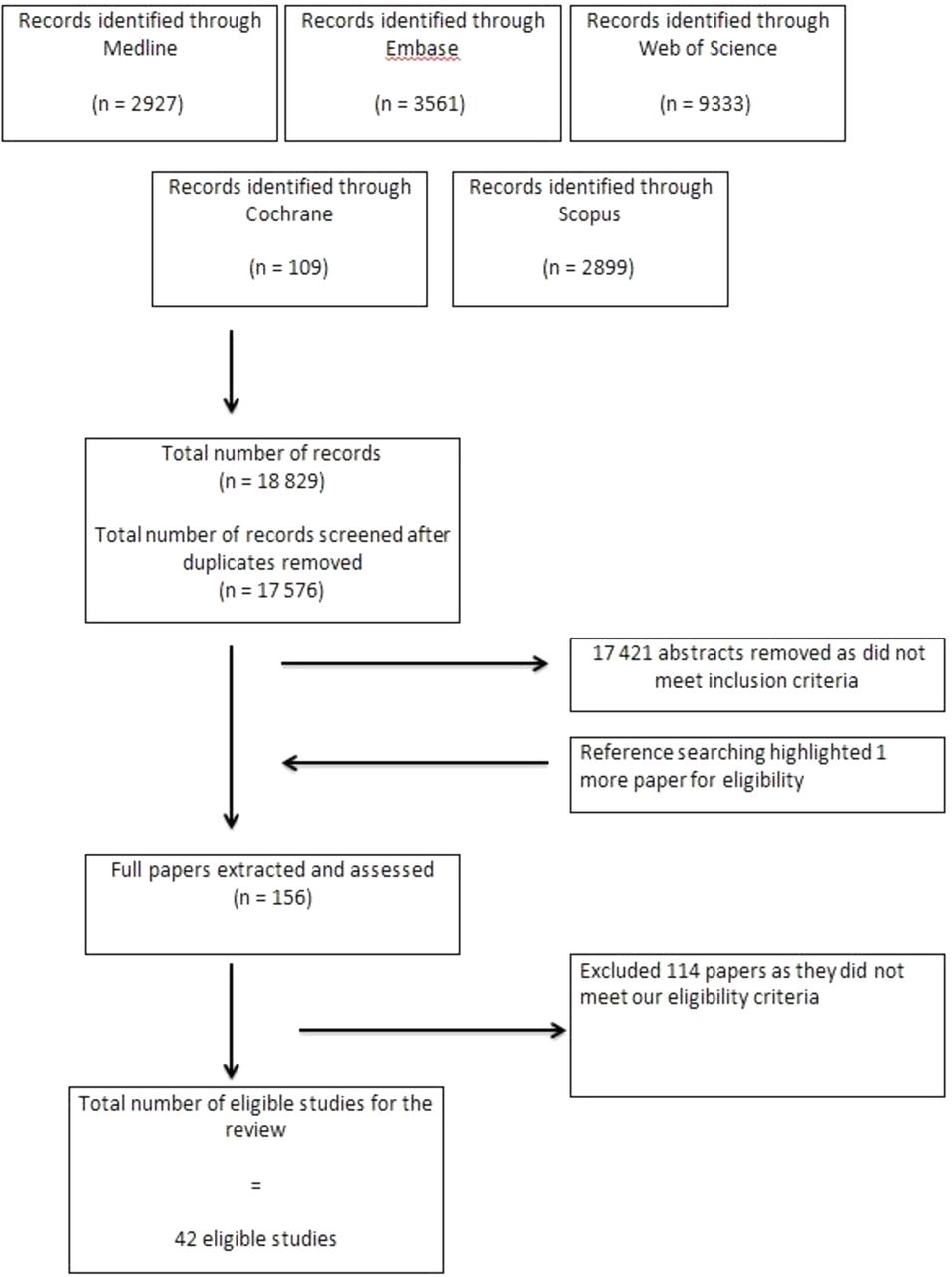
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow sheet.
Characteristics of studies
Twenty-nine of the 42 studies were conducted in USA, 9 in Europe, 2 in Australia, 1 in Mexico and 1 in Israel. Follow-up of outcomes in the studies varied in length from 353 to 36 months.46 The mean HbA1c at baseline across all studies was 9.5% (95% CI 9.3% to 9.8%). The mean age of patients in the studies was 58.0, varying from 47.9 (62) to 67.5 (41) partly reflecting different inclusion criteria (table 1). Thirty studies explicitly defined their study population as ‘poorly controlled’, ‘complicated’ or ‘persistently poorly controlled’, whereas the other 12 had poorly controlled T2DM with HbA1c ≥59 mmol/mol (7.5%) as per the review inclusion criteria. Twenty-seven of the 42 studies reported SBP results22–24 30–36 38 39 41 45 46 48–51 54 58–60 62 65 66 68 and of these, 23 reported DBP.22–24 31 32 34–36 38 39 41 45 46 48 49 51 54 58 59 62 65 66 68 Twenty of the studies reported a lipid outcome.23 24 30–32 35 36 38 39 41 45 46 48 51 56 58 62 65 66 68 All of the 42 studies reported at least one secondary outcome. Two studies were excluded from primary outcome analysis due to lack of appropriate data, despite efforts to contact authors.31 61
Characteristics of included studies
Interventions were all complex with multiple components. Studies were categorised based on the predominant intervention element using the EPOC taxonomy. The included interventions were categorised as predominantly patient-centred (n=20, 48%), organisational (n=20, 48%), financial (n=1, 2%) or professional (n=1, 2%). One study44 comprised two intervention arms with a patient-centred and financial intervention (included as a patient-centred predominant intervention in our analysis). Descriptions of the interventions are outlined in table 1.
The 20 patient-centred interventions in our review included 4 telephone-based,34 41 56 58 5 computerised/mobile phone-based,32 36 52 61 68 1 video-based,51 5 peer-support-based,30 38 44 49 65 3 self-monitoring-based37 50 64 and 2 -culturally supportive self-management interventions.39 45 The 20 organisational interventions included 5 pharmacist interventions performing case management,35 40 47 48 57 6 nurse case management interventions,23 31 46 53 55 60 3 web-based/telemedicine/telephone case management interventions,24 59 63 3 new-clinic-based interventions,43 54 66 1 community health-worker intervention,62 1 psychological intervention22 and 1 lay health worker intervention.67 Eight interventions had an mHealth or telehealth component.33 36 45 52 56 59 65 68 More detailed descriptions of the interventions are outlined in online supplementary appendix 3.
supplementary appendix 3
Risk of bias
All 42 studies were RCTs, with six being cluster RCTs. Overall, 25 studies were classified as having a predominant low-risk of bias (59.5%),22–24 32–36 39 41 42 45 46 51 53–55 58 59 62–66 68 13 studies had an unclear-risk (31%)30 31 37 38 40 44 47 49 56 57 60 61 67 and 4 RCTs were classified as having a high-risk of bias (9.5%)43 48 50 52 (see online supplementary appendix 4). Blinding of outcome assessment was classified as low-risk in all studies. Attrition bias was evident in seven studies. Online supplementary appendix 5 outlines the summary judgements for both overall risk of bias and predominant intervention type, which were used in the meta-regression analysis.
supplementary appendix 4
supplementary appendix 5
There was no evidence of publication bias in the studies included in the HbA1c (p=0.37) or SBP analysis (p=0.54). However, there was some evidence of publication bias in the studies included in the DBP analysis (p<0.01) (see online supplementary appendixes 6(a) and 6(b)).
supplementary appendix 6(a)
supplementary appendix 6(b)
Primary outcomes
HbA1c
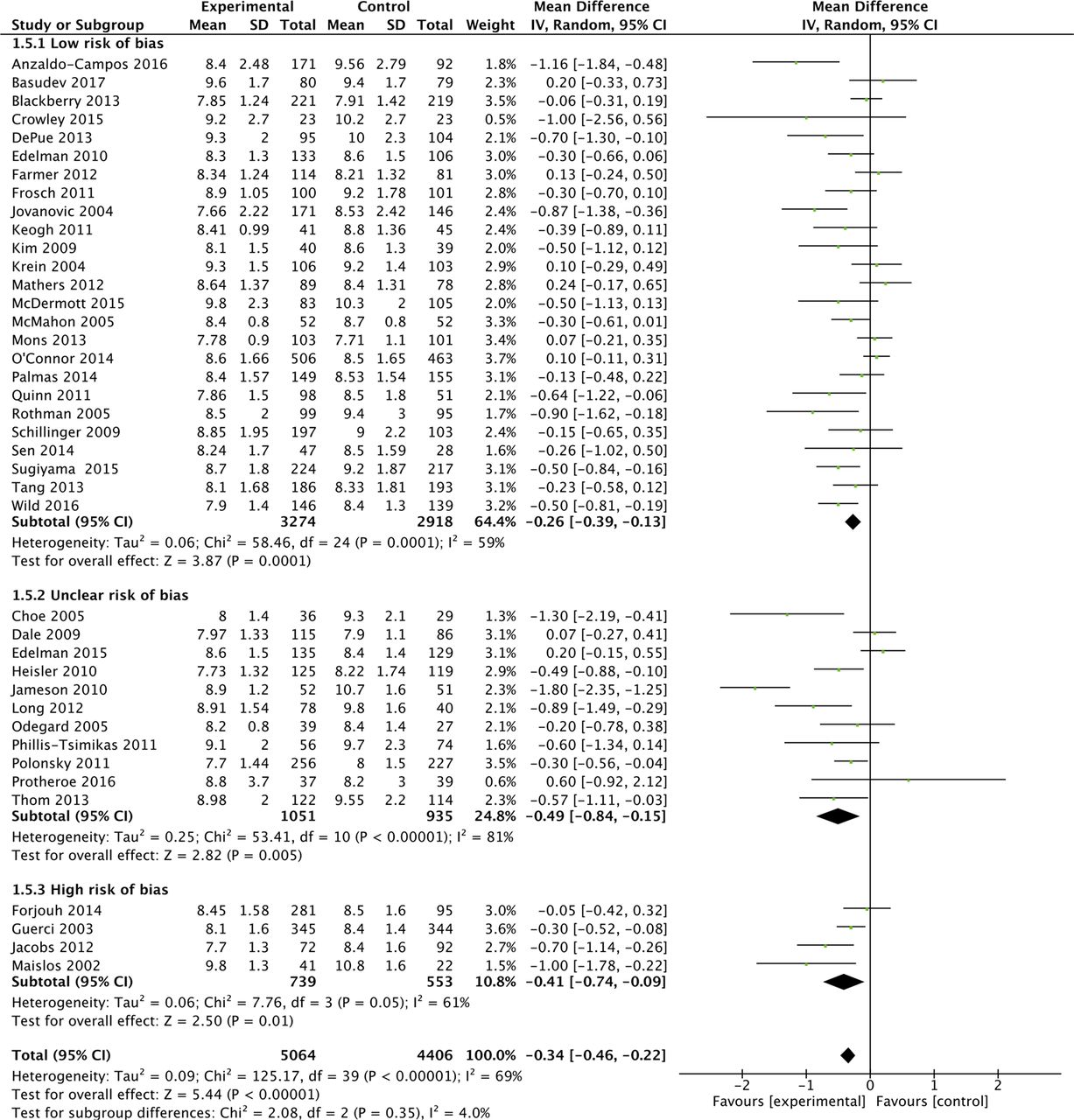
Overall 40 of the 42 studies were included in a meta-analysis, which found a MD in HbA1c of −3.7 mmol/mol (−0.34%; 95% CI −0.46% to −0.22%) favouring intervention groups, but with statistical heterogeneity (I2=69%). Figure 2A outlines the overall effect of interventions on HbA1c, across EPOC categories.

Effects of interventions on HbA1c, with intervention-type subgroups.
Subgroup analyses were performed based on the predominant intervention type (figure 2A), the baseline HbA1c level (figure 2B), study duration (figure 2C) and study quality (figure 2D).

Effects of interventions on HbA1c, with baseline HbA1c subgroup.

Effects of interventions on HbA1c, with baseline study duration subgroups.

{kind=link}
![[SP4.jpg]](https://bmjopen.bmj.com/content/bmjopen/7/8/e015135/DC4/embed/inline-supplementary-material-4.jpg?download=true){kind=link}
![[SP6.jpg]](https://bmjopen.bmj.com/content/bmjopen/7/8/e015135/DC6/embed/inline-supplementary-material-6.jpg?download=true){kind=link}
![[SP7.jpg]](https://bmjopen.bmj.com/content/bmjopen/7/8/e015135/DC7/embed/inline-supplementary-material-7.jpg?download=true){kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of interventions on HbA1c, with baseline study quality subgroup.
These analyses suggested that organisational interventions (MD in HbA1c of −5.2 mmol/mol (−0.42%; 95% CI −0.66% to −0.18%; I2=79%) had better improvements in HbA1c than patient-centred interventions (−0.30%; 95% CI −0.43% to −0.18%; I2=48%) (p=0.05). Similarly interventions performed when the baseline population-HbA1c was over 80 mmol/mol (9.5%) (MD in HbA1c of −6.3 mmol/mol (−0.58%; 95% CI −0.81% to −0.35%; I2=75%) had better improvements in HbA1c than populations with a baseline-HbA1c<9.5% (−0.17%%; 95% CI −0.29% to −0.05%%; I2=51%) (p=0.002). Study duration did not appear to affect HbA1c (figure 2C). Lastly, studies with a low-risk of bias (MD in HbA1c was −2.8 mmol/mol (−0.26%; 95% CI −0.39% to −0.13%; I2=59%) appeared to have a smaller reduction in HbA1c compared with unclear (−0.49%%; 95% CI −0.84%% to −0.15%; I2=81%) and high-risk studies (−0.41%; 95% CI −0.74% to −0.09%; I2=61%), but there was no evidence of a statistically significant difference (p=0.35). Though not considered in our original protocol, subgroup analysis did not highlight additional benefit from those interventions (included in both organisational and patient-centred intervention types), which had a telemedicine or mHealth component (see online supplementary appendix 7).33 36 45 52 56 59 65 68
supplementary appendix 7
![[SP8.jpg]](https://bmjopen.bmj.com/content/bmjopen/7/8/e015135/DC8/embed/inline-supplementary-material-8.jpg?download=true){kind=link}
As the overall results showed statistical heterogeneity, meta-regression analysis was also conducted to explore the components of this heterogeneity. As with the meta-analyses, higher baseline HbA1c was associated with a greater reduction in HbA1c (β-Coefficient: −0.27; 95% CI −0.41 to –0.13; p<0.001). The predominant-intervention type, risk of bias and study-duration were not associated with improved glycaemic control.
Blood pressure
Overall there was small improvement in SBP in the 26 interventions included in the meta-analysis, (MD SBP: –1.13 mm Hg (95% CI −2.19 to –0.08)) with moderate heterogeneity (I2=47%) (see online supplementary appendix 8).22–24 30–36 38 39 41 45 46 48–51 54 58–60 62 65 66 68 DBP improved modestly in the 22 studies included in the meta-analysis (MD DBP: –1.37 mm Hg (95% CI −2.25 to –0.50)) with moderate heterogeneity (I2=44%) (see online supplementary appendix 9).22–24 31 32 34–36 38 39 41 45 46 48 49 51 54 58 59 62 65 66 68
supplementary appendix 8
![[SP9.jpg]](https://bmjopen.bmj.com/content/bmjopen/7/8/e015135/DC9/embed/inline-supplementary-material-9.jpg?download=true){kind=link}
supplementary appendix 9
![[SP10.jpg]](https://bmjopen.bmj.com/content/bmjopen/7/8/e015135/DC10/embed/inline-supplementary-material-10.jpg?download=true){kind=link}
In the subgroup analysis, organisational interventions appeared to improve SBP modestly (MD SBP: –2.69 mm Hg; 95% CI −5.11 to –0.26; I2=57%) compared with patient-centred interventions (MD SBP: –0.52 mm Hg; 95% CI −1.41 to 0.38; I2=20%) which showed no statistically significant improvement (see online supplementary appendix 8). However, there was no evidence of a statistically significant difference between intervention types. Similarly with DBP, organisational interventions appeared to improve DBP modestly (MD DBP: −2.87 mm Hg; 95% CI −4.29 to –1.45; I2=30%) compared with patient-centred interventions (MD DBP: −1.37 mm Hg; 95% CI −1.42 to 0.2; I2=30%) (see online supplementary appendix 9) and there was evidence of a statistically significant difference (p=0.007). Meta-regression analysis was not conducted for SBP or DBP, as significant heterogeneity was not present on the overall effect sizes.
Lipids
Twenty of the 42 studies reported total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol or triacylglicerides.23 24 30–32 35 36 38 39 41 45 46 48 51 56 58 62 65 66 68 Statistically significant improvements in lipids were only demonstrated in 4 of these 20 studies.31 32 45 48 Baseline lipid levels were generally not reported. Eleven of the 20 studies reported data relating to total cholesterol. Meta-analysis was undertaken on these studies, which indicated a modest improvement in total cholesterol, favouring intervention groups (MD total cholesterol – 4.29 mg/dL (95% CI −7.68 to –0.89); I2=0%) (see online supplementary appendix 10).35 36 38 41 45 46 58 62 65 66 68
supplementary appendix 10
![[SP11.jpg]](https://bmjopen.bmj.com/content/bmjopen/7/8/e015135/DC11/embed/inline-supplementary-material-11.jpg?download=true){kind=link}
Secondary outcomes
All but 1 of the 42 included studies reported at least one of the eligible secondary outcomes (see online supplementary appendix 11). Overall, interventions had very limited effect on secondary outcomes. Twenty-six studies reported other physical outcomes (eg, body mass index (BMI) and estimated glomerular filtration rate). Of the 15 studies that reported on weight or BMI, only one showed significant improvement.56 Ten studies reported mental health outcomes36 38 41 45 58 59 64 with two showing a significant improvement in the Change Mental Component Summary Score and the Short Form-12 Mental Health Score.64 67 Twenty-eight studies reported PROMs, with 11 showing an improvement with the intervention. Ten studies reported medication adherence outcomes, with two showing improvement. Eighteen studies reported utilisation outcomes, with four improving processes of care.
supplementary appendix 11
Discussion
Statement of principle findings
Healthcare interventions have positive, although modest, effects on HbA1c in poorly controlled T2DM. Interventions targeting those with a higher baseline HbA1c (≥80 mmol/mol (9.5%)) show the greatest effects. There was also evidence of a modest impact on both blood pressure and lipids, though baseline control of these risk factors was generally good. Generally, little effect on secondary outcomes was found. Our results suggest that a targeted approach to T2DM management, focussing on individuals with very poor glycaemic control, may represent a prudent strategy for future management.
Strengths and weaknesses of the study
The methodology of our systematic review addresses key credibility issues.69 70 The research question was sensible, our search of the literature was exhaustive and our results are outlined clearly for primary and secondary outcomes. The effect of baseline HbA1c was consistent across studies, biologically plausible and was an a priori hypothesis.70
We performed meta-regression to explore the heterogeneity, which also confirmed the increased effectiveness of interventions on those with HbA1c ≥80 mmol/mol (9.5%). However, a major limitation is that meta-regression is usually underpowered to detect anything but very large associations. Meta-regression considers the interactions between trial level covariates and the treatment effect, but it inherits difficulties of interpretation attached to non-randomised studies, as it is not possible to randomise patients to one covariate value or another, so causality cannot be attached its findings.71 Though we do not believe the subgroup findings occurred by chance, there remained high heterogeneity and we explored between-study comparisons rather than within-study comparisons.70 There was some evidence of publication bias in the DBP analysis, but this was not present for the 22 studies reporting SBP. It should also be noted that the power of Egger's test is low when the number of studies is small and should only be used if the analysis includes a range of study sizes.
This study will inform researchers regarding the range of interventions that have been deployed to target patients with poorly controlled T2DM. There is no specific definition for ‘poor control’ of T2DM in the literature, but by including all studies that had patients with a HbA1c >59 mmol/mol (7.5%), we captured the full range of poor glycaemic control. Studies examining poor control of HbA1c possess a risk of regression towards the mean. However, all included studies were RCTs with control groups, which should have accounted for this. Targeted interventions in poorly controlled T2DM need to be distinguished from interventions, which are designed to intensively reduce HbA1c in all patients. Though persons with very poor glycaemic control are also at risk of the adverse effects of hypoglycaemic agents, targeting this population is more likely to reach the right balance of reducing harms of overtreatment and maximising potential benefits.18 The relative importance of targeting glycaemic or cardiovascular risk has been debated in the literature.17 We did not account for medication use in the studies, but given that all included studies were RCTs, which would balance out delivery of medications, we think that differences relating to underlying medication usage relate to how different interventions types promote the intensification of medications.
Comparison with other studies
The existing literature examining healthcare interventions to improve glycaemic control has focused on a range of approaches. There have been systematic reviews of interventions including QI initiatives, education, self-management support, case-management, adherence to medication and professional interventions, though as outlined previously, most have not specifically targeted patients with poor glycaemic control.8 10 11
A synthesis of 27 systematic reviews and 347 RCTs identified the cost-effectiveness of self-management interventions in T2DM in all patients with T2DM.72 This overview included studies that targeted all patients with T2DM and found very good evidence that education improves blood glucose control in patients with T2DM in the short term (less than 12 months) and that behavioural and psychological interventions are associated with modest improvements in blood glucose control (HbA1C).72 73 A review of computer-based diabetes self-management interventions to manage T2DM reported a small beneficial effect on blood glucose control (MD of −0.2%).74 Another recent systematic review of 118 self-management interventions found improvements in HbA1c in 62% of studies. The overall mean effect was to reduce HbA1c by −0.57%, although patients with persistently elevated HbA1c over 9 had greater improvements.75 In our review, patient-orientated interventions, such as self-monitoring of blood glucose and self-management interventions, seemed to be less effective than organisational interventions.
Case management by nurses and other professionals and case management in socially disadvantaged have been shown to be beneficial when targeted at all patients with T2DM and our review supports this conclusion for poorly controlled populations.5 76–78 Pharmacist-based interventions have been studied, mainly in outpatient settings or in US primary care and have been found to be effective and cost-effective.79 80 The five pharmacist interventions in our review, targeting patients with poorly controlled T2DM, showed mixed results, but overall had predominantly positive effects on HbA1c.
Attention to, and reporting of, intensification of antidiabetic medications and patient's adherence to treatment regimens are needed to achieve optimal glycaemic control.81 82 Evidence regarding adherence in T2DM is mixed. A previous systematic review of 21 studies that included 14 RCTs to enhance T2DM treatment adherence in community and hospital settings found that few studies measured or assessed adherence and that interventions to improve adherence did not show benefits or harms.83 A review by Farmer et al found limited evidence of effect for interventions promoting the monitoring of medication use and brief messaging to support medication adherence in patients with T2DM, though the included studies did not specifically target patients with poorly controlled diabetes.84 Only 10 of the 42 included studies in our review looked at adherence to medications as an outcome and only 2 of these 9 studies had a statistically significant effect on adherence.49 62 The baseline level of adherence varied considerably and studies used different scale ranges.
Our review identified only one professional-based interventions in poorly controlled T2DM, through a physician decision aid.42 Two systematic reviews have examined the impact of clinical decision support systems (CDSS) on the management of T2DM in primary care, between them looking at 28 trials, with varying results but none of these CDSS interventions were designed to promote intensification of prescribing in persons with poor glycaemic control.85 86
Future research
There is a need for further research examining professional-based interventions in poorly controlled T2DM, such as CDSS, which promote intensification of medications.81 Studies from jurisdictions outside North America on poorly controlled populations would also be welcome. An individual patient data meta-analysis would answer further questions not possible in this review and future research should attempt to obtain individual-level patient data. It is likely that most successful interventions have their impact as a result of intensification of medicines and/or improving adherence to medicines.81 As adherence was not measured in most of the studies and intensification poorly documented, it is important that future interventions report on these findings. Furthermore organisational interventions could incur significant costs to a health system, so cost-effectiveness analyses on future interventions should be undertaken to ensure the modest improvements in HbA1c are beneficial for the health systems.
In conclusion, clinicians and policy makers, when considering organisation of care for T2DM, should focus their effects on those patients with very poor glycaemic control (≥80 mmol/mol (9.5%)). Prioritising interventions that emphasise structured organisation of care, which can include intensification and adherence to medications, also seem more likely to deliver optimal results in terms of glycaemic control for T2DM patients.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
Footnotes
Contributors All authors contributed to the drafting of the paper. MEM and RG independently assessed studies for eligibility, extracted data and assessed study quality. Decisions or disagreements were brought to SMS. SMS, TF and FB provided methodological and statistical support to the paper.
Funding This work was supported by the HRB Centre for Primary Care Research (Research Grant: HRC-2014-1), a publicly funded body. Four of the six study authors are employed by this agency.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All collected data has been supplied as Supplementary Files. Please contact the corresponding author (MEM) if there are queries regarding this data.