Article Text

Abstract
Background High-risk human papillomaviruses (HPVs) cause all cervical cancer and the majority of vulvar, vaginal, anal, penile and oropharyngeal cancers. Although HPV is the most common sexually transmitted infection, public awareness of this is poor. In addition, many clinicians lack adequate knowledge or confidence to discuss sexual transmission and related sensitive issues. Complex science needs to be communicated in a clear, digestible, honest and salient way. Therefore, the aim of this study was to coproduce with patients who have cancer appropriate resources to guide these highly sensitive and difficult consultations.
Methods A matrix of evidence developed from a variety of sources, including a systematic review and telephone interviews with clinicians, supported the production of a draft list of approximately 100 potential educational messages. These were refined in face-to-face patient interviews using card-sorting techniques, and tested in cognitive debrief interviews to produce a ‘fast and frugal’ knowledge tool.
Results We developed three versions of a consultation guide, each comprising a clinician guidance sheet and patient information leaflet for gynaecological (cervical, vaginal, vulvar), anal or oropharyngeal cancers. That cancer could be caused by a sexually transmitted virus acquired many years previously was surprising to many and shocking to a few patients. However, they found the information clear, helpful and reassuring. Clinicians acknowledged a lack of confidence in explaining HPV, welcomed the clinician guidance sheets and considered printed information for patients particularly useful.
Conclusion Because of the ‘shock factor’, clinicians will need to approach the discussion of HPV with sensitivity and take individual needs and preferences into account, but we provide a novel, rigorously developed and tested resource which should have broad applicability in the UK National Health Service and other health systems.
- cervical cancer
- vaginal cancer
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
We provide a rigorously developed and tested resource comprising a brief and succinct guidance sheet to help doctors address their patients’ human papillomavirus (HPV) information needs and a more detailed information sheet for patients to take home.
This resource has been produced in partnership with patients and clinicians to provide information they wanted in a way that they found honest, accurate, reassuring and useful.
Due to its comparative rarity, we did not include patients with HPV-related penile cancer; therefore, we have no direct evidence that this resource would be equally suitable for these patients.
We have only limited evidence of acceptability to patients across all sexual orientations and ethnicities.
Introduction
Nearly all men and women are exposed to human papillomavirus (HPV) at some stage in their lives. Persistent infection with high-risk HPV types causes virtually all cervical cancer,1 most vulvar, vaginal2 and anal cancers,3 approximately half of penile cancers4 and over half of oropharyngeal (tonsil, base of tongue) cancers. In some instances, HPV status will determine the approach to cancer treatment.5 It also has a profound effect on prognosis in patients with oropharyngeal cancer.6 Health professionals must be prepared to discuss HPV status because affected patients may want to know the cause of their condition and may question the implications for their sexual partners. Although discussions about HPV between patients and health professionals are becoming more common in cervical disease, patients express concern about the stigma attached to sexual transmission.7–9 There is little rigorous research into how clinicians communicate with patients for other cancers associated with HPV.
Systematic reviews demonstrate consistently that women have poor knowledge of HPV and lack of awareness that it is a sexually transmitted causative factor for cervical cancer.10 11 Furthermore, women who are found to be HPV positive during cervical screening experience considerable distress and anxiety largely due to their lack of understanding of the commonness of HPV, and their tendency to view it in terms of other sexually transmitted infections (with associated stigma) or confuse it with HIV.11 Healthcare professionals often have difficulty initiating discussions about sexual matters with patients, and find it challenging to explain HPV infection; they describe it as a ‘can of worms’.12 To address stigma and psychosexual information needs, in addition to explaining the nature of HPV infection and the link between HPV and cancer, there is a clear need for new ‘fast and frugal’ knowledge tools for such sensitive, complex clinical consultations.13
A patient-centred approach has been proposed, but there is a lack of studies where patient input has informed education and counselling strategies.14 Written material, designed to inform and educate both healthcare professionals and patients, and thus improve health outcomes, has been used effectively to deliver patient-sensitive, evidence-based information about difficult scientific subjects.15 We intentionally included patient perspectives in a strategy designed to provide timely and accurate information on the role of HPV infection in cancer. Our methodological approach fitted with the Cochrane Consumers and Communication Review Group’s ‘The Knowledgeable Patient’,16 a summary of health benefits from improving patient and public/professional interactions by integrating systematic review evidence with patient and public views, as well as the co-production principle embedded in National Health Service Wales’ ‘Prudent Healthcare’.17 We also drew on the resources and recommendations for producing high-quality patient information outlined by the Patient Information Forum.18 19
Although there is quite a lot of publicly available information about HPV and cervical cancer, much of it focuses on cancer prevention (ie, HPV vaccination and HPV testing within cervical screening programmes), and there is much less information available about other cancer sites. Furthermore, while much of the relevant information is transferable across the cancers, some of it relates only to one cancer site. We aimed to develop and field-test evidence-based cancer site-specific versions of an HPV consultation guide, including ‘take-home’ information for patients diagnosed with HPV-related cancer. These guides were to contain the most salient points not to miss, rather than verbatim wording for a consultation, and were designed to reduce anxiety and increase knowledge about HPV in patients with specific cancers.
Methods
The methods for this study are described in detail in a protocol paper published during the data collection period20 and a schematic overview is presented in figure 1. In brief, consultation guides were developed in two stages and tested in a third.

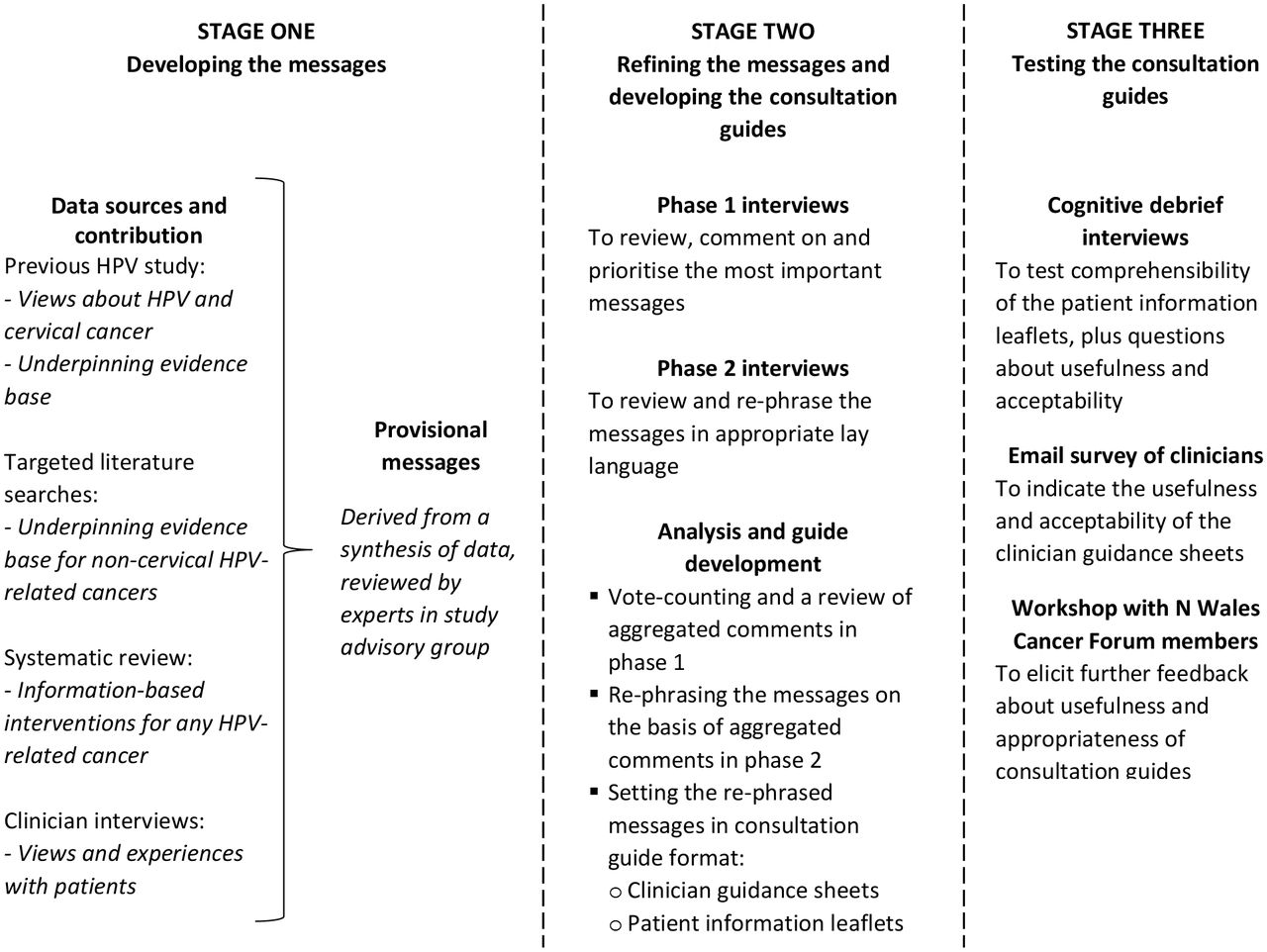{kind=link}
Overview of study methods.
First, a list of approximately 100 draft messages was generated based on a synthesis of findings from previous published and unpublished work relating to cervical cancer.21–23 This list was augmented by additional messages nominated by the study advisory group or resulting from targeted literature searches to address the remaining relevant cancers, a systematic review of information-based interventions for patients with HPV-related cancers, and telephone interviews with cancer clinicians. Data extracted from each of these sources were aggregated in a matrix of evidence (see online supplementary file 1) to support the draft messages. After a review of the evidence matrix by our study advisory group including specialists in each type of HPV-related cancer, HPV pathology and sexual health, the messages were either accepted verbatim, accepted with modifications or considered not sufficiently relevant or lacking in evidence, and deselected. Thus, a revised list of 32 provisional messages was developed. Since some messages were relevant only to specific cancers, three versions of the list were created to be appropriate for patients with gynaecological (cervical, vulvar, vaginal), anal or oropharyngeal cancers.
Stage 2 involved two phases of face-to-face exploratory interviews with patients diagnosed with gynaecological, anal or oropharyngeal cancers (penile cancer was not included because of the rarity of this disease and the difficulty in identifying suitable patients). In phase 1, the provisional messages were presented to participants in the format of statements printed on cards, and we drew on methods used in website design to sort and prioritise content.24–26 In phase 2, participants commented on the clarity of the selected messages, including specifics such as the tone and language used. Data comprising comments and suggestions from both phases were aggregated, summarised and reviewed, and the messages were modified accordingly. The research team structured the modified messages in a format consisting of one page of narrative information and one page of ‘frequently asked questions’ with answers to comprise three cancer-specific versions of the patient leaflet element of the consultation guide. These were reviewed by the study advisory group, chiefly to ensure the scientific accuracy of the information, revised and recirculated until final versions were agreed. Text from these versions was selected and formatted to provide the one-page clinician guidance element of the consultation guide. Thus, three cancer-specific versions of a consultation guide, each comprising a clinician guidance sheet and a patient information leaflet, were produced.
In stage 3, we adapted cognitive interviewing methods, using probing and ‘think aloud’ techniques to assess participants’ understanding of the patient leaflets.27 28 We also explored their views, reactions and feelings about the information they had received, for example, how they would use the information, whether they would share it and whether it made them feel differently about themselves. As additions to the protocol, we circulated the clinician guidance sheets by email to the clinicians who had participated in telephone interviews and asked them for feedback on their usefulness to patients and themselves. Finally, we presented our methods and findings to a group of cancer patients and carers from the North Wales Cancer Patient Forum and invited comments and discussion.
The study was granted UK NHS ethical approval. All patients recruited into the study were initially approached in private by the cancer clinician treating them during a consultation. They were given a verbal explanation of the study and supplied with a written information sheet and reply slip to take home. On receipt of the completed reply slip, they were contacted by a member of the research team to arrange an interview, which could be conducted in a private room in the university or hospital or in the participant’s own home, according to their preference. The interviewer sought confirmation that the participant had read and understood the information, and responded to any further questions, before obtaining written consent and commencing the interview.
Findings
Stage 1 findings: developing the provisional messages
Relevant findings from an earlier study conducted by members of this team, including published and unpublished work on HPV and cervical cancer prevention, were used to populate a matrix of evidence to support the draft messages as described in the methods section.21–23 Four studies were included in a new systematic review of information-based interventions for patients with HPV-related cancers. One qualitative study29 and one survey30 both investigated the informational and psychosocial needs of patients with oropharyngeal cancer. One study used audio-recorded data and a brief questionnaire to examine the content and quality of postcolposcopy consultations.31 Finally, one study used an intervention comprising a fact sheet developed from a review of available pamphlets, combined with a 40 min consultation with a nurse practitioner colposcopist, and compared compliance to postcolposcopy recommendations with a control group who did not receive the intervention.32 The review is fully reported in online supplementary file 2. Data from the included studies were added to the evidence matrix to inform message development. A number of additional articles were identified from targeted literature searches or by members of the study advisory group to fill evidence gaps in the matrix.
We attempted to identify and contact all the cancer clinicians working in Wales with the aim of interviewing a purposive sample of ~40 working across Wales and in varied clinical roles. Thirty-six clinicians, including oncologists, surgeons, clinical nurse specialists, colposcopists and speech and language therapists, took part in telephone interviews, which were audio-recorded. Data from the transcriptions were summarised and, together with illustrative quotations, entered into the matrix of evidence (see online supplementary file 1). While a few clinicians said that their patients never asked about HPV and so discussions never arose, this perception may have been related to their specific clinical role, that is, if patient encounters were confined to a point when the focus was on treatment and prognosis. Some indicated that they did not mention HPV to the patients because they considered it to be not relevant to disease management or not their role. However, many clinicians said that patients were becoming more aware of HPV, that some were doing their own research on the internet and that most asked what caused their cancer.
A minority of clinicians were completely comfortable with giving frank and open explanations (including the role of oral/anal sex in transmission, if applicable), clearly exercised tact and sensitivity and were conscious of the potential for partner problems and the possible need for privacy. They emphasised the normality and commonness of HPV infection, and were inclusive, using the word ‘we’, as in ‘we all get it’. They allayed concerns about fault and blame and made an effort not to be judgemental. However, many freely admitted to a lack of confidence in their own knowledge/ability to explain HPV to patients. A few commented about the need for training and the lack of available patient information. Several clearly found talking about sexual transmission embarrassing and confessed to being ‘out of their comfort zone’. Conversations about HPV were described as ‘awkward’, ‘a can of worms’ and ‘a minefield’. There was evidence of a degree of age and gender bias, with a perception that older patients were less likely to be interested in discussing HPV and more likely to be embarrassed, and that women were more likely to want to talk about it than men. Common ways of managing these difficulties were to give limited information and assume that if patients did not ask questions, they understood and were ‘OK with it’, or to allow the conversation to be ‘patient-led’, that is, not to mention HPV at all unless the patient raised it first. Some explained HPV as a virus but did not mention its mode of transmission, or referred to it obliquely, for example, ‘only women who have been sexually active get this’ or ‘it comes from a woman’s cervix’. Three interviewees reported having observed patients being upset by insensitively handled discussions, but there were also reports of patients being extremely relieved when their fears about infidelity or having ‘given their partner cancer’ were allayed.
After advisory group review and discussion of the completed evidence matrix, eight messages were deselected, leaving a list of 24 provisional messages comprising 15 generic messages, four applicable to oropharyngeal cancers, three to anal cancers and two to gynaecological cancers. Each message was underpinned by at least two different types of evidence and was considered by the advisory group to be useful and appropriate. Table 1 gives the list of messages and evidence sources; table 2 comprises an extract from the draft message evidence matrix (see online supplementary file 1) illustrating how each message was developed.
Provisional messages tested in phases 1 and 2 patient interviews, and sources of supporting evidence as described in the draft message evidence matrix
Extract from the draft message evidence matrix
Stage 2 findings: refining the provisional messages and developing the consultation guides
Characteristics of the participants in all stages of this study are described in table 3. In all, 59 people took part in face-to-face interviews to refine the provisional messages—30 in phase 1 interviews to prioritise and comment on the content of the messages and 29 in phase 2 interviews to comment on the language and tone of the messages and eliminate repetition. Most people knew very little about HPV, indeed many had never heard of it before being recruited to the study; a few confused it with HIV. Therefore, they were somewhat taken aback at the information that a virus could cause cancer, and that HPV is so common and easily passed on. Many were surprised, and a small minority quite shocked, to find that that their cancer might have been caused by a sexually transmitted infection, and especially that it could have been acquired many years ago, although for some this was a relief as it exonerated their current partner.
study participant characteristics
While most participants took this new information in their stride, several struggled to varying degrees with feelings of guilt and worry. A particular concern for a few was that they felt ‘dirty’, and two asked whether the transmission of HPV was associated with poor personal hygiene. Some felt stigmatised by having an infection that was sexually transmitted, even though they had had a very limited number of sexual partners. One woman asserted that ‘older people’ should not be told that HPV is sexually transmitted, ‘This is the most devastating thing for our age group’. Patients with anal cancer were especially likely to be embarrassed, but were reassured to have information that explained how HPV could be transmitted by intimate contact but not necessarily anal sex. To a lesser extent, patients with oropharyngeal cancer had similar concerns that people would assume they had engaged in oral sex. Indeed, these concerns proved to be well-founded in some instances by health professionals or acquaintances making comments to that effect. Nevertheless, the majority felt that ‘people should know’, and were reassured that ‘it was not their fault’. Questions that commonly arose and were not addressed by any of the messages were whether they were at risk of a further HPV-related cancer at a different site or whether their partner was at risk.
In phase 1, participants each selected five messages that were most important to them.The results of this prioritisation exercise are included in a summary analysis of the phase 1 and 2 interviews. This is provided in full in online supplementary file 3, of which an extract appears in table 4. There was a degree of consensus among the participants that pointed to a split into a high-scoring group of messages, which ≥15 out of 30 rated in their top 5, and a low-scoring group which ≤8 out of 30 rated in their top 5. Every message was rated in the top 5 at least twice, and many participants said that all the messages were important. Messages in the high-scoring group were related to the prevalence and natural history of HPV and cancer. Although participants often asked questions about the effects of HPV and cancer, particularly in terms of their possible impact on relationships, these messages were in the lower-scoring group.
Extract from the summary analysis of phase 1 and 2 interviews
Several participants pointed out repetition and overlap between the messages and that, as a consequence, sexual transmission was overemphasised, ‘another one about sex!’. Therefore, in phase 2, the cards were grouped in topic areas rather than presented one at a time, and participants considered how to eliminate repetition and whether, and how, to merge overlapping messages, as well as commenting on the content, language and tone. Suggestions for changes were noted (verbatim if specific rewording was suggested). Data relating to each message, from both phases of interviews, were summarised with relevant illustrative quotes. After review and discussion, the messages were rephrased to improve conciseness, comprehensibility and readability, and merged where necessary to eliminate repetition and overlap. The final list of messages for each cancer type, described in table 5, was reviewed by the advisory group.
Final list of messages incorporated in consultation guides
While retaining the newly developed phrasing of each of the resulting 10 generic and nine cancer-specific messages, they were organised into three versions of a new ‘consultation guide’ format. For each type of cancer (gynaecological, anal, oropharyngeal), a one-page clinician guidance sheet and a two-page patient information leaflet were created. To enhance comprehension and readability, we framed page 1 of the patient information leaflet (comprising the high-scoring messages) as a narrative and page 2 (comprising the lower-scoring messages) as ‘frequently asked questions’ with answers. For the clinician guidance sheet, we also selected a question and answer format: If your patient asks…, try saying…. as we considered this to be a more helpful, less directive format that might be more acceptable to clinicians.
Stage 3 findings: testing the consultation guides
Cognitive debrief interviews
Another 17 people with HPV-related cancers, recruited as before, took part in face-to-face cognitive debrief interviews. To assess comprehension, participants were asked to reflect back the meaning of the messages to the interviewer (‘what does this mean to you?), as well as what they thought about each message and how it made them feel. The majority of participants reported that they understood the content of the information sheet and found it informative, reassuring and interesting, and there was overall agreement on the comprehensibility, clarity and completeness of all the messages, ‘the message it’s intended to deliver has been delivered to me’. Therefore, although cognitive debrief interviews are often used to fine-tune wording, no further modifications were needed. As before, there was a degree of surprise or even shock; however, for most participants, being helped to understand that HPV was a common infection, was not their fault and they could not have prevented it was reassuring, ‘I might think about it more later, but I shan’t worry about it’.
Four of the participants who had been told about HPV outside the study context reported particularly upsetting experiences. They variously described: being referred to a sexual health clinic, being made to feel ‘dirty’ and ‘like a prostitute’, doctors insisting on HIV and chlamydia testing, being told that HPV infection was a result of ‘being unclean and having a lot of anal sex’ or simply not being looked at when the explanation was being given. In contrast, they found the information sheet reassuring, ‘It’s a shame the doctors didn’t speak to me like that’. Some participants felt that information should be more widely available. They reported that having an HPV-related cancer, as opposed to, say, breast cancer or bowel cancer, which are more commonly known and spoken about, could be very isolating. Some did not speak to anyone about their cancer, not just because they felt a degree of shame and stigma associated with it, but also because they did not know how to explain it and did not think others would understand; the information gave them the ability to talk: ‘knowledge is power’ said one.
There was no overall consensus on how information about HPV should be given to patients, that is, by whom, at what time point and in what circumstances. Some people thought nurses were best placed as they had more time and ‘might be more sensitive’; others thought it was a doctor’s responsibility ‘because they know more’. While some people wanted to have been told about HPV right from the beginning, many thought it was too much information to absorb at the time of diagnosis and would get lost among the plethora of information given at that time. Among those who tended to go accompanied to consultations, some thought it would be embarrassing to have a partner present, or were concerned about what they might think; others considered it ‘a journey you go through together’.
Most participants found the information useful and acceptable and although a small minority of participants were shocked by some of the content, all expressed approval of the manner in which the information was presented. They wanted information that was ‘straightforward and easy to understand’. Addressing repetition in the provisional messages meant that there was less emphasis on sexual transmission, with a result that the final versions appeared to be more reassuring. A summary of the stage 3 interview findings is available in online supplementary file 4.
Feedback from cancer clinicians on the clinician guidance sheets
Of the 36 clinicians who took part in telephone interviews in stage 1 of the study, 17 responded to an email request for feedback. We sent them the appropriate cancer-specific version of the clinician guidance sheet and asked them, on a scale of 1 to 5, how useful it was, how likely they were to use it in consultations and why. A few of the respondents commented but did not score the guidance sheets; 8 out of 12 who did gave a score of 4 or 5 for usefulness and 8 out of 13 gave a score of 4 or 5 for likelihood that they would use it. Those who scored the items lower than 4 gave one of two reasons: either that it was already part of their routine practice to talk to their patients about HPV , or that they would only give information to patients who asked about HPV, which rarely happened in their experience. Other comments were very positive; ‘useful’, ‘relevant’, ‘simple to understand’ and so on. Six respondents specifically mentioned that it would be particularly useful to have a written handout to give to patients, one thought the guidance sheet would be useful as a teaching aid and another commented that a useful addition would be signposting to further resources.
Discussion with North Wales Cancer Patient Forum
Five cancer patients and carers from the North Wales Cancer Patient Forum met with the research team and we presented the study methods and findings. After a lengthy discussion, the group reaffirmed our findings, saying that the information was very helpful. They expressed interest in how the consultation guides could be put into practice, and felt that this type of information should be disseminated more widely to raise awareness among the public.
Discussion
The product of this study is a suite of novel, coproduced consultation guides comprising clinician guidance sheets and patient information leaflets for HPV-related gynaecological, anal and oropharyngeal cancers. They were developed through a systematic process that included ensuring a robust evidence base and the scrutiny of experts at every stage. Crucially, they were coproduced and tested by cancer patients who, overall, found the resulting patient information leaflets to be interesting, accessible, informative and reassuring. In interviews, clinicians acknowledged a need for more education in the science relating to HPV and cancer and for training in communicating sensitive information to patients. Although slightly less than half of them responded to an email invitation to give feedback on the clinician guidance sheets, several mentioned a lack of patient information about HPV and three of them had written their own patient information leaflets to fill this gap. Representatives from the North Wales Cancer Patient Forum expressed enthusiastic support for the provision of information in general to patients and the public, and deemed the information we provided to be interesting, relevant, clear and easy to understand. All three versions of the clinician guidance sheets and patient information leaflets are available as supplementary files to download (see online supplementary files 5–10), and may be used under the terms of the Creative Commons Attribution License, which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
This was a mixed-methods study in which we creatively developed messages through an iterative process of lay and professional stakeholder coproduction using both primary qualitative, quantitative and secondary data collection and analysis methods. We took a pragmatic, iterative approach, borrowing and adapting techniques from a variety of sources and we used these methods together in a systematic and transparent manner, according to a peer-reviewed, published protocol.20 We recruited male and female participants with a range of ages and spread across the cancer sites. We aimed for a sample with a range of socio-economic backgrounds by means of recruiting from diverse geographical areas across North and South Wales, and a range of understanding based on a health literacy question, ‘How often do you need to have someone help you when you read instructions, pamphlets, or other written material from your doctor or pharmacy?’33; however, our sample was not ethnically diverse. Therefore, we can only make limited comments about the usefulness or acceptability of the consultation guides among minority populations. One woman was extremely shocked by the information because the discussion of any matters relating to sex was taboo in her community. We did not ask participants about their sexual orientation, but one who volunteered that they were in a same-sex relationship said that our information was perfectly acceptable, ‘the offensive bit can come from doctors not knowing what to say…’
To our knowledge, this was the first study to develop educational resources for both clinicians and patients, for three types of HPV-related cancers, that were both evidence-based and coproduced by patients. Several authors have documented the need for patients to be informed and counselled about HPV,29 34 35 and that physicians lack the ability to do so for want of adequate knowledge34 36 or because of discomfort in talking about sexual matters.37 Some have identified questions that patients might ask and offered suggestions for explanations that might be given.14 34 38 We drew heavily on the work of these and other authors to build the evidence base for our draft messages. However, the available literature was overwhelmingly related to cervical or oropharyngeal cancers only and patients were not directly engaged in the production of educational resources.
We did not attempt to recruit patients with penile cancer because this is a relatively rare condition; however, there is no obvious reason why an appropriately modified version of the consultation guide would not be acceptable to them. The opinions of participants were divided with respect to the appropriate timing of introducing information about HPV, and whether it should be given privately or in the presence of a spouse or other companion. Although we provide a resource that will help clinicians to navigate these difficult consultations, they will still need to approach the discussion of HPV with sensitivity and take individual needs and preferences into account.
These materials have the potential for wide dissemination and reach as the content has high provenance and is likely to be widely acceptable in the UK and other English-speaking countries. Potential formats include written or computerised prompts and web-based patient or clinician resources. Further research should consider which methods are most likely to ensure successful implementation and the degree to which the messages serve the needs of patient populations more diverse than those who contributed to the current version. As scientific understanding progresses, there will also be a need to review the validity of the messages and determine whether updates will be required.
References
Footnotes
Contributors CW is Chief Investigator and conceived the original idea for the research. MH, DP, RA, ME, AF, MR, CC and MM were co-applicants and together with CW designed the study. JH and SN developed participant recruitment materials and sought ethical and R&D approval. All authors regularly attended meetings of the study advisory group and contributed to further development of the protocol. JR represented the patient perspective; OW advised on sexual health; MS advised on virology/pathology of HPV. RA, ME, AF and SG were involved in patient recruitment. MH and DP conducted the systematic review; JH and MH conducted telephone interviews with clinicians; MH and M-JB conducted face-to-face patient interviews. MH and DP drafted the paper; all authors read, commented and were involved in subsequent redrafts and all have read and approved the final version.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval NHS Health Research Authority, Wales REC 3.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement We have attempted to make all relevant data available, either within this manuscript or in the supplementary files; however, we welcome further inquiries to the corresponding author.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected theseerrors and the correct publishers have been inserted into the references.