Article Text

Abstract
Introduction The incidence and mortality rates of cutaneous melanoma (CM) are increasing among fair-skinned populations worldwide. Ultraviolet radiation (UVR) is the principal risk factor for CM, but is also the main source of 25-hydroxyvitamin D (25(OH)D), which has been associated with reduced risk and better prognosis of some cancer types. However, both low and high 25(OH)D levels have been associated with increased risk of CM. Obesity as measured by body mass index (BMI) is associated with risk of several cancers and has also been suggested as a risk factor for CM, and may also be related to insufficient 25(OH)D and/or high leptin levels. Moreover, contracting a CM diagnosis has been associated with increased risk of developing second cancer. We aim to study whether low prediagnostic serum levels of 25(OH)D, high prediagnostic levels of BMI and high serum leptin levels influence CM incidence, Breslow thickness and CM mortality, and risk of second cancer and survival after a CM diagnosis.
Methods and analysis Cohort and nested case–control studies will be carried out using the population-based Janus Serum Bank Cohort (archival prediagnostic sera, BMI, smoking and physical activity), with follow-up from 1972 to 2014. Additional data will be received from the Cancer Registry of Norway, the national Cause of Death Registry, Statistics Norway (education and occupation) and exposure matrices of UVR. Time-to-event regression models will be used to analyse the cohort data, while the nested case–control studies will be analysed by conditional logistic regression. A multilevel approach will be applied when incorporating group-level data.
Ethics and dissemination The project is approved by the Regional Committee for Medical Research Ethics and is funded by the Norwegian Cancer Society. Results will be published in peer-reviewed journals, at scientific conferences and in the news media.
- Vitamin D
- 25-hydroxyvitamin D
- leptin
- serum samples
- Obesity
- body mass index
- ultraviolet radiation
- melanoma
- incidence
- mortality
- second cancer
- survival
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Vitamin D
- 25-hydroxyvitamin D
- leptin
- serum samples
- Obesity
- body mass index
- ultraviolet radiation
- melanoma
- incidence
- mortality
- second cancer
- survival
Strengths and limitations of this study
Linkage of independent, national data sources by use of a unique personal identification number for a comprehensive research file and complete control of loss to follow-up.
Prediagnostic serum samples assuring a true prospective relationship between exposures and cancer, limiting bias introduced by reverse causality.
Lifetime ambient ultraviolet radiation (UVR) exposure data (UVA, UVB and erythemally weighted UV) and group-level data on sunburns, sunbathing vacations and solarium use capturing variations in age, time period and county of residence.
Ambient UVR exposure and data on sunburns, sunbathing vacations and solarium use can only be linked to the Janus Cohort on a group level.
Lack of data on pigmentary characteristics and naevi.
Introduction
Rationale and evidence gaps
Ultraviolet radiation (UVR) is a recognised human carcinogen and the principal environmental risk factor for cutaneous melanoma (CM),1 2 while skin characteristics such as skin sensitivity and number of naevi indicate CM susceptibility.3–7 CM incidence and mortality rates have been increasing in fair-skinned populations worldwide the past decades, and CM is currently the third most common cancer in Europe after cancers of the colon/rectum and the lung.8 9 In Norway, CM incidence has increased more than 3% annually between 1982 and 2011 and has been projected to continue to rise.9 Excess UVR exposure is likely the major cause of this increase,10 but also low vitamin D levels and obesity have been suggested to play a role.11 12
Vitamin D synthesis in the skin is initiated by UVR exposure to the skin surface at wavelengths of 290–320 nm, which converts 7-dehydrocholesterol in the keratinocytes to previtamin D3 (cholecalciferol). Together with previtamin D2 (ergocalciferol), previtamin D3 may also be obtained by diet. Both previtamin D2 and D3 are then hydroxylated in the liver to 25-hydroxyvitamin D (25(OH)D), which represents the circulating storage form of vitamin D. A second hydroxylation in the kidney converts vitamin D to its biologically active form 1, 25-hydroxyvitamin D (1, 25(OH)D),13 14 which has been associated with anticancer mechanisms.13 15–17 Based on four studies, a recent meta-analysis reported a summary relative risk of CM of 1.46 (95% CI: 0.60 to 3.53) for the highest compared with the lowest (reference) quantile of 25(OH)D.12 In three of these studies, risks increased with increasing 25(OH)D serum levels, while the fourth study reported the opposite.18–21 None of these studies individually showed any statistically significant associations, and the inconclusive results may be due to difference in statistical power, the covariate adjustments, whether CM cases had a cancer history or not, and whether serum was sampled before or after the CM diagnosis. Several recent studies have reported an inverse association between Breslow thickness and 25(OH)D serum level at diagnosis.20 22–25 As both tumour thickness and 25(OH)D level were measured at the same time in these studies, these associations may have been affected by reverse causality.26 27 However, for prognosis after a CM diagnosis, higher diagnostic 25(OH)D levels have been shown to predict lower risk of relapse and increased survival, independent of Breslow thickness.22 24 A recent study ascribed the effect on CM survival to change in 25(OH)D during follow-up from CM diagnosis to death, and not the 25(OH)D level at diagnosis.28
Low 25(OH)D levels are more frequent in obese persons, suggesting that 25(OH)D deficiency is associated with obesity and vice versa.29–33 Obesity as measured by body mass index (BMI) above 30 kg/m2 has been positively associated with CM risk in males, but results for women are ambiguous and possibly confounded by personal habits as obese women may refrain from sunseeking behaviour compared with their normal-weight peers.11 Further, diet-induced obesity has been found to increase CM progression in mice models.34 The biological mechanism underlying an obesity-induced increase in CM incidence is not well understood, although a hyperglycaemia hypothesis has been suggested.35 Another hypothesis suggests that adipocytes produce high levels of vascular endothelial growth factor, associated with visceral fat, which contributes to angiogenesis and tumour growth.36
The metabolic hormone leptin may be a risk factor for both CM and CM progression. Leptin is released by adipose tissue and plays an important role in the regulation of insulin sensitivity and weight regulation.37 38 Increased diagnostic serum levels of leptin have been associated with increased CM risk, possibly caused by a leptin-induced increase in neoangiogenesis, reduction of melanogenesis and a decreased capacity of the melanocytes’ DNA repair.39 40 Recent studies have demonstrated that leptin receptors are present in melanoma cell lines that proliferate in response to leptin, and that leptin bound to its receptor stimulates melanoma growth.41–44
After a CM diagnosis, there is an increased risk of diagnosis of additional CM, as well as other cancers.45 46 For example, the risk of lymphoma before or after CM has received increased focus.47 Immune perturbation has been suggested to contribute to the development of CM after non-Hodgkin’s lymphoma (NHL) subtypes such as chronic lymphocytic leukaemia/small lymphocytic lymphoma.48 As for CM, low 25(OH)D serum levels have also been associated with reduced survival and poor prognosis after NHL,49 50 which raises the question of whether low 25(OH)D could alter the risk of lymphoma as a second cancer after CM or vice versa.
Aims and hypotheses
The interplay between 25(OH)D and obesity and their relation to CM is poorly described, and increased knowledge of these factors is warranted to improve CM prevention and prognosis. In the present study protocol, we propose a set of prospective cohort and nested case–control studies with the primary aim of examining BMI and serum levels of 25(OH)D and leptin in relation to CM risk, Breslow thickness and mortality, and risk of second cancer and survival after a CM diagnosis. As a secondary aim, we propose a nested case–control study of lymphoma risk after CM and vice versa, in relation to serum levels of 25(OH)D and leptin.
We hypothesise that:
High prediagostic BMI (≥30 kg/m2, quantiles, continuous) is associated with
Increased CM risk, Breslow thickness and mortality;
Reduced survival after a CM diagnosis;
Increased risk of contracting CM followed by a second cancer (n=292 851);
Increased risk of second cancer among CM survivors (n ≈ 3000).
High prediagnostic serum levels of leptin (>4 ng/mL, highest quantile, continuous) and low prediagnostic 25(OH)D levels (<30 nmol/L, lowest quantile, continuous) are associated with
Increased CM risk and Breslow thickness;
Reduced survival after a CM diagnosis;
Increased risk of contracting CM followed by a second cancer compared with no cancer history;
Increased risk of second cancer among CM survivors;
Increased lymphoma risk after a CM diagnosis and vice versa compared with no cancer history.
Methods and analysis
Study population and data sources
Janus Serum Bank Cohort
This project is based on the Janus Serum Bank Cohort, a population-based biobank for prospective cancer studies containing serum samples and questionnaire data from 292 851 Norwegians who participated in five health surveys 1972–2003. A detailed description of the Janus Serum Bank Cohort (hereafter Janus Cohort), its data and establishment, is published elsewhere.51 The Janus Cohort includes participants from the following surveys:
The Oslo Study I (1972–1973) invited men residing in Oslo aged 20–49 years.
The Norwegian Counties Study was carried out as a three-wave survey (1974–1978, 1977–1983 and 1985–1988), inviting men and women aged 20–49 years residing in Finnmark, Oppland or Sogn og Fjordane.
Oslo Age 40 Programme invited men and women aged 40 residing in Oslo 1981–1999.
The National Age 40 Programme triennially invited all men and women aged 40–42 years in all Norwegian counties during 1985–1999.
The TROFINN Health Study invited all men and women aged 30–75 years residing in Troms and Finnmark in 2001–2003.
Blood serum samples
The Janus Cohort has detailed sample information including date of sample collection and county of residence at sample collection. The samples have been stored at –25°C for up to 43 years.51 Serum samples of 25(OH)D and leptin have been demonstrated to have high stability after long-term storage,52 53 and previous studies have shown that serum from the Janus Cohort is well suited for analyses of 25(OH)D54 55 and leptin.56 57 Although the storage condition at −25°C is not ideal, a possible time-dependent degradation may be partly compensated for by matching cases and controls on time of blood draw.
Height and weight measurements and questionnaire data
Together with blood sample collection, standardised height and weight measurements were taken by trained personnel. Participants in the surveys were also asked to complete questionnaires on smoking habits, alcohol consumption, diet, physical activity, use of medications etc. Slightly different questionnaires (different wording and number of response categories) were used in the five health surveys, and a set of variables has been harmonised.58 For the present project, the following variables are available: height (cm), weight (kg), BMI (kg/m2 and categorised as 12–18.49, 18.5–24.9, 25.0–29.9, ≥30),59 smoking status (never, former, current), cigarettes per day (1–9, 10–14, ≥15), years of smoking (1–9, 10–29, ≥30), time since smoking cessation (<3 months, 3 months–1 year, 1–5 years, >5 years), level of total physical activity (inactive, low, medium, high) and level of physical activity at work (sedentary, walking, walking and lifting, heavy physical work).
Linking the Janus Cohort to population-based registries
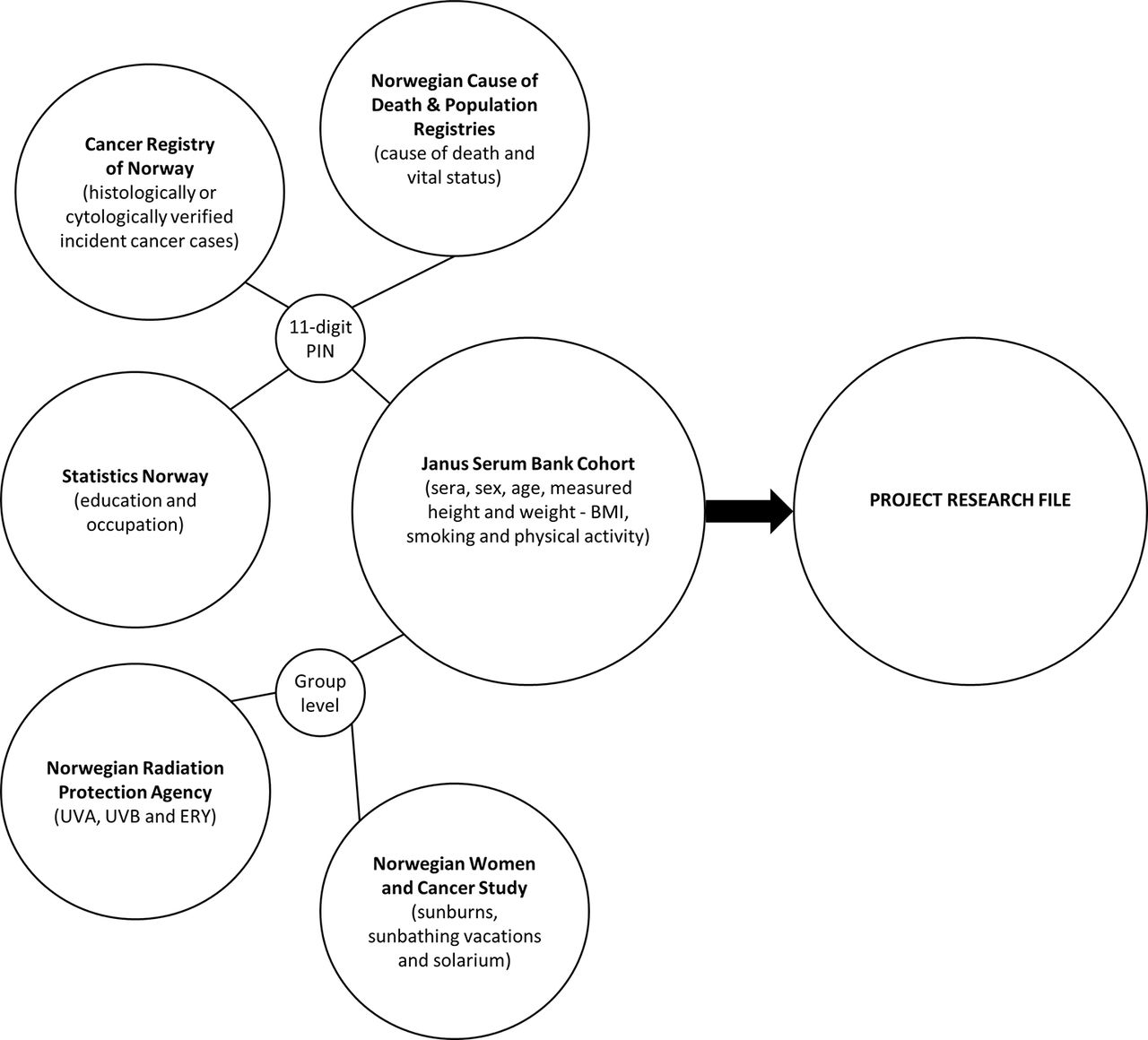
Every resident in Norway is assigned a unique 11-digit personal identification number (PIN), which ensures a correct linkage of the Janus Cohort to population-based registries and databases as described below and in figure 1.

Overview of linkage between different data sources. BMI, body mass index; ERY, erythemally weighted UVR; PIN, personal identification number; UVR, ultraviolet radiation.
Population-based registries
The Cancer Registry of Norway (CRN) has registered all new cancer diagnoses in Norway since 1953. Reporting of incident cancers to the CRN is compulsory by law, and information from pathologists, general practitioners, the Norwegian Patient Registry and the Norwegian Cause of Death Registry ensures a high degree of completeness (overall 98.8%).3 For the present project, incident cancers from 1972 through 2014 will be linked to the Janus Cohort. The following cancer information will be used: date of diagnosis (month and year), tumour localisation (International Classification of Diseases seventh revision (ICD-7 codes) converted into ICD-10 codes), histology (codes from ICD-Oncology second and third revisions), clinical stage (local=no metastases, regional=metastasis in regional lymph nodes or surrounding area, distant=distant metastasis) and Breslow thickness (mm).
Date and cause of death (death from cancer and death from causes other than cancer) will be obtained from the Cause of Death Registry and vital status (alive, emigrated or dead) with corresponding dates will be obtained from the National Population Registry.
Data on occupation at baseline (categorised as indoor/outdoor/mixed and high risk/medium risk/low risk for UVR exposure) and highest attained educational level at baseline (none, compulsory, upper secondary, college/university) will be obtained from Statistics Norway.
UVR exposure matrices
County-specific, yearly average doses of ultraviolet A (UVA), ultraviolet B (UVB) and erythemally weighted UVR (ERY) will be calculated and assigned to each participant, according to place of residence, at baseline and cumulated throughout follow-up (ie, until cancer, emigration, death or 31 December 2014, whichever occurs first). The UVR exposure matrices will be based on measurement data from UV-network stations operated by the Norwegian Radiation Protection Authority and on modelled values as described by Medhaug et al.60 Furthermore, age-specific, county-specific and time period-specific data on sunburns, sunbathing vacations and solarium (women only) use will be linked to the Janus Cohort on a group level as derived from questionnaire data collected in the Norwegian Women and Cancer study.61 62 Surveys conducted by the Norwegian Cancer Society show small gender differences with respect to frequency of sunburns and sunbathing vacations among Norwegian women and men.63 This is also supported by almost identical CM incidence rates between men and women in Norway in the past 60 years.64
Study designs
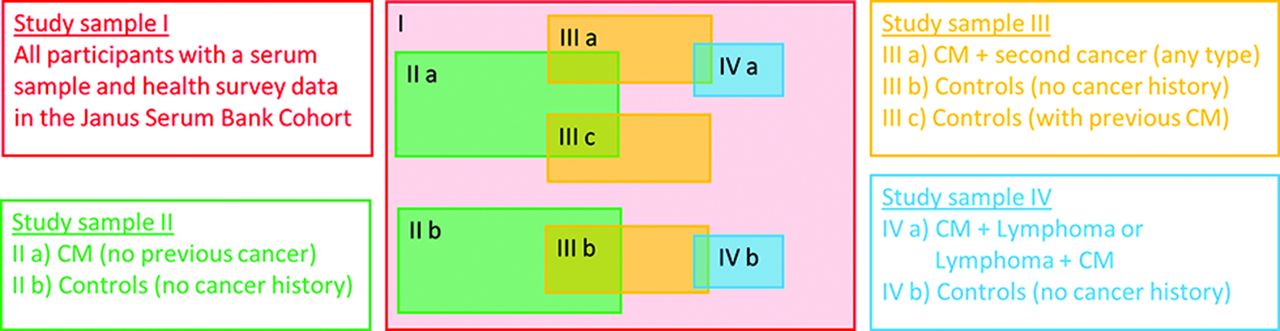
Study I: a prospective cohort study
In a prospective cohort study among all 292 851 individuals in the Janus Cohort (study sample I in figure 2), we will explore baseline BMI in relation to CM risk, Breslow thickness and mortality (hypothesis 1.1), survival after a CM diagnosis (hypothesis 1.2) and risk of second cancer after CM (hypotheses 1.3 and 1.4). Hypotheses 1.3 and 1.4 differ by use of study sample; hypothesis 1.3 includes all 292 851 individuals in the Janus Cohort, while hypothesis 1.4 includes only the 3000 CM cases. Sex-specific analyses exploring the potential confounding effects from age, UVR exposure, smoking and education will be conducted for all analyses in study I.
{kind=link}
{kind=link}
Overview of study samples and overlap between cases and controls between studies.
Studies II–IV: prospective nested case–control studies
Three prospective case–control studies will be nested within the Janus Cohort (study samples II–IV in figure 2). For serum analyses, the nested case–control design is cost-efficient compared with the cohort design as only a limited number of CM cases and cancer-free controls are selected and matched using an incidence-density sampling scheme.65 Also, the nested case–control design takes advantage of the prospective nature of the cohort study by using data and serum samples collected before any cancer diagnosis, thereby reducing the potential for bias. Table 1 gives a complete description of the case, control and matching criteria.
Overview of case, control and matching criteria for studies II–IV
Study II
Study II will examine CM risk and Breslow thickness according to prediagnostic serum levels of 25(OH)D and leptin (hypothesis 2.1). We will study CM cases (II a; figure 2) without a history of cancer and controls alive and without a cancer history at the time of the case diagnosis (II b). We will include one control per case, matched on sex, age at serum sampling and season due to seasonal variation in 25(OH)D levels (table 1). UVR exposure, smoking and education will be adjusted for. Survival analysis (as in study I) will be undertaken on the subsample of CM cases (II a) with measured 25(OH)D and leptin (hypothesis 2.2). Covariates included in study I will be taken into account.
Study III
In study III, we will examine the risk of second cancer after a CM diagnosis according to prediagnostic serum levels of 25(OH)D and leptin (hypotheses 2.3 and 2.4). CM cases with a second cancer (III a; figure 2) and controls without a cancer history at the time of the second cancer diagnosis (III b) will be selected to address hypothesis 2.3. For hypothesis 2.4, controls with a CM diagnosis at the time of the second cancer diagnosis will be selected (III c). We will include one control per case, matched on sex, age at serum sampling and season of serum sampling (table 1). In addition, control group III c will be matched on date of the CM diagnosis (table 1). Covariates included in studies I–II will be taken into account.
Study IV
A group including cases (IV a; figure 2) with CM before lymphoma or vice versa and controls (IV b) with no cancer history at the time of the second cancer diagnosis will be examined according to prediagnostic serum levels of 25(OH)D and leptin (hypothesis 2.5). All case–control pairs will be matched on sex, age at serum sampling and season of serum sampling (table 1). Covariates included in studies I–III will be taken into account.
Power and sample size calculations
Study I
With the large study sample (n=292 851), including more than 3000 CM cases by 31 December 2014, we have sufficient statistical power to reveal minor risk differences between the BMI categories, normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2) and obese (≥30 kg/m2). Thus, further power calculation is not conducted.
Studies II–IV
Study II will include 700 CM cases of the approximately 3000 available. Study III will include 345 cases with a second primary cancer after CM and study IV will include 60 cases of lymphoma after CM or vice versa, which were the total number of cases in the Janus Cohort by 31 December 2014. Table 2 shows the smallest detectable OR according to assumed proportion of controls exposed to low serum levels of 25(OH)D and high leptin levels when using a power of 0.80 and a significance level of 0.05. The assumed proportions of exposed controls were based on previous studies conducted on serum samples from the Janus Cohort. For 25(OH)D, a study on prostate cancer reported that 4.4% and 30.6% of the controls had 25(OH)D levels below 30 nmol/L and 50 nmol/L, respectively.54 For leptin, a study on colon cancer reported that 20% of the controls had a leptin level of 4.1 ng/mL or higher.56
Smallest detectable OR (above the null) according to proportion of controls exposed to low vitamin D (25(OH)D) and high leptin levels, using a power of 0.80 and a significance level of 0.05
Data management
Case–control selection
As indicated in figure 2, there will be some overlap between cases and controls between the studies. CM cases (II a) will be sampled at random from all available CM cases in the Janus Cohort, independent of second cancer status. However, some of the CM cases (II a) may have developed a new cancer and then be eligible for use in study III as CMs with a second cancer (III a). Controls (II b) will be sampled at random with replacement (incidence-density sampling) from the Janus Cohort and matched to CM cases (II a). Also, controls (II b) matched to the CM cases (II a) who developed a second cancer (III a) will be eligible for use in study III (group III b) if they are alive, resident and cancer-free at the time of the CM cases’ second cancer (III a). Cases from study II (II a) may be reused as controls in study III (III c) if they fulfil the matching criteria (table 1). The remaining case–control pairs for study III will be sampled from the Janus Cohort. Study IV will follow the same approach as studies II and III with respect to reuse. A picking list of unique serum samples for all studies will be prepared by a data manager for the Janus Serum Bank Cohort laboratory team.
Laboratory analyses
The Janus Serum Bank laboratory team will send 220 µL aliquots of serum to the Hormone Laboratory at Oslo University Hospital for analyses of 25(OH)D and leptin. The laboratory participated in the Vitamin D External Quality Assessment Scheme for total 25(OH)D. The Hormone Laboratory is accredited by the Norwegian Accreditation as a testing laboratory and complies with the requirements of the NS-EN ISO/IEC 17025 standards.
Serum concentrations of 25(OH)D will be determined by an in-house developed liquid chromatography/tandem mass spectrometry method. In brief, after protein precipitation, 25(OH)D will be extracted from samples using phospholipid depletion plates. Separation is achieved by reversed-phase chromatography and the isobaric C3 epimer 3-epi-25(OH)D3 will be separated from 25(OH)D3. Mass spectrometric detection will be performed by electrospray ionisation and triple quadruple ion separation (multiple reaction monitoring).66 Serum concentrations of leptin will be determined by using EMD Millipore Human Leptin Radioimmunoassay as described in Lee et al.67
Hormone Laboratory staff will be blinded to case–control status. Two identical quality control (QC) samples with serum from a pool of several persons will be placed on each batch. These two QC samples will change position for each new batch to avoid bias from weak spots in the machine/kit and will thus take into account both inter-batch variability and intra-batch variability. Each case–control pair will be placed and analysed on the same batch.
Statistical methods
In the cohort studies, we will use Poisson and Cox regression and estimate relative risks with 95% CIs. Spline models will also be explored if a non-linear relationship between exposure and outcome is assumed. In the nested case–control studies, conditional logistic regression will be applied to estimate ORs with 95% CIs. A multilevel approach will be applied for analyses containing group-level data. Directed acyclic graphs will be used in the process to select variables to include in the statistical models. Confounding variables will be included in the models and tests of interaction effects will be performed when relevant. In the case of interaction effects, stratified results will be presented. All tests will be two-sided and p<0.05 will be considered statistically significant. All statistical analyses will be performed using Stata.
Analysis plan
We plan to conduct the following analyses to test our hypotheses:
Hypothesis 1.1: A prospective cohort analysis of prediagnostic BMI and other anthropometric measures in relation to CM risk, Breslow thickness and mortality using the complete Janus Cohort (n=292 851).
Hypothesis 1.2: A prospective analysis of survival after a CM diagnosis, according to prediagnostic BMI (n ≈ 3000).
Hypothesis 1.3: A prospective cohort analysis of prediagnostic BMI and the risk of second cancer after a CM diagnosis using the complete Janus Cohort (n=292 851).
Hypothesis 1.4: A prospective cohort analysis of prediagnostic BMI and the risk of second cancer among CM survivors (n ≈ 3000).
Hypothesis 2.1: A nested case–control analysis of CM risk and Breslow thickness according to prediagnostic serum levels of 25(OH)D and leptin in 700 pairs.
Hypothesis 2.2: A prospective analysis of survival after a CM diagnosis (n=700) according to prediagnostic serum levels of 25(OH)D and leptin.
Hypothesis 2.3: A nested case–control analysis of risk of second cancer after a CM diagnosis according to prediagnostic serum levels of 25(OH)D and leptin. Using 345 pairs of cases with CM + a second cancer and controls without a cancer history.
Hypothesis 2.4: A nested case–control analysis of risk of second cancer among CM survivors according to prediagnostic serum levels of 25(OH)D and leptin. Using 345 pairs of cases with CM + a second cancer and controls with a CM diagnosis.
Hypothesis 2.5: A nested case–control analysis investigating risk of lymphoma after CM or vice versa according to prediagnostic serum levels of 25(OH)D (n=60 cases) compared with controls without a cancer history.
Project strengths and limitations
A major strength of the project is the linkage of multiple data sources by use of the PIN, thereby establishing a comprehensive research file with independently and prospectively collected data, and a complete control of loss to follow-up. An important strength is also the use of high-quality cancer data with over 3000 CM cases from a population-based registry relying on compulsory reporting of incident cancers. Further, the prediagnostic serum samples assure a clear prospective temporal relationship between exposure and cancer, which limits the possibility of reverse causality, that is, that the cancer or its precursor affects the 25(OH)D or leptin serum levels.
An important limitation of the project is that we will only be able to obtain group-level data on UVR exposure (ambient UVA, UVB and ERY; sunburns, sunbathing vacations and solarium use), but our data will capture variation in these variables by age, time period and between counties. However, the long and complete time series, covering the whole observation period and early childhood for many of the participants, enables analysis with time-varying UVR exposure. Another limitation is the lack of data on pigmentary characteristics and number of naevi. Also, differences in skin colour between cases and controls could potentially bias our estimates. However, the average fraction of non-whites during 1970–1991 (when 97% of the Janus Cohort was established) was less than 1% of the total Norwegian population,68 and hence we consider the risk of introducing bias by not taking individual information on skin colour into account as negligible.
Ethics and dissemination
The project has a running approval from the Regional Committee for Medical and Health Research Ethics to link the different population-based registries to establish a deidentified research file. In addition, each registry and data source has approved that its data will be linked and used in a deidentified research file. A linkage key consisting of the 11-digit PIN and a project-specific ID number will be stored and governed by a third party unavailable to the research team. Moreover, participation in each of the health surveys constituting the Janus Cohort was voluntary and based on informed consent.
All results will be published in relevant peer-reviewed international scientific journals and presented at conferences, nationally and internationally. Results will also be directly communicated to user groups such as the Norwegian Cancer Society, The Norwegian Melanoma Association, and to health authorities and clinicians. Both the annual Norwegian conferences (‘Oncologic Forum’, the Norwegian Melanoma Group Meeting) and international conferences will serve as platforms for knowledge distribution to clinicians and researchers. Important results will also be disseminated through press releases. Further, lectures, the CRN website, social media and other potential channels will also be used to reach patient organisations, patients and the general public.
Acknowledgments
The authors thank Hilde Langseth, Marianne Lauritzen, Tove Slyngstad, Kirsti Vik Hjerkind, Jan Ivar Martinsen and Elina Vinberg at the Janus Serum Bank/Cancer Registry of Norway and Sven Ove Samuelsen at the Department of Mathematics, University of Oslo, for valuable assistance in planning this project. Further, we also thank Lill Tove Nilsen and Bjørn Johnsen at the Norwegian Radiation Protection Authority and Reza Ghiasvand at the Department of Biostatistics, University of Oslo, for the development of the UVR exposure data.
References
Footnotes
Contributors TER conceived the study. JSS, TKG, JRR, LV, RB, MBV and TER contributed to the project design. TER and JSS are responsible for data acquisition. JSS and TER drafted the manuscript, and MBV, TKG, JRR, LV and RB reviewed and revised it critically for important intellectual content and approved the final version for submission. JSS and TER are the guarantors.
Funding The research project has been reviewed and granted funding by the Norwegian Cancer Society (no 5829980-2014) and the Cancer Registry of Norway Research Fund.
Competing interests None declared.
Ethics approval This project has approval from the Regional Committee for Medical and Health Research Ethics (no 2014/185).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Requests for data sharing/case pooling may be directed to the corresponding author. This project uses third-party data derived from State government registries, which are ultimately governed by their ethics committees and data custodians. Thus, any requests to share these data will be subject to formal approval from each data source used in this project.
Correction notice This paper has been amended since it was published Online First. Owing to a scripting error, some of the publisher names in the references were replaced with 'BMJ Publishing Group'. This only affected the full text version, not the PDF. We have since corrected theseerrors and the correct publishers have been inserted into the references.