Article Text

Abstract
Objective To investigate the risk of dementia in patients with stroke who did and did not receive acupuncture treatment.
Design Retrospective cohort study.
Setting This study was based on Taiwan’s National Health Insurance Research Database that included patients with stroke hospitalised between 1 January 2000 and 31 December 2004.
Participants We identified 11 220 patients aged 50 years and older with newly diagnosed stroke hospitalisation.
Primary and secondary outcome measures We compared the incident dementia during the follow-up period until the end of 2009 in patients with stroke who did and did not receive acupuncture. The adjusted HRs and 95% CIs of dementia associated with acupuncture were calculated in multivariate Cox proportional hazard regressions.
Results Acupuncture treatment was associated with a decreased risk of dementia with multivariate adjustment (HR, 0.73; 95% CI 0.66 to 0.80), and the association was significant in both sexes and every age group, as well as in groups with ischaemic stroke, with fewer medical conditions and those hospitalised after stroke. Patients with stroke received acupuncture treatment, and conventional rehabilitation was associated with a significantly reduced risk of poststroke dementia (HR, 0.64; 95% CI 0.56 to 0.74).
Conclusions This study raises the possibility that patients with non-haemorrhagic stroke who received acupuncture had a reduced risk of dementia. The results suggest the need for prospective sham-controlled and randomised trials to establish the efficacy of acupuncture in preventing dementia.
- Dementia
- Stroke
- acupuncture
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
We used a matching procedure with a propensity score to reduce the confounding effects.
Multivariate Cox proportional hazard models were used to control the residual confounding bias.
Our data lacked clinical risk scores, lesion characteristics, biochemical measures and lifestyles of patients with stroke.
The actual acupuncture points used in the treatment were not available.
The mode of acupuncture treatment for patients with stroke varied among traditional Chinese medicine physicians.
Introduction
Dementia represents a major burden of disease worldwide. An estimated 47 million people lived with dementia in 2015, and the ageing of the population worldwide is expected to triple this number by 2050.1 Dementia also represents a substantial financial burden on society; for example, US dementia care costs are estimated to reach $215 billion per year.2 Dementia commonly occurs after a stroke, with the 1-year incidence of poststroke dementia ranging from 7.4% to 41.3%.3 Poststroke dementia is one of the major determinants of dependency among patients with stroke, and it also predicts the recurrence of ischaemic stroke in long-term follow-up.4 5
Given ageing populations and declining mortality after a stroke,5 it is important to prevent dementia among stroke survivors. Strategies have been suggested to reduce cognitive decline and the subsequent risk of dementia; these include regular physical activity, increased fruit and vegetable consumption, and the management of medical risk factors (diabetes, obesity, smoking, depression and hypertension).6 7 Nevertheless, active interventions to prevent poststroke dementia deserve further investigation.8
Acupuncture is a technique in which fine needles are inserted and manipulated at specific points on the body to achieve therapeutic purposes, and it is integral to everyday medical practice in many nations around the world.9 A 2002–2007 US study found some 3.1 million adults and 150 000 children had acupuncture in the previous year, as reported in the 2007 National Health Interview Survey.9 10 While some clinical studies and systematic reviews support acupuncture’s effectiveness in poststroke rehabilitation,11–15 these therapeutic effects remain unclear due to poor methodology and small sample sizes.
Whether acupuncture is effective in reducing dementia in patients with stroke remains unknown. Using the Taiwan National Health Insurance Research Database, we conducted a nationwide matched cohort study to investigate the results of acupuncture treatment in reducing poststroke dementia.
Patients and methods
Source of data
Research data were obtained from the reimbursement claims of Taiwan’s National Health Insurance Programme, which was implemented in March 1995 and covers more than 99% of Taiwan’s 23 million residents. The National Health Research Institutes established a National Health Insurance Research Database, which records all beneficiaries’ medical services for public research interest. This information includes inpatient and outpatient demographics, primary and secondary diagnoses, procedures, prescriptions, and medical expenditures. The validity of this database has been favourably evaluated, and research articles based on it have been accepted in prominent scientific journals worldwide.8 16–18
Ethical approval
Insurance reimbursement claims used in this study were from Taiwan’s National Health Insurance Research Database, which is available for research access. This study was conducted in accordance with the Helsinki Declaration. To protect personal privacy, the electronic database was decoded with patient identification scrambled for further academic access for research. According to the National Health Research Institutes regulations, informed consent is not required because of the use of decoded and scrambled patient identification. This study was evaluated and approved by the Joint Institutional Review Board of Taipei Medical University (TMU-JIRB-201505055) and E-DA Hospital (EDA-JIRB-2014012).
Study design
Of the 23 million people in Taiwan, we identified 226 699 new stroke survivors aged ≥50 years admitted to the hospital (people who visited inpatient care with a physician’s primary diagnosis of stroke) between 1 January 2000 and 31 December 2004. The diagnosis of stroke was validated in previous studies.8 16–18 To confirm that all patients with stroke in our study were incident cases, only new-onset stroke cases were included; patients with previous records of stroke within 5 years before the index date were excluded. Among the subjects, 5610 received at least five courses (one course consisted of six consecutive treatments) of acupuncture treatment after stroke admission. To select appropriate study subjects, patients with stroke with only one to four courses of acupuncture treatment were excluded. Patients with stroke without acupuncture treatment were selected by a matched pair procedure with propensity score (exposure vs non-exposure ratio=1:1). For the non-acupuncture group, patients with stroke were followed up from the discharge date following stroke admission (index date) until 31 December 2009, or until the dementia event occurred, was lost to follow-up or death. For the acupuncture group, patients with stroke were followed up from the first date of receiving acupuncture treatment after stroke admission (index date) until 31 December 2009, or until the dementia event occurred, was lost to follow-up or death. In the acupuncture group, the time period between discharge date after stroke admission and the date of first acupuncture treatment after stroke admission was the immortal time. Therefore, the immortal time bias (resulting from the overestimation of the intervention’s beneficial effects) was avoided in this study. The follow-up time, in person-years, was calculated for each patient with stroke from the index date to the end point. We compared the risk of incident dementia between patients with stroke who did and did not receive acupuncture treatment during the follow-up period.
Criteria and definition
In this study, low-income patients were defined as those qualifying for waived medical copayment, because this status is verified by the National Health Insurance system. We calculated the population density (persons/km2) for each of all administrative units in Taiwan. Based on population density, these units were stratified into tertiles to designate areas of low, moderate and high urbanisation. We defined newly diagnosed stroke according to the International Classification of Diseases, 9th Revision, Clinical Modification, as ICD-9-CM 430–437. The primary outcome as the incident event of dementia was defined by patients who sought medical care with a physician’s primary diagnosis of dementia (ICD-9-CM 290). Coexisting medical conditions were determined from medical claims for the follow-up period and included hypertension (ICD-9-CM 401–405), diabetes (ICD-9-CM 250), mental disorders (ICD-9-CM 290–319), chronic obstructive pulmonary disease (ICD-9-CM 490–496), ischaemic heart disease (ICD-9-CM 410–414), urinary tract infection (ICD-9-CM 599.0), hyperlipidaemia (ICD-9-CM 272.0–272.4), pneumonia (ICD-9-CM 480–486), congestive heart failure (ICD-9-CM 428), epilepsy (ICD-9-CM 345) and liver cirrhosis (ICD-9-CM 571). Renal dialysis was defined by the administration code (D8, D9). Subtypes of stroke, staying in a medical centre or not, length of hospital stay, admission to the intensive care unit, or receiving neurosurgery during the index stroke hospitalisation were also identified as potential confounding factors. Medications for stroke (anticoagulants, antiplatelet agents and lipid-lowering agents) were also considered.
Statistical analysis
To reduce confounding effects, we developed a non-parsimonious multivariable logistic regression model to estimate a propensity score for acupuncture treatment. Clinical significance guided the initial choice of covariates. These included age, sex, low-income status, urbanisation, hypertension, diabetes, mental disorders, chronic obstructive pulmonary disease, ischaemic heart disease, urinary tract infection, hyperlipidaemia, pneumonia, congestive heart failure, epilepsy, liver cirrhosis, renal dialysis, subtypes of stroke, stay in a medical centre, length of hospital stay, admission to the intensive care unit and receiving neurosurgery. We used a structured iterative approach to refine this logistic regression model to achieve a balance of covariates within matched pairs. We then matched (without replacement) patients who had acupuncture treatment with those who did not using a greedy matching algorithm with a calliper width of 0.2 SD of the propensity score log odds. The nearest neighbour algorithm was applied to construct matched pairs, assuming that the proportion of 0.95–1.0 was perfect. This method could remove 98% of the bias from measured covariates.19 20
To compare the balance between groups after the application of the propensity score, χ2tests were used to analyse categorised data between patients with stroke who did and did not receive acupuncture treatment. The mean and SD for age and length of hospital stay for patients with stroke with and without acupuncture treatment were compared using t-tests. We used a multivariable Cox proportional hazard model to analyse the adjusted HRs and 95% CIs for incident dementia associated with acupuncture treatment in patients with stroke. All analyses were performed using Statistical Analysis Software V.9.1. A two-sided p value of <0.05 was considered to be significant.
Results
After propensity score matching (table 1), there were no significant differences in the distributions of age, sex, low-income status, urbanisation, stay in a medical centre, length of hospital stay, stay in the intensive care unit, type of stroke, hypertension, diabetes, mental disorders, chronic obstructive pulmonary disease, ischaemic heart disease, urinary tract infection, hyperlipidaemia, pneumonia, congestive heart failure, epilepsy, renal dialysis, liver cirrhosis, physical rehabilitation, anticoagulants, antiplatelet agents and lipid-lowering agents between patients with stroke who did and did not receive acupuncture treatment.
The characteristics of stroke patients with and without acupuncture treatment
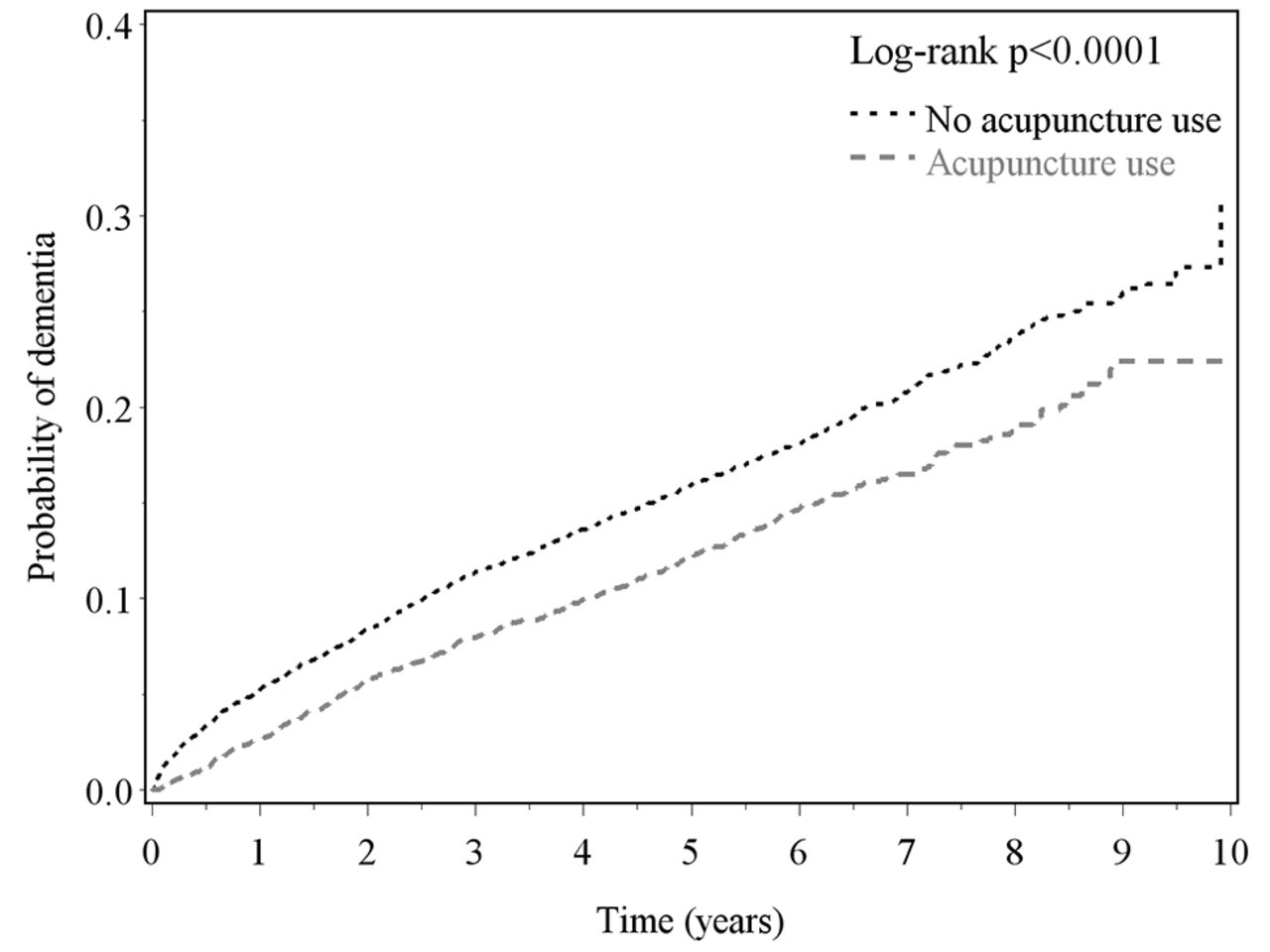
During the follow-up period (table 2), patients with stroke with acupuncture treatment had a lower incidence of newly diagnosed dementia (26.5 per 1000 person-years) than those without acupuncture treatment (34.6 per 1000 person-years), with an HR of 0.73 (95% CI 0.66 to 0.80)
Incidence and adjusted risks of dementia during the follow-up period in patients with stroke with and without acupuncture treatment
after adjustment for age, sex, low-income status, urbanisation, stay in a medical centre, length of hospital stay, stay in the intensive care unit, types of stroke, hypertension, diabetes, mental disorders, chronic obstructive pulmonary disease, ischaemic heart disease, urinary tract infection, hyperlipidaemia, pneumonia, congestive heart failure, epilepsy, renal dialysis, liver cirrhosis, physical rehabilitation, anticoagulant, antiplatelet agents and lipid-lowering agents. The log-rank test (figure 1) indicated that patients with stroke with acupuncture treatment had a lower probability of newly diagnosed dementia events than those without acupuncture treatment (p<0.0001).
{kind=link}
Cumulative incidence of dementia for patients with stroke with and without acupuncture treatment during the follow-up period.
Among patients with stroke (table 3), the decreased risk of newly diagnosed dementia associated with acupuncture treatment was significant in men (HR, 0.75; 95% CI 0.66 to 0.85) and women (HR, 0.70; 95% CI 0.60 to 0.80). The age-stratified results revealed adjusted HRs for dementia associated with acupuncture treatment for patients with stroke aged 50–59 years (HR, 0.64; 95% CI 0.47 to 0.86), 60–69 years (HR, 0.75; 95% CI 0.64 to 0.88), 70–79 years (HR, 0.72; 95% CI 0.63 to 0.83) and ≥80 years (HR, 0.54; 95% CI 0.38 to 0.76). The associations between reduced dementia and acupuncture treatment were also significant in patients with ischaemic stroke (HR, 0.74; 95% CI 0.66 to 0.84), other stroke (HR, 0.69; 95% CI 0.57 to 0.82), no medical conditions (HR, 0.55; 95% CI 0.39 to 0.77), 1 medical condition (HR, 0.64; 95% CI 0.52 to 0.80), 2 medical conditions (HR, 0.81; 95% CI 0.68 to 0.98), ≥3 medical conditions (HR, 0.82; 95% CI 0.71 to 0.95), <7 days of hospital stay (HR, 0.81; 95% CI 0.71 to 0.91) and ≥7 days of hospital stay (HR, 0.64; 95% CI 0.55 to 0.74).
Risks of dementia associated with acupuncture treatment in patients with stroke stratified by age, sex, type of stroke, medical conditions and length of stay*
Table 4 shows the joint effects of acupuncture and rehabilitation on dementia risk. Compared with patients with stroke who did not receive acupuncture and rehabilitation, patients with stroke receiving acupuncture and rehabilitation had the lowest risk of dementia (HR, 0.64; 95% CI 0.56 to 0.74). The beneficial effects for reducing dementia risk were also shown in patients with stroke who received acupuncture treatment but not rehabilitation (HR, 0.76; 95% CI 0.64 to 0.90).
Incidence and risk of dementia associated with acupuncture treatment and physical rehabilitation in patients with stroke
Discussion
This study found that patients with stroke receiving acupuncture treatment exhibited a significantly lower risk of dementia during the follow-up period compared with those without acupuncture in both sexes and people aged more than 50 years, but not in patients with haemorrhagic stroke. To our knowledge, this study may be the first report to show the results of acupuncture treatment on poststroke dementia.
Factors associated with poststroke dementia included age, sex, diabetes, traumatic brain injury and heart disease.3 21 22 To reduce confounding effects, we used multiple regressions to adjust sociodemographics (age, sex, low income, urbanisation), characteristics of stroke admission (subtypes of stroke, stay in medical centre, length of hospital stay, admission to intensive care unit, neurosurgery) and medical conditions (hypertension, diabetes, mental disorders, chronic obstructive pulmonary disease, ischaemic heart disease, urinary tract infection, hyperlipidaemia, pneumonia, congestive heart failure, epilepsy, liver cirrhosis, renal dialysis). In addition, these potential confounding factors were also matched by propensity score. The strengths of our study include this matching by propensity score and the retrospective cohort study, multivariate regression model, adjustment for immortal time bias and large sample size.
We found that the association between the reduced risk of poststroke dementia and acupuncture treatment existed in patients with stroke of both sexes aged ≥50 years, with a greater protective effect in patients with fewer medical conditions and those admitted to the hospital after their stroke. From an epidemiological viewpoint, the above phenomena validated the beneficial effects of acupuncture treatment in reducing risk of poststroke dementia. However, our subgroup analysis found that patients with haemorrhagic stroke who received acupuncture treatment did not show a reduced risk of dementia during the follow-up period. Patients with haemorrhagic stroke had poorer outcomes (such as mortality, dependency, disabilities and modified Rankin Scale score) than those with ischaemic stroke.23 Patients with haemorrhagic stroke were also more likely to develop dementia than those experiencing ischaemic and other types of stroke.3 According to the previous studies based on the data from Taiwan’s National Health Insurance Research Database,24 25 patients with haemorrhagic stroke had a longer length of hospital stay and higher mortality than patients with ischaemic stroke. The greater severity in patients with haemorrhagic stroke may have diluted the effect of acupuncture on reducing poststroke adverse outcomes.26 27 Additionally, the small sample size of dementia cases in the patients with haemorrhagic stroke also decreased the statistical significance of acupuncture’s effect. These two reasons might explain why there was no significant reduction in the risk of dementia in patients with haemorrhagic stroke who received acupuncture treatment. In addition, our analyses show that combined acupuncture treatment and rehabilitation has the most beneficial effect in reducing dementia risk. This finding is not surprising because one of our previous studies showed reduced dementia in patients with stroke who received conventional rehabilitation.8
Acupuncture is one of several treatments used in rehabilitation programmes for patients with stroke and is generally considered safe and well-tolerated.12 15 The incidence of acupuncture-related adverse reactions is relatively low, particularly when treating patients with Alzheimer’s disease or cerebral infarction.9 28–30 In a large cross-sectional study of more than 34 000 acupuncture treatments in the UK in 2001, no serious adverse events (such as hospitalisation, permanent disability or death) were reported in relation to acupuncture treatment, and the rate of underlying minor adverse events (such as nausea, fainting, prolonged aggravation of existing symptoms and psychological or emotional reaction) was reported to be 0–1.1 per 10 000 treatments.9 29 Nevertheless, the surveillance of major or minor adverse events during acupuncture treatment is necessary in future studies.
To clarify the effects of acupuncture treatment in reducing dementia in patients with stroke, we propose some possible explanations. First, acupuncture treatment (acupoints: Tai chong (Liv3) and He gu (LI4)) can cause activation in the regions with decreased activity; it can also cause deactivation in the regions with increased activity for patients with mild cognitive impairment and Alzheimer’s disease.31 Second, several studies show acupuncture’s effectiveness in improving physical abilities as well as wellness indicators, such as blood pressure.12 32 Acupuncture has been found to reduce or relieve depression,33 34 anxiety,35 obesity,36 migraine37 and Parkinson’s disease34 38; these factors are also associated with increased risk of dementia.39–43 Third, patients with stroke who choose acupuncture treatment may have better knowledge, attitudes and practices regarding physical rehabilitation and disease prevention; these factors could also contribute to reduced incidence of dementia after stroke.
This study has some limitations. First, we used insurance claims data that lacked information on clinical risk scores (such as the National Institutes of Health Stroke Scale or the Barthel Index), lesion characteristics such as location or size, biochemical measures, and patient lifestyle factors such as smoking, drinking alcoholic beverages and physical activity. Second, our study could not validate the actual acupuncture points used in treatment given the limited information provided by the National Health Insurance Research Database. Because acupuncture treatments for patients with stroke vary, we could not confirm that all traditional Chinese medicine physicians performed the same procedures or used the same acupuncture points. Finally, residual confounding is always possible, although we used propensity score matching procedure and multivariate regression adjustment for several potential confounding factors in our analysis.
To the best of our knowledge, our study is the first population-based study that rigorously evaluated the impact of acupuncture treatment on the risk of dementia in patients with stroke. We found that patients with non-haemorrhagic stroke receiving acupuncture treatment had a reduced risk of dementia. Although the beneficial effect of acupuncture on dementia risk was investigated in this study, future population-based studies that overcome the limitations of this study are needed to provide more evidence of this association.
Acknowledgments
This study is based in part on data obtained from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Ministry of Health and Welfare, and managed by the National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Ministry of Health and Welfare, or National Health Research Institutes.
References
Footnotes
Contributors All the authors revised and approved the contents of the submitted article. C-CL and C-CS created the idea of the manuscript. C-CL and H-LL conducted statistical analysis of data. C-CS and C-CL wrote the manuscript. All the authors made substantial contributions to interpretation of data and carried out a critical revision of the manuscript for important intellectual content.
Contributors Prof. Ta-Liang Chen has equal contribution with the corresponding author
Funding This research was supported in part by Taiwan’s National Union of Chinese Medical Doctors’ Association (UNCMA104-H-001), Shuan Ho Hospital and Taipei Medical University (104TMU-SHH-23), Ministry of Science and Technology (MOST105-2629-B-038-001; MOST105-2314-B-038-025; MOST104-2314-B-038-027-MY2; MOST103-2320-B-214-010-MY2; NSC102-2314-B-038-021-MY3), the Committee on Chinese Medicine and Pharmacy, Department of Health, Taiwan (Grants nos. CCMP98-RD-038 and CCMP99-RD-035), and Taiwan’s Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW106-TDU-B-212-113004).
Competing interests None declared.
Patient consent To protect personal privacy, the electronic database was decoded with patient identification scrambled for further academic access for research. According to National Health Research Institutes regulations, informed consent is not required because of the use of decoded and scrambled patient identification.
Ethics approval This study was evaluated and approved by the Joint Institutional Review Board of Taipei Medical University (TMU-JIRB-201505055) and E-DA Hospital (EDA-JIRB-2014012).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data set available from the Taiwan’s National Health Research Institutes.