Article Text

Abstract
Introduction Mechanically ventilated children in paediatric intensive care units are commonly administered analgesics and sedative agents to minimise pain and distress and facilitate cooperation with medical interventions. Opioids and benzodiazepines are the most common analgesic and sedative agents but have safety concerns. The α2 agonists clonidine and dexmedetomidine are alternative sedatives in use despite neither having robust evidence to support their use. Studies evaluating effectiveness of α2 agonists to date have not focused on sedation-based outcomes instead focusing on opioid-sparing properties and ventilation outcomes. The aim of this study is to evaluate if an opioid-based sedation regimen, with an α2 agonist adjunct (clonidine or dexmedetomidine), produces a non-inferior proportion of time adequately sedated compared with a control group without an α2 agonist adjunct, while conferring potential additional benefits such as reduced opioid administration and less exposure to potential additional agents such as benzodiazepines.
Methods and analysis We will conduct a retrospective cohort study in two Irish paediatric intensive care units using clinical information on patient characteristics, sedation scores and drug use. Eligible children admitted between January 2014 and June 2016 who were mechanically ventilated and received an opioid infusion will be included. Patients will be categorised into two exposure categories (received an α2 agonist or did not receive an α2 agonist) and the time adequately sedated (measured using the COMFORT Behaviour Score) will be calculated using interpolation of nursing sedation scores at each recorded time point. At least 150 per group is planned for inclusion to ensure adequate study power. Propensity score matching will be used in analysis to account for potential confounding by indication.
Ethics and dissemination The study has been approved by the ethics committees of both hospitals. Dissemination will occur via local, national and international presentations for academic and healthcare audiences as well as through peer reviewed publications.
- Paediatric intensive & critical care
- clonidine
- dexmedetomidine
- sedation
- adrenergic 2-receptor agonists
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Both clonidine and dexmedetomidine are in routine use in children with limited information on efficacy; this study examines effectiveness based on clinical data from a large cohort of patients from two paediatric intensive care units (PICUs).
Both PICUs use a validated sedation score: the COMFORT Behaviour score, which allows calculation of a sedation-based primary outcome to determine sedative effectiveness of α2 agonists; an outcome which studies to date have yet to evaluate.
The PICU population is heterogeneous which may lead to confounding by indication due to the non-randomised design of the study. To minimise the influence of confounding, we will use statistical techniques such as propensity scores to adjust our findings for the most important confounders.
Neither clonidine nor dexmedetomidine are licensed for use in children nor have their optimal dosage regimens been defined. A substudy will evaluate dose–response relationships for different dose bands of each agent.
Introduction
Distress and anxiety management is an integral part of paediatric critical care and can be achieved by non-pharmacological and pharmacological interventions. The use of sedatives is important to modifying stressors in the environment and to promote comfort in the ill child.1 Over 90% of mechanically ventilated children receive sedatives as part of treatment.2 These are used to maintain comfort, facilitate stressful interventions, attenuate the stress response and reduce metabolic demands during periods of cardiac, respiratory and neurological instability.3 4 The practice of sedation itself is a clinical balance between both states of undersedation and oversedation which represent hazards to the critically ill child. Undersedation may lead to distress and adverse events such as unintentional extubation or displacement of catheters as well as increased lengths of stay.5 6 Conversely, oversedation can cause cardiovascular depression and ileus, may interfere with comprehensive neurological examinations and, with prolonged sedation, tolerance and withdrawal phenomena may occur.6 7
Pharmacological interventions are the cornerstone to achievement of adequate sedation and analgesia. Consensus statements for critically ill children recommend continuous infusions of morphine or fentanyl for relief of severe pain.1 Opioids are the preferred analgesics because of their marked useful sedative effects.8 Combination therapy of analgesics and other sedatives is often required in clinical practice with midazolam and other benzodiazepines commonly co-prescribed.9 Yet, opioids and benzodiazepines are well known to produce tolerance, dependence and a number of unwanted side effects including cardiovascular and respiratory depression in children.10 Animal studies also suggest the risk of neurotoxicity and impaired neurodevelopment with use of these agents.11 It is unclear whether this translates to impairment of human cognitive and functional outcomes.11 The critical variables of dose and duration of exposure to anaesthetic and sedative agents do however create a subset of sedated infants who are potentially at greater risk of longer-term cognitive impairment.12 Alternative sedative options are available through the use of α2 agonists.1 Their alternative mode of action has been reported to deliver a lighter sedation with less potential for unwanted adverse effects as seen with traditional agents.13 14 Both clonidine and dexmedetomidine are α2 agonists in routine use in clinical practice in an off-label manner, similar to many analgesics and sedatives.15 Clonidine, licensed as an antihypertensive in adults, was the first α2 agonist to enter use as a sedative in paediatrics though lack of dosing information and formulation availability limit its potential use. Dexmedetomidine is eight times more selective than clonidine for the α2 over the α1 receptor and thus may confer less unwanted adverse effects. It is also licensed in adults for intensive care unit (ICU) sedation and has a shorter half-life allowing easier titration of infusions to sedative effect.
The goal of sedation therapy is to have most patients free of distress, safe and somewhat interactive with their environment.2 This should ideally be achieved with the minimal amount of medications possible. The level of sedation reached can be assessed by sedation assessment scales and should be reassessed regularly to ensure that the optimal level of sedation is maintained.1 Sedation assessment scales further facilitate titration of sedative medications. One of the most widely used sedation assessment scales is the COMFORT Behaviour scale.16 This is a modified version of the original COMFORT scale17 which excluded the physiological parameters (blood pressure and heart rate) of the original scale. This leaves a six-parameter non-intrusive measure of behaviours designed to assess distress and response to sedatives. Following a 2 min observation period, the assessor rates alertness, calmness-agitation, respiratory response in mechanically ventilated children (or crying in spontaneously breathing children), physical movement, muscle tone and facial tension. Each parameter is marked on a scale ranging from 1 to 5 and summed to give an overall score from 6 to 30. A separate Nurse Rating scale estimates any pain experienced by the patient. The COMFORT Behaviour scale is validated for use in mechanically ventilated and non-mechanically ventilated children including preterm infants, neonates and children with Down syndrome.16 18–20 The COMFORT Behaviour scale has good internal consistency with a Cronbach’s alpha estimated at 0.84 in a validation study of 78 patients.16 Nurses displayed high interobserver validity with a median linearly weighted Cohen’s kappa of 0.84 (range 0.67–0.96) for 52 nurses.16 Medication adjustments are recommended at scores of <11 and ≥17 for subsequent risk of oversedation and undersedation, respectively.21 22 Those scores in between are considered to be representative of an adequately sedated state.
Despite their frequent use in critically ill children, the real additive value of using clonidine or dexmedetomidine for sedation is not yet established.23 A Cochrane review in adults showed that dexmedetomidine reduced the duration of mechanical ventilation (−22%) and intensive care stay (−14%) compared with standard sedation regimens.24 Our recent systematic review summarises the current evidence on efficacy of clonidine and dexmedetomidine as sedatives in paediatric critical care.25 The review highlighted the current lack of evidence from randomised controlled trials supporting efficacy of either agent. The US Food and Drug Administration has advocated for quality of sedation-based outcomes in the determination of efficacy of sedative drugs in paediatrics using validated sedation assessment scales such as the COMFORT score.16 26 Pivotal adult studies of the α2 agonist dexmedetomidine used proportions of time at target sedation levels as their primary outcome using validated sedation scales.27 In contrast, only one included study in the systematic review of paediatric trials used a validated clinical sedation score-based outcome and this study evaluating clonidine efficacy failed to meet the planned recruitment numbers.28 The remaining studies used primary outcomes based on other measures such as potential opioid-sparing effects or duration or mechanical ventilation.29–33 The systematic review also described some reports outlining the potential for clonidine to reduce opioid and benzodiazepine co-administration in mechanically ventilated children and for dexmedetomidine to allow for shorter time to extubation after surgery in children.25 Furthermore, the optimal dosage strategies for both clonidine and dexmedetomidine remain undefined which limits their potential benefit in clinical practice. This needs to be addressed before further interventional studies are planned.
Given the importance of achieving adequate sedation in critical care, the lack of existing evidence from published randomised controlled trials, the lack of studies which used sedation-based outcomes and the routine use of α2 agonists in clinical practice, we plan to conduct a multisite retrospective cohort observational study of effectiveness within the two largest Irish paediatric intensive care units (PICUs). Applying the design and analysis principles of the adult dexmedetomidine trials, we will use a robust design of primarily evaluating non-inferiority of time adequately sedated comparing mechanically ventilated children who received an α2 agonist (either clonidine or dexmedetomidine) to a control group receiving opioids and benzodiazepines.27 If the prerequisite of non-inferiority of quality of sedation holds, secondary outcomes will then evaluate any additional opioid or benzodiazepine-sparing effect conferred by the additional of the α2 agonists.
Methods and analysis
We will conduct a multisite retrospective cohort study of paediatric mechanically ventilated patients at the PICUs of Ireland’s two tertiary paediatric hospitals. The PICUs at Our Lady’s Children’s Hospital, Crumlin, Dublin (OLCHC) and The Children’s University Hospital, Temple Street Dublin (TSCUH), are the nation’s only PICUs with approximately 1700 annual admission combined.
The study period is planned to be over a 2-year period from 1 January 2014 to 30 June 2016. These dates have been chosen based on the availability of an adequately large patient population who would have been exposed to the study drugs as well as coinciding with the availability of electronic patient information. The observation period when data for outcomes will be recorded is that during which the patient is mechanically ventilated as shown in figure 1.

Observation periods for study groups. MV, mechanical ventilation.
The start time for the α2 agonist group will be from the time of the first administration of either clonidine or dexmedetomidine (T2a). The end time will be the time of end of mechanical ventilation (T3). Proportion of the time from T2a to T3 judged to be adequately sedated will be calculated for the primary outcome comparison. The period of time (hours) from beginning of mechanical ventilation (T1) to first administration of an α2 agonist (T2a) will be recorded and included as a time-varying covariant in subsequent analysis.
For the control group which did not receive an α2 agonist, their corresponding observation period start time (T2c) will be defined as the point at which analgesia and sedation therapy is ‘stepped up’. This will be defined as any of the following:
administration of a rescue morphine or midazolam bolus;
administration of chloral hydrate;
commencement of a midazolam infusion;
increase in background opioid infusion.
For this control, the corresponding proportion of time from T2c to T3 adequately sedated will also be calculated. The preceding lag time before T2a and T2c will be left censored. These observation time periods for both groups will be used for calculation of opioid and benzodiazepine use for calculation of secondary outcomes. We will right censor for patients who die or remain in the study at the end of the study period. The left-censored lag time will be included in the propensity score model. Long stay patients with study times >28 days will be excluded from the study as they may not be representative of the general PICU population.
Data for clinical details, exposure and outcomes measures will be extracted from a combination of the electronic clinical information systems, local PICANET audit data34 and hardcopy medical records. Patients will be followed up for the duration of their PICU stay. The study protocol has been compiled with regard to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist of items to be included in reports of cohort studies.35
Inclusion and exclusion criteria
All patient admissions where the patient was mechanically ventilated in the two study PICUs will be allocated a unique encounter identification number. These encounters will then be further screened against the below eligibility to generate a database of potentially eligible patients. All eligible patients from the solely electronic site (OLCHC) will be included. The second site (TSCUH) requires additional manual data extraction from medical records. Approximately 4 months will be spent extracting the extra data from this site sampling randomly across the 2-year study timeline. The final included patients will be a representative sample of both study sites distributed across the study groups.
Only patients meeting all of the following criteria will be included:
PICU inpatient between 1 January 2014 and 30 June 2016 at either hospital;
first admission during study time period;
received mechanical ventilation for >8 hours;
received an infusion of an opioid;
COMFORT Behaviour scores recorded (>2 scores).
Patients with one or more of the following criteria will be excluded:
COMFORT Behaviour scores not valid (severe neurodevelopmental delay, severe autism, severe hypotonia or those receiving continuous neuromuscular blockade);
COMFORT Behaviour scores not recorded (<2 scores);
administered an α2 agonist for an indication other than sedation;
study durations >28 days;
opioid infusions other than morphine.
Exposure measures
For the primary outcome, patients will be categorised into two exposure groups: (1) α2 agonist exposed (2) no α2 agonist exposure (control group) based on the sedative agents administered while mechanically ventilated. Included patients will be described according to the characteristics shown in table 1.
Patient characteristics.
Primary outcome
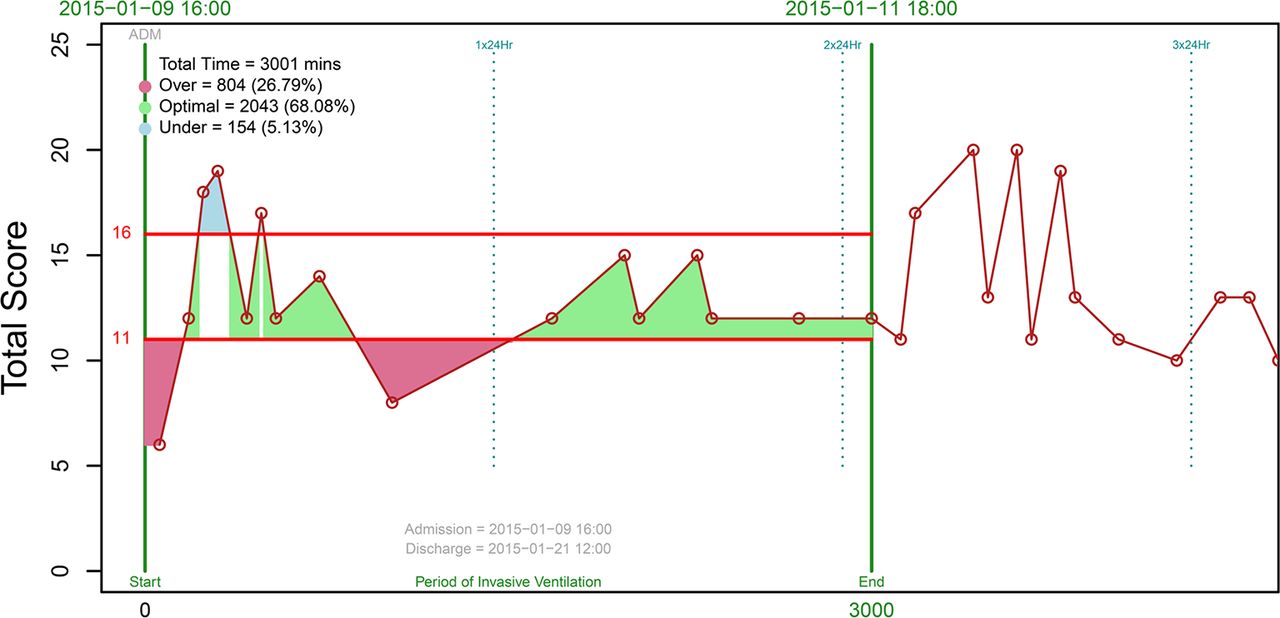
The primary outcome of this study is the proportion of time adequately sedated while mechanically ventilated. Level of sedation will be measured using the validated COMFORT Behaviour score. We define ‘adequately sedated’ as COMFORT Behaviour scores recorded at 11–16 inclusive as scores outside this range may indicate oversedation, undersedation or a requirement for medication adjustment. The recorded time of COMFORT Behaviour scores at each assessment point will be plotted (see figure 2) and, by linearly connecting these, we will calculate the time in the respective sedation states: adequately sedated (COMFORT Behaviour score 11–16), potentially undersedated (COMFORT Behaviour score >16) and potentially oversedated (COMFORT Behaviour score <11). Sedation protocols in both units recommend assessing clinical sedation scores every 4 hours while mechanically ventilated. In practice, COMFORT Behaviour scoring tends to occur more frequently (every 2–3 hours on average) with more frequent scoring occurring with restless children. Nursing staff are also instructed to repeat COMFORT Behaviour scores to evaluate effectiveness of non-pharmacological and pharmacological interventions approximately 30 min post intervention. This more frequent scoring will reduce the potential for misclassification of time. It has also been reported that the COMFORT Behaviour score is sensitive to detect change following pharmacological and non-pharmacological sedation interventions.36
{kind=link}
{kind=link}
Calculation of primary outcome for a patient mechanically ventilated for 3001 min.
We will investigate patients with very low calculated proportions of time adequately sedated (<20%) to see if they had a different sedation target due to clinical necessity and if so they will be excluded from the analysis.
Planned secondary outcomes
proportion of time potentially oversedated;
proportion of time potentially undersedated;
opioid use, infusion and bolus doses (expressed as morphine μg/kg/hour) during the observation period;
change in opioid infusion rate from baseline infusion rate to average infusion rate (expressed as morphine μg/kg/hour);
midazolam use, infusion and bolus (expressed as midazolam μg/kg/hour);
number of chloral hydrate boluses/24 hours;
number of paracetamol boluses/24 hours;
duration of mechanical ventilation (days);
ventilator-free days;6
duration of PICU stay (days).
Determination of potential benefit of α2 agonists
This study design adopts a hierarchical set of outcomes. Similar to the design of the largest adult trials of sedatives, we have set the prerequisite that an α2-based regimen is non-inferior to an opioid/benzodiazepine control regimen before we compare potential benefits such as lessening the amount of other sedatives administered.27 We believe this is more rigorous than simply describing similarity of average sedation scores. Only if non-inferiority can be confirmed can we explore fully the benefits of an α2-based regimen. Meeting the primary outcome alone does not form the basis of evidence of α2 effectiveness but allows us then to evaluate benefits in our secondary outcomes that may provide evidence for potential benefits of α2-based regimens. The addition of the α2 agonists may produce a deeper sedation and we will also report on time potentially oversedated and undersedated for both groups to allow the reader contextualise any secondary outcome benefits with the depth of sedation achieved.
Using an assessment score like the COMFORT Behaviour score as a guiding therapy for sedative use and also as an outcome measure would not usually be an appropriate study design as reactionary and compensatory use of other drugs may artificially increase time adequately sedated. However, in this specific context, similar to the adult dexmedetomidine trials,27 meeting the primary outcome alone does not determine effectiveness. It is a prerequisite to evaluate other potential benefits in the secondary outcomes. Compensatory use of other drugs to ensure maintenance of target sedation that may occur will be captured by our selected secondary outcomes on opioid and benzodiazepine use. Hence, if this compensation occurs it will be measurable to us and even if the α2 regimen meets the primary outcome no benefit will be seen in the secondary outcomes and we cannot interpret the results as a sign of α2 effectiveness.
Confounding factors
Confounding by indication is an important consideration in pharmacoepidemiological observational studies of drug effects. This type of confounding arises from the fact that patients who are prescribed a medication may be different from those not prescribed the drug. In our context, this may arise if, for example, sicker patients are prescribed clonidine or dexmedetomidine as reserve agents compared with those receiving first-line agents like opioids and midazolam. To minimise this risk of confounding, we will use propensity score analysis. This creates probability scores for receiving exposures or treatments that allow comparisons to unexposed patients. It is a direct way of adjusting for confounding but relies on the confounders being identifiable and measurable. We will capture a comprehensive list of patient and practice characteristics which will be considered for inclusion as potential confounders in our analyses. Details of potential confounders to be included in the process of constructing a propensity score model are included in the data analysis section. Sedation guidelines within both PICUs leave the decision to use α2 agonists to individual physician preference which should generate a degree of randomness in the distribution of exposed and unexposed groups as exposure is less influenced by inherent patient characteristics. We will also capture all drug exposure information for patients, diagnoses and comorbidity alongside severity of illness scores to attempt to further minimise confounding by indication.
Data analysis plan
All variable and outcome data will be plotted to assess normality. Normally distributed data will be described by a mean and SD while non-parametric data will be described by medians and IQRs. Tests of statistical significance will be assumed significant at the level of p<0.05.
Matching
We will estimate using a logistic regression the propensity score for receiving treatment with an α2 agonist. Predicted probability values for being exposed to one drug over the unexposed on a range from 0 to 1 will be estimated using a combination of measured variables (potential confounders) incorporated into the models. Rosenbaum bounds will then be calculated to determine sensitivity to unmeasured confounders. Matching quality will be assessed for balanced covariants. Once propensity scores are estimated, the outcomes for α2 agonist-exposed patients can be contrasted with outcomes of the control patients. The overlap and region of common support will be checked between the exposed and cohorts. We will then trim the samples by excluding patients corresponding to extremes of propensity score. We will then use 1:1 and nearest neighbour matching with replacement. A maximum difference of 0.2 ×SD of the propensity score will be set as a calliper interval for distances between propensity score matches. Patient and hospital-level potential confounders which will be included in the process of constructing a propensity score include hospital site, age, weight, gender, pre-existing diseases, severity of illness, risk of mortality and baseline dose of analgesic and sedative drugs.
Primary outcome analysis
The proportion of time adequately sedated for the α2 agonist-exposed group (clonidine and dexmedetomidine patients) will be compared with the corresponding proportion for a non-α2 agonist-exposed group, mimicking the primary analysis of the adult dexmedetomidine trials.27 Non-inferiority will be assessed using a two-sided 95% CI for the estimated ratio of proportion of time in range for the exposed and non-exposed groups. If the lower limit of the CI of the estimated α2 agonist to control group ratio of proportion of time in range is >0.875 (within the non-inferiority threshold of 12.5%), then non-inferiority is inferred. If the test is successful, we will then proceed to analyse the study for a superiority conclusion. No statistical adjustment is required for this planned sequence of analyses.
Secondary outcome analyses
All of the prespecified secondary outcomes will result in continuous outcome variables. Paired t-tests will be used to evaluate differences between treatment groups and unexposed controls. Non-parametric equivalents such as the Mann-Whitney U test will be considered in the event of skewness of data.
Other analyses
While the primary outcome of this study combines patients who received clonidine and dexmedetomidine into one α2 agonist cohort, we anticipate having a larger subcohort of clonidine-exposed than dexmedetomidine-exposed patients. In secondary analyses, we will evaluate the two α2 agonist subgroups (clonidine and dexmedetomidine) in terms of the prespecified outcomes. We do not anticipate having enough dexmedetomidine patients to power the study for three independent groups a priori. We will however form a series of triplets of closely matching clonidine, dexmedetomidine and control patients to increase study power and allow inter-drug comparisons between clonidine and dexmedetomidine.
We plan to further analyse by potential effect modifiers such as dose range bands for both agents, matching different dose bands by propensity score ranges and examining for differential responses to highlight potentially favourable dose bands for future studies. We will also evaluate diagnostic category subgroups such as postsurgery and by reason for admission to allow comparisons in more homogenous groups. A subgroup analysis for those with and without neurodevelopmental disorders is also planned.
Determination of non-inferiority limit
Pilot data from the patient data population estimate that the control group is adequately sedated 68% of the time. Allowing for a non-inferiority margin of 12.5%, we would accept the test groups to be not inferior when adequately sedated >59.5% of the time. This is acceptable both clinically and also this threshold corresponds to 2 hours less adequately sedated on a 24-hour clock. Anything >2 hours is likely to be detectable on regular sedation score-based nursing monitoring.
Sample size calculation
Taking a conservative estimate of 65% of time adequately sedated (lower than from pilot data) and an acceptable non-inferiority limit of 12.5%, a sample size of 150 per group would be required to give 90% power when testing our hypothesis. We will therefore require at least 150 patients who received an α2 agonist and 150 suitable unexposed patients given a total of at least 300 patients in the overall study. As this is retrospective data and we are seeking to enhance the quality of our matching potential, we will extract data for more patients as some may need to be excluded when ensuring quality matches. Manual data extraction from charts will be the rate-limiting factor that determines our number of included patients over the data extraction period.
Missing data
Due to the observational nature of the study, there will be varying numbers of data points recording COMFORT Behaviour scores while mechanically ventilated. Protocols in place on both units recommend sedation scoring every 4–6hours. We will describe the extent and patterns of COMFORT Behaviour scores in both units. By design we evaluate proportion of time adequately sedated. This intentionally minimises the impact of some patients having more or less regular scores recorded versus other studies which report number of episodes of oversedation or undersedation scores. We will also perform a sensitivity analysis excluding those with a low amount of COMFORT Behaviour scores recorded (eg, <60% expected assessments)
Sources of bias
Selection bias would result is a distortion of the measurement of treatment effect due to selection into the study of groups of patients who have an unusual and unequal relationship between drug exposure and outcome.37 To reduce this risk, we include all eligible patients from the larger PICU site at OLCHC. At the second site at TSCUH due to the existence of paper records, we will sample randomly from all eligible patients throughout the study period. Due to the nature of monitoring in PICU and the short study time, there will be no patients lost to follow-up. The fact that sedative choice is influenced by physician preference also reduces the risk of selection bias.
A potential limitation of the COMFORT Behaviour score is that scoring is based on a 2 min observation window and not a longer time period. Second, the middle area of the COMFORT Behaviour scale is regarded as less reliable for predicting undersedation and oversedation. In particular, the value of 11 can be debated to be more likely to represent adequately or not adequately sedated. We initially will consider 11 as adequately sedated based on local practice, but a sensitivity analysis will be carried out to examine the potential implications of classifying the 11 as adequate or inadequately sedated. Exposure to drug may also be time varying. For our initial analysis of effectiveness, we will consider exposures as fixed, but in future further analysis will evaluate the effect of consideration of exposure as time varying.
Outcomes
Anticipated effectiveness and safety outcomes from the primary and secondary outcomes are shown in table 2. Data will be presented in both unadjusted and adjusted formats. Any differences will be described in clinical and statistical significance.
Ethics and dissemination
We have obtained ethical approval from the ethics committee of OLCHC and the ethics committee of TSCUH. Two articles are currently planned to be submitted to international peer reviewed journals: (1) results from the comparative effectiveness study and (2) results from a sub study evaluating dose–response relationships with clonidine and dexmedetomidine. The reporting will be in accordance with the ‘STROBE criteria’.35 Further dissemination of study results is planned for national and international conferences in the area as well as locally in both hospitals for clinical information.
Planned outcome measures
Acknowledgments
The authors acknowledge the statistical advice given by Dr Tim Grant during the study design.
References
Footnotes
Contributors JCH drafted the manuscript and developed the study protocol. ID designed a clinical information data extraction method for the protocol. CB, MH, JF and DRD provided a clinical expertise review and conceived the project idea. PJG,FPL and GC provided methodological support and critically reviewed the manuscript. All authors reviewed and contributed to the manuscript preparation.
Competing interests None declared.
Ethics approval Our Lady’s Children’s Hospital Crumlin, Dublin, Ireland and Children’s University Hospital, Dublin, Ireland.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it was first published. Some typos in the Ethics and Dissemination statement have been corrected.